When my daughter, Emily, and I started writing this blog in the spring of 2020, we did not anticipate that almost three years later, there would still be no end in sight for this pandemic. As we begin a new year, we wish we had better news, but the data continues to tell a grim story, and, as our long-time readers know, we always ground our outlook in the numbers.
In the United States, from March 2020 to December 31, 2021, we had 55,696,500 SARS CoV-2 infections and 846,905 deaths (66 infections per death). In the last 12 months we have had an additional 46,813,072 new infections and an additional 271,051 deaths (173 infections per death). That’s an average of 742 deaths per day. The majority of these deaths were in people over the age of 65, and all of them were preventable. In November 2022, KFF reported that COVID-19 was still the number 3 cause of death in the United States. It’s also worth noting that the number one cause of death, cardiovascular disease, is a known complication of COVID.
In late December 2021 the FDA approved both oral Paxlovid and oral Molnupiravir for outpatient treatment of SARS-CoV-2 with distribution beginning in January 2022. Unfortunately, all of the mask mandates were removed by individual states in 2022, and despite President Biden’s vow to institute a federal mask mandate during his 2020 campaign, the President and his administration adopted a decidedly anti-mask policy this year. CDC Director Rochelle Walensky even went so far as to describe masks as “the scarlet letter of this pandemic.” This irresponsible public health messaging has led to thousands of infections and deaths that could have been otherwise prevented by responsible mask wearing. We continue to urge our patients to protect themselves and others by wearing an N95 (or better) mask in public.
This year, multiple new Omicron variants BA.1, BA.2, BA.4, and BA.5 assaulted the world’s population of humans and other animals. By the time multiple companies made and tested Omicron BA.1 vaccines, BA.1 was no longer the dominant variant; in fact, it was no longer present. On August 31, 2022, the FDA allowed rapid introduction of an Omicron BA.5 bivalent vaccine. However, this has had no effect on new immune evading BQ variants. In December the first highly infectious recombinant variant, XBB, began spreading around the world. An additional variant, XBB.1.5, is now rapidly spreading across the country and the world causing increased numbers of hospitalizations and critically ill patients in the USA.
At the same time, we have had outbreaks and deaths from Influenza A H3N2 and RSV. Travel and lack of masking and social distancing have exacerbated the spread of these viruses. In addition, Mpox virus outbreaks occurred nationwide, a measles outbreak began in Ohio in unvaccinated children, and several cases of polio in New York were reported.
Part of why the United States’ vaccine-only approach to COVID-19 is so dangerous is that SARS-CoV-2 mutates, evading immune protection, and spreads more quickly than anyone can make, get approved, and distribute new vaccines. The Omicron BQ.1.1 variant is now being rapidly replaced by XBB.1.5. As an example, at D4 Labs, we designed, manufactured and packaged a new vaccine for Omicron BQ.1.1 in 6 weeks. Minimal animal testing, IRB approval, human testing, and expedited FDA approval under an EUA would probably require at least another 6 months. Even if we skipped or delayed animal testing, obtained IRB approval, and internally did a standard two-dose immunogenicity study in 20 humans using IgG antibody to the RBD of SARS-CoV-2 as the surrogate marker for protection, it would still take three months in our in-house human testing and assay facility to complete the study. This approach would probably not be acceptable to the FDA for even EUA approval but might be attempted in individual states. The timely production and distribution of any new vaccine against any new SARS-CoV-2 mutant will be difficult to accomplish by any company using the current regulatory framework for approval of vaccines in the United States. Using XBB.1.5 as an example, it is responsible for over 40% of the infections in the United States in the last 28 days. Vaccines would have to be designed, manufactured, and distributed in less than four weeks to stop an outbreak of a virulent, highly-infectious respiratory pathogen. Considerable thought needs to be entertained on how to accomplish this task rapidly.
Sadly, we do not see things improving in 2023 for respiratory virus control in the United States unless people wear high quality masks (N95 or better) and practice social distancing again. Continued infection and death increases are expected in the next eight weeks with 113 million people expected to travel during the holiday season, schools reopening on January 2, and people returning to work in poorly ventilated spaces.
Here are our 14-day moving average determinations for SARS-CoV-2 for the United States. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
After Delays, CDC Discloses XBB.1.5 Variant Data
On 12/31/22 the CDC estimates that BA.5 accounted for 3.7% of infections (a 49.6% point drop from its peak), BQ.1 accounted for 18.3% (a 12.4% point drop decrease from its peak on 12/17/22), BQ.1.1 accounted for 26.9% (a 11.5% point drop from its peak on 12/17/22), BA.4.6 accounted for 0.3%, BF.7 accounted for 2.1% of infections, BN.1 accounted for 2.4% of isolates,andBA.2.75.2 accounted for 0.1%. XBB is 3.6% of isolates, XBB.1.5 is 40.5% of isolates, BA.5.2.6 is 0.6% of isolates, and BF.11 0.3% of isolates. In the week ending December 31, 2022, BQ isolates accounted for 45.2% of isolates (a 23.9% point decrease in infections caused by these BQ variants since 12/17/22).
CDC
BQ.1.1 has five spike mutations that are different from BA.5. Four of these mutations allow escape from immunity from monoclonal antibodies, any prior infection (including Omicron BA.5), or any vaccine to include the bivalent Omicron BA.5 vaccine. Infections are still occurring in our clinic in patients that received the Omicron BA.5 bivalent vaccine. The XBB recombinant isolate XBB.1.5 has rapidly become the dominant infection in the USA. It took 28 days to become the cause of 40% of infections in the USA and it now causes over 70% of infections in Regions 1 and 2.
XBB.1.5 Proportion of Sequenced Isolates in the USA
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
SARS-CoV-2 infections per day in the United States have decreased for the fourth time in 12 weeks; however, there is still widespread underreporting by states, a failure to capture positive home tests, and a decreased PCR screening program in most states. Deaths per day in the United States have decreased by 81 deaths per day; however, many states are not reporting deaths in a timely manner. The number of infections per day has decreased by 8,524. The CDC estimates that BA.5 accounted for 62.2% (a 17% drop from 10/7/22), BQ.1 accounted for 9.4%, BQ.1.1 accounted for 7.2%, BA.4.6 accounted for 11.3%, BF.7 accounted for 6.7%, BA.2.75 accounted for 1.6%, BA.2.27.2 accounted for 1.3%, and BA.4 accounted for 0.4%, in the week ending October 22.
CDCCDC
The total percentage of BQ variant infections in the region that includes New York and New Jersey is 28.4%.
CDC
The total percentage of BQ variant infections in the region that includes Pennsylvania, Delaware, Maryland, West Virginia, and Virginia is 17.8%.
CDC
The total percentage of BQ variant infections in the region that includes California, Nevada, Arizona, and Hawaii is 13.6%.
Data on the rapid spread of a dangerous variant category, the BQ variants, was withheld by the CDC in their weekly reports until last week. The data on BQ.1 and BQ.1.1, the last being a variant with five significant spike protein mutations leading to escape from immunity from prior infections or vaccination. In addition, our monoclonal antibody therapies do not work for these isolates. Infections and hospitalizations in New York are rapidly increasing, secondary to BQ variants. We can expect this pattern to continue in many states, since New York has been a harbinger of things to come throughout the pandemic.
These emerging BQ variants are descendants of BA.5. It’s troubling that, despite the availability of a BA.5 bivalent SARS-CoV-2 vaccine, few people are getting vaccinated. As of October 19, the CDC reports that 19.4 million people have received the bivalent vaccine. That’s only 8.5% of people who received the primary series and 5% of the overall population.
There has been no new UK Health Security Agency Technical Briefing since October 7. The October 7 Technical Briefing says, “From UK data, BQ.X, BA.2.75.2 and BF.7 are the most concerning variants in terms of both growth and neutralisation data at present; there is also supportive animal model data for BA.2.75.”
Variant
Sublineage of
Spike Mutations
Global Sequences
UK Sequences
BF.7
BA.5.2.1
R346T
9,809 (1,752 from Belgium)
663
BQ.1.1
BA.5
N460KK444TR346T
326(20 countries)
60
BJ.1
BA.5
13 non- synonymous spike mutations, 7 in RBD and including4 predicted immune escape locations
123 (10 countries, most cases in India)
1
BS.1
BA.2.3.2
R346TL452RN460KG476S
25 (15 from Japan)
0
Data from UK Health Security Agency
In Monterey County, as of 10/22/22, 2.1% of 0-4 year-olds and 40.1% of 5-11 year-olds have received the first two doses of vaccine, while 73.3% of 12-17 year-olds have received two doses. Only 54.1% of Monterey County residents have received a third dose of the vaccine. The Monterey County Health Department does not publish data on how many residents have received the new BA.5 bivalent booster vaccine. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. All Monterey County residents should get up to date on COVID-19 vaccinations, including the bivalent BA.5 booster, as soon as possible.
Monterey County Health Department
On 10/21/22, the United States had 19,652 documented new infections. There were also 190 deaths. Thirty-four states did not report their infections, and 36 states didn’t report their deaths. In the United States the number of hospitalized patients has decreased slightly (-1% compared to the previous 14 days) in many areas and was 26,810 on October 22. On 10/21/22 there were 2,707 patients who are seriously or critically ill; that number was 2,753 two weeks ago. The number of critically ill patients has decreased only by 47 in the last 14 days, while at least 4,951 new deaths occurred. The number of critically ill patients has decreased for the fifth time in twenty-nine 14-day periods. Patients are still dying each day (average 354/day). Omicron BA.4, BA.4.6, BA.5, and BF.7 variants are still causing infections. A new variant BQ.1.1, descended from Omicron BA.5, is causing increasing numbers of infections and hospitalizations in New York. In Singapore a different Omicron BA.2 variant, XBB, is causing rapidly increasing infections. Past infections with a BA.1, BA.2 or BA.5 variants will not prevent infections with any of the newer variants.
As of 10/21/22, we have had 1,092,606 deaths and 99,055,537 SARS-CoV-2 infections in the United States. We have had 532,369 new infections in the last 14 days. We are adding an average of 266,185 new infections every seven days. For the pandemic in the United States we are averaging one death for every 90.65 infections or over 11,030 deaths for each one million infections. As of 10/21/22, thirty-eight states have had greater than 500,000 total infections, and 38 states have had greater than 5,000 total deaths. Forty-six states have had greater than 2,000 deaths, and 43 states have greater than 2,000 deaths per million population. Seven states have over 4,000 deaths per million population: Mississippi (4,350), Arizona (4,330), Alabama (4,186), West Virginia (4,178), New Mexico (4,111), Tennessee (4,103) and Arkansas (4,114). . Eighteen states (Alabama, Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Seven states have had greater than 40,000 deaths: Florida (82,065 deaths), Texas (91,584 deaths), New York (72,694 deaths), Pennsylvania (47,582 deaths), Georgia (40,552 deaths), Ohio (40,111 deaths) and California (96,721 deaths, 20th most deaths in the world).
On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. Since 11/20/20 (23 months), there were 825,605 new deaths from SARS-CoV-2. For nineteen of those months, vaccines have been available to all adults. During these eighteen months, 520,509 people have died of SARS-CoV-2 infections. Most of the hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 10/21/22, California was ranked 33rd in the USA in infection percentage at 28.65%. In California, 24.68% of people were infected in the last 19 months. As of 10/21/22, 24 states have had greater than 30% of their population infected. Fifty states have greater than 20% of their population infected.
Worldwide, average deaths per day are 1,569 for the last 14 days, which is a 97 deaths-per-day increase over the previous 14 days. The United States accounts for 22.56% (354 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 310,532. The United States accounts for 12.04% of those infections (or 37,384 infections per day).
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Merck has developed the oral drug Molnupiravir, which induces RNA mutagenesis by viral RNA-dependent RNA polymerase of SARS-CoV-2 and other viruses. According to Kabinger et al, “Viral RNA-dependent RNA polymerase uses the active form of Molnupiravir, β-D-N4-hydroxycytidine triphosphate, as a substrate instead of cytidine triphosphate or uridine triphosphate. When the RNA-dependent RNA polymerase uses the resulting RNA as a template, β-D-N4-hydroxycytidine triphosphate directs incorporation of either guanine or adenine, leading to mutated (viral) RNA products. Analysis of RNA-dependent RNA polymerase–RNA complexes that contain mutagenesis products has demonstrated that β-D-N4-hydroxycytidine (the active form ofMolnupiravir) can form stable base pairs with either guanine or adenine in RNA-dependent RNA polymerase explaining how the polymerase escapes proofreading and synthesizes mutated RNA” (quotation modified for clarity). The results of the phase 3 trial of Molnupiravir were published in the NEJM article “Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients” by Angélica Jayk Bernal, M.D. et al. (December 16, 2021 DOI: 10.1056/NEJMoa2116044). In this phase 3 study in the Molnupiravir group, 28 patients were hospitalized and one death occurred. In the placebo group, 53 patients were hospitalized and 9 died. Overall, 47% of hospitalizations and deaths were prevented by Molnupiravir. If you do a post hoc analysis and just look at deaths,Molnupiravir would prevent 89% of deaths. An Emergency Use Authorization by the FDA for Molnupiravir was approved on 12/24/21.The dose of Molnupiravir approved is four 200 mg capsules orally twice a day for five days. Diarrhea is reportedly a side effect in two percent of patients. I treated my first patient with Molnupiravir on 1/28/22. Currently more Molnupiravir is available weekly in the United States than PAXLOVID™ (see chart below; data from PHE.gov). Locally Molnupiravir is still available at CVS in Monterey (Fremont Blvd.; phone number: 831-375-5135) and CVS in Salinas (East Alisal Street; phone number 831-424-0026).
28, p740–746 (2021)with four 200 mg capsules orally twice a day for five dayfour 200 mg capsules orally twice a day for five daysIntravenous Drug Treatment for non-hospitalized SARS-CoV-2 Infected Patient
FDA-Approved Intravenous Monoclonal Antibody Treatment for Non-Hospitalized SARS-CoV-2 Patients
Bebtelovimab is a monoclonal antibody treatment for mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death, and for whom alternative COVID-19 treatment options approved or authorized by FDA are not accessible or clinically appropriate. The authorized dose of bebtelovimab is 175 mg, given as an intravenous injection over at least 30 seconds. The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for this drug on 2/11/22. Bebtelovimab is a human antibody that demonstrates neutralization against the Omicron variants and is available in every state and many hospitals and some clinics. If you are planning on using a monoclonal antibody to treat a SARS-CoV-2 infection, currently only bebtelovimab has activity against all Omicron variants, including BA.4.6. Researchers at Columbia University recently reported that “The loss of activity of tixagevimab and cilgavimab [components of Evusheld] against BA.4.6 leaves us with bebtelovimab as the only therapeutic mAb that has retained potent activity against all circulating forms of SARS-CoV-2.” For this reason, we no longer recommend Evusheld for immunocompromised patients with Omicron infections.
An examination of the three variants that Wang et al identified as capable of immune escape in patients who receive the two monoclonal antibodies that are contained in Evusheld reveals that all three variants have a mutation in the spike protein at position 346. The changes substitute an uncharged amino acid— threonine (T), serine (S), or isoleucine (I)—for a positively-charged amino acid, arginine. This just goes to show that a single point mutation in the spike protein can render a monoclonal antibody treatment ineffective. Policy makers should keep in mind that the only way to prevent new drug-resistant variants like BA.4.6 from emerging is to prevent transmission of SARS-CoV-2 in the first place, using non-pharmaceutical interventions. The lack of use of N95 masks, with impending winter and influenza outbreaks, on top of COVID-19, is not wise public health and infectious disease policy. If we don’t make effective use of the non-pharmaceutical interventions available to us (masks, ventilation, social distancing), then the pharmaceutical interventions we have will all eventually be useless.
Two virologists collaborated on Twitter to create the figure below, which Professor Johnson titled “Convergent Evolution on Steroids.” It shows the key mutations present in many of the currently-circulating Omicron subvariants and demonstrates that mutation at site 346 is becoming more and more common. This means that even if prevalence of BA.4.6 wanes, we are still likely to have drug resistance issues with other newer variants.
From Professor Marc Johnson, molecular virologist @SolidEvidence on Twitter and Daniele Focosi, M.D., Ph.D. @dfocosi on Twitter
Watching World Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 10/21/22
New Infections on 10/21/22
Total Deaths
New Deaths on 10/21/22
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate
Currently in Lockdown
World
632,432,678(4,347,443 new infections in 14 days).
349,351
6,581,530(21,965 new deaths in last 14 days)
1,189
8.11%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1 (USA)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BF.7BJ.1XBBBQ.1BQ.1.1BS.1
No
No
USA
99,055,537(ranked #1) 532,369 new infections in the last 14 days.
19,652(ranked #7) 34 states failed to report infections on 10/21/22.
1,092,606(ranked #1) 4,951 new deaths reported in the last 14 days.
190 36 states failed to report deaths on 10/21/22.
29.58%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)
No
No
Brazil
34,822,174(ranked #4) 64,917 new infections in the last 14 days.
3,400
687,581(ranked #2; 732 new deaths in 14 days)
37
16.16%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
India
44,640,748(ranked #2); 31,991 new infections in 2 weeks.
2,112
528,957(ranked #3) 199 new deaths in 2 weeks.
4
3.17%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India)
No
No
United Kingdom
23,855,522(ranked #7) 120,249 new infections in 2 weeks.
–
192,682 (ranked #7) 1,794 new deaths in 2 weeks
–
34.82%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)
No
No
California, USA
11,332,345(ranked #14 in the world; 39,798 new infections in the last 14 days).
998
96,721 (ranked #20 in world) 303 new deaths in the last 14 days
14
28.65%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)
No
No
Mexico
7,106018(ranked #19) 4,587 new infections in 14 days).
453
330,321(ranked #5)181 new deaths in 14 days)
15
5.40%
No
No
South Africa
4,025,375(ranked #37; 4,587 new infections in 14 days).
416
102,257 (ranked #18) 63 new deaths in 14 days)
11
6.62%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
Canada
4,314,718(ranked #33) 43,827 new infections in 14 days).
3,067
46,025(ranked #25)631 new deaths in the last 14 days
49
11.23%
No
No
Poland
6,333,591 (ranked #21;22,629 new infections in 14 days).
1,170
118,015 (ranked #15)272 new deaths in the last 14 days
24
16.78%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3
No
No
Russia
21,354,915(ranked #10), 190,973 new infections in 14 days).
9,761 (ranked #8)
389,359(ranked #4)1,368 new deaths in 14 days
93
14.64%
No
No
Peru
4,152,019(ranked #32, 3,858 new infections in 14 days).
314
216,877(ranked #6) 177 new deaths in the last 14 days
–
12.32%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Iran
7,555,694(ranked #17; 4,672 new infections in last 14 days)
139
144,540(ranked #12) 69 new deaths in the last 14 days
4
8.78%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Spain
13,488,015(ranked #12; 46,047 new infections in 14 days).
3,630
114,858 (ranked #16)390 new deaths in 14 days
31
28.87%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)
No
No
France
36,524,605 (ranked #3; 758,248 new infections in the last 14 days).
49,087 (ranked #2)
156,337 (ranked #10)803 new deaths in 14 days.
81
55.69% a 2.17% increase in 14 days.
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant
No
No
Germany
35,172,693(ranked #4; 1,224,661 new infections in 14 days.)
49,087 (ranked #2)
152,482 (ranked #11)1,947 new deaths in 14 days
204
41.93% 1.71% increase in 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
South Korea
25,244,255 (ranked #6 310,499 new infections in 14 days).
24,709(ranked #8)
28,952 (ranked #37) 338 new deaths in 14 days
30
49.18%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Vietnam
11,496,354 (ranked #13; 10,933 new infections in 14 days).
582
43,159 (ranked #26)
–
11.61%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Netherlands
8,494,705 (ranked #16; 33,354 new infections in 14 days).
952
22,683 (ranked #41)
5
49.35%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Denmark
3,131,149(ranked #40) 12,835 new infections in 14 days.
652
7,248 (ranked #79 126 new deaths in the last 14 days)
13
53.66%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Taiwan
7,379,205(ranked #18)569,950 new infections in 14 days
37,265 (ranked #3)
12,206 (ranked #59 937 new deaths in the last 14 days)
78
30.89% 2.53% of population has been infected in the last 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Japan
21,926,231(ranked #9)463,493 new infections in the last 14 days
31,593(ranked #5)
46,152(ranked #25) 831 new deaths in the last 14 days
67
17.45%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)BA.2*BA.5*
No
No
What Our Team Is Reading This Week
Effectiveness of Monovalent mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States — IVY Network, 18 States, December 26, 2021–August 31, 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7142a3.htm
“Three-dose monovalent mRNA VE estimates against COVID-19–associated hospitalization decreased with time since vaccination. Three-dose VE during the BA.1/BA.2 and BA.4/BA.5 periods was 79% and 60%, respectively, during the initial 120 days after the third dose and decreased to 41% and 29%, respectively, after 120 days from vaccination.”
Saliva antibody-fingerprint of reactivated latent viruses after mild/asymptomatic COVID-19 is unique in patients with myalgic-encephalomyelitis/chronic fatigue syndrome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.949787
Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: an observational study (The Lancet) https://doi.org/10.1016/S0140-6736(22)01586-0
Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients (Ear, Nose, and Throat Journal) https://doi.org/10.1177/01455613221123737
Note: This is a frightening paper and if the conclusions are accurate humans in general are in trouble. From other papers the facts that HERV-M and EBV are activated by SARS-CoV-2 infection does not bode well for humans moving forward.
SARS-CoV-2 Spike protein promotes vWF secretion and thrombosis via endothelial cytoskeleton-associated protein 4 (CKAP4) (Signal Transduction and Targeted Therapy) https://www.nature.com/articles/s41392-022-01183-9
VACCINE INFORMATION FACT SHEET FOR RECIPIENTS AND CAREGIVERS ABOUT COMIRNATY (COVID-19 VACCINE, mRNA), THE PFIZER-BIONTECH COVID-19 VACCINE, AND THE PFIZER-BIONTECH COVID-19 VACCINE BIVALENT (ORIGINAL AND OMICRON BA.4/BA.5) TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19) FOR USE IN INDIVIDUALS 12 YEARS OF AGE AND OLDER https://labeling.pfizer.com/ShowLabeling.aspx?id=14472
SARS-CoV-2 variants of concern: spike protein mutational analysis and epitope for broad neutralization (Nature Communications) https://doi.org/10.1038/s41467-022-32262-8
Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients (The Lancet Psychiatry) https://doi.org/10.1016/S2215-0366(22)00260-7
An Antibody from Single Human VH-rearranging Mouse Neutralizes All SARS-CoV-2 Variants Through BA.5 by Inhibiting Membrane Fusion (Science Immunology) https://doi.org/10.1126/sciimmunol.add5446
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic (Preprint) https://doi.org/10.1101/2022.08.03.22278363
SARS-CoV-2 Brain Regional Detection, Histopathology, Gene Expression, and Immunomodulatory Changes in Decedents with COVID-19 (Journal of Neuropathology and Experimental Neurology) https://doi.org/10.1093/jnen/nlac056
Notes from the Field: Increase in Pediatric Intracranial Infections During the COVID-19 Pandemic — Eight Pediatric Hospitals, United States, March 2020–March 2022 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7131a4
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
SARS-CoV-2 infections are accelerating at a rapid rate in the United States and many other countries including the United Kingdom, France, Germany, and Italy. This is caused by the Delta variants and the Omicron variant of concern. Omicron is at least four times as infectious as the already highly infectious Delta variants. UK scientists have found that the household secondary attack rate for Omicron is 21.6%, compared to 10.7% with Delta, meaning people infected with Omicron are twice as likely to infect household members as they would be if infected with Delta. They also estimate a “three- to eight-fold increased risk of reinfection with the Omicron variant.”
I would expect the Omicron variant to continue to mutate just like Delta. There are already two Omicron variants, BA.1 and BA.2. We expect to see additional Omicron variants as this isolate spreads rapidly around the USA and the World. As of 12/22/21 the Omicron variant, which was first seen in South Africa on 11/08/21, is now in all 50 states, Puerto Rico and the District of Columbia. It has also been identified in at least 92 countries.
Omicron has mutations which decrease the effectiveness of current vaccines and monoclonal antibodies. The effectiveness of the new Pfizer drug, PAXLOVIDTM, should not be compromised by any of the current mutations in Omicron or Delta variants. Pfizer completed their filing with the FDA on 11/15/21. The FDA approved PAXLOVIDTM on December 22 , 2021.The FDA approved Merck’s drug Molnupiravir on December 23, 2021. On 12/23/21 CVS announced by fax it was selected by the Government to distribute oral PAXLOVIDTM and Molnupiravir. On 12/27/21 another fax from CVS listed which CVS pharmacies in California would have these drugs. Monterey County covers 3,771 square miles with a population of 434,061. Three CVS pharmacies in Monterey, Salinas, and Soledad are the only listed pharmacies in our county. Fresno County covers 6,011 square miles with a population of 999,101. Four CVS pharmacies in Fresno County are the only listed pharmacies.
In the PAXLOVIDTM study no deaths occurred in the treatment group. We are averaging over 1,000 deaths per day in the USA and Russia. If PAXLOVIDTM is widely available and just 90% effective in preventing deaths, each country could prevent over 900 deaths per day. If Molnupiravir is widely available and just 50% effective in preventing deaths and hospitalizations, each country could prevent over 450 deaths per day. If drug distribution doesn’t occur rapidly then that’s at least 27,000 additional deaths in each country that could have been prevented in the next 30 days. For now only masking (N95 rated masks, please!), social distancing and vaccination will have any effect on these variants. Furthermore, we do not believe that a 5-day quarantine or isolation period is sufficient for any COVID-19 infection. The Taiwanese CDC agrees with both our recommendations on quarantine period and masking. In fact, the Taiwanese CDC has recommended N95 masking since the beginning of the pandemic (and made these masks universally available to their population). Taiwan has one of the lowest death rates per million during the course of the pandemic (see graph below).
In the United States as of 12/31/21, SARS-CoV-2 deaths have increased for the third time in seven 14-day periods. There were 113 more deaths per day than in the last 14-day period. In the last 14 days, the number of infections has increased by 160,999 infections per day compared to the preceding 14-day period. Our infections per day have increased for the fourth time over the last 14 weeks.With travel and multiple holidays and events occurring in the next 60 days, we expect the infections to continue to increase. Unless people get vaccinated and get their third dose of the vaccine, we will see further spread of Delta variants like AY4.2 and an increase in deaths particularly in people with risk factors and over the age of 55. Anyone over the age of 5 years can now get vaccinated in the United States at no cost. This should get done immediately.
A new variant, B.1.1.529 (Omicron), was first seen in South Africa on 11/8/21 with multiple new mutations, deletions and an insertion that was causing a doubling of new infections every 1.3 days in Gauteng, South Africa. In just 54 days, as of 12/31/21, Omicron has been found in 70 countries and 40 states in the United States. Unlike Delta variants in South Africa, Omicron is infecting and hospitalizing patients in all age groups but particularly children under five years of age and adults greater than 60 years of age. Increased vaccinations, vaccines against new mutants, drugs against 3C-like protease, increased mask usage and social distancing, which are part of the Biden SARS-CoV-2 plan, are all necessary to continue to stop further spread of mutants and reduce infections, hospitalizations, and deaths. Per CDC data ending in 12/25/21, the Delta variant still accounts for 41.1% of new infections in the United States, while Omicron accounts for 58.6%. It’s worth noting that in the last 30 days, according to GISAID, the United States has only sequenced 2.23% of cases.
On 12/31/21, the United States had 443,677 new infections with twenty-two states and the District of Columbia failing to report. There were also 716 deaths(with 27 other states failing to report deaths). Florida continues to consistently under-report daily infections and deaths. The number of hospitalized patients has been increasing in many areas, and now 15,602 patients are seriously or critically ill; that number was 13,714 two weeks ago. The number of critically ill patients has increased by 1,888 in the last 14 days, while at least 18,603 new deaths occurred. The number of critically ill patients has increased for the third time in twelve 14-day periods and a large number of patients are still dying each day (average 1,329/day).
As of 12/31/21, we have had 846,905 deaths and 55,696,500 SARS-CoV-2 infections in the United States. We have had 4,186,219 new infections in the last 14 days. We are adding an average of 2,093,110 infections every seven days. For the pandemic in the United States we are averaging one death for every 65.3 infections reported or over 15,206 deaths for each one million infections. As of 12/31/21, thirty-four states have had greater than 500,000 total infections, and 36 states have had greater than 5,000 total deaths. Thirteen states (Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York, and California) have had greater than 60,000 deaths.
On 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota, 9.18% of the population was infected (ranked #1), and in South Dakota, 8.03% of the population was infected (ranked #2). As of 12/17/21, in the United States, 15.45% of the population has had a documented SARS-CoV-2 infection. In the last 13 months, 11.75% of our country became infected with SARS-CoV-2. On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. In the last 13 months, there were 604,574 new deaths from SARS-CoV-2. For ten of those months, vaccines have been available to all adults. During these ten months, 242,232 people have died of SARS-CoV-2 infections. Many of these hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 12/31/21, California was ranked 43rd in infection percentage at 13.57% and10.04% of Californians were infected in the last 13 months. As of 12/31/21 42 states have greater than 16% of their population infected. Five states have greater than 20% of their population, which is not a list that you’d like to be on in 2021. North Dakota was at 22.85% (ranked #1), Rhode Island was at 21.81% (ranked #2), Tennessee was at 20,89% (ranked #3), Alaska was at 20.72% (ranked #4) and South Dakota was at 20.25% (ranked #5) of their population infected. Forty-four states and the District of Columbia now have greater than 12% of their population infected. Only one state has less than 8% of their population infected: Hawaii (7.97%). Hawaii and the US Virgin Islands still remain the safest places in the United States. Hawaii had its first patient with an Omicron (B.1.1.529) SARS-CoV-2 infection four weeks ago.
The table below shows that if we rank the US states with the highest death rates per million population within the world rankings, we see that Mississippi has the seventh highest COVID-19 deaths per million in the world. New Jersey is 8th, New York, Louisiana and Arizona would be tied at the 9th highest number of deaths per million in the world, followed by Arkansa at 12th, Arizona, Massachusetts and Rhode Island tied at 13th and Florida at 14th. The United States as a whole ranks 21st in the world for deaths per million population (2,559 deaths per million). California ranks 36th in the USA (and 37th in the world). If we look at the death rates per million in South Korea (108), Iceland (107), Japan (146), and Israel (884), they suggest that treatment outcomes are somehow different in these four countries. The same phenomenon can be seen in Scandinavia, where the death rate in Sweden is 1,498 per million, compared to 238 per million in Norway and 282 per million in Finland. The United States should take a closer look at how countries with low death rates (like South Korea, Iceland, Japan, Finland, and Norway) are preventing COVID-19 infections and treating COVID-19 patients.
State or Country
COVID-19 Deaths per million population
Rank in USA
Ranked within World
Mississippi
3,511
1st
7th
New Jersey
3,269
4th
8th
Louisiana
3,224
5th
9th tied
New York
3,085
6th
9th tied
Alabama
3,356
2nd
9th tied
Arizona
3,329
3rd
9th tied
Massachusetts
2,941
11th
13th tied
Rhode Island
2,894
15th
13th tied
Arkansas
3,031
8th
12th
Florida
2,909
13th
14th
California
1,920
35th
36th
USA
2,559
21st
Peru
6,022
1st
Bosnia-Herzegovina
4,136
3rd
North Macedonia
3,821
6th
Hungary
4,072
4th
Montenegro
3,821
5th
Bulgaria
4,506
2nd
Gibraltar
2,969
12th
Czechia
3,367
8th
Brazil
2,882
14th
San Marino
2,936
13th
Georgia
3,261
8th
Sweden
1,498
57th
Israel
884
87th
Canada
793
94th
Finland
282
135th
Norway
238
138th
Japan
146
154th
Iceland
107
164th
South Korea
108
163rd
A New Drug for SARS-CoV-2 Treatment
Pfizer has developed a reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, called Compound 6, is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. I had anticipated that the drug would be approved in the next 7 days. In my opinion, this agent, if approved, will markedly alter the course of every coronavirus infection throughout the world.
The Threat of SARS-CoV-2 Variants
In response to the need for “easy-to-pronounce and non-stigmatising labels,” at the end of May, the World Health Organization assigned a letter from the Greek alphabet to each SARS-CoV-2 variant. GISAID, Nextstrain, and Pango will continue to use the previously established nomenclature. For our purposes, we’ll be referring to each variant by both its Greek alphabet letter and the Pango nomenclature.
The WHO has sorted variants into two categories: Variants of Concern (VOC) and Variants of Interest (VOI). The criteria for Variants of Concern are as follows:
Increase in transmissibility or detrimental change in COVID-19 epidemiology; or
Increase in virulence or change in clinical disease presentation; or
Decrease in effectiveness of public health and social measures or available diagnostics, vaccines, therapeutics.
The WHO categorizes the following five variants as Variants of Concern (VOC):
Source: World Health Organization
The criteria for Variants of Interest (VOI) are as follows:
has been identified to cause community transmission/multiple COVID-19 cases/clusters, or has been detected in multiple countries; OR
is otherwise assessed to be a VOI by WHO in consultation with the WHO SARS-CoV-2 Virus Evolution Working Group.
The WHO categorizes the following six variants as Variants of Interest (VOI):
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 12/31/21
New Infections on 12/31/21
Total Deaths
New Deaths on 12/31/21
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate?
Currently in Lockdown?
World
288,467,234(14,507,440 new infections in 14 days).
1,638,236
5,452,992(92,274 new deaths in last 14 days)
5,944
3.70%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 (South Africa November 2021)B.1.640 (Congo/France)
No
No
USA
55,510,281 (ranked #1) 4,182,219 new infections in the last 14 days)
443,677 (ranked #1)
846,905 (ranked #1)20,186 new deaths in the last 14 days)
716
16.68%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 (South Africa November 2021)B.1.640 (Congo/France)
No
No
Brazil
22,287,521(ranked #3)
10,282
619,109(ranked #2)
85
10.37%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 (South Africa November 2021)
No
No
India
34,861,579(ranked #2)
22,775
481,486(ranked #3)
406
2.49%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 (South Africa November 2021)B.1.640 (Congo/France)
No
No
United Kingdom
12,937,886(ranked #4; was #6 eighteen weeks ago)
189.846
148,624 (ranked #7 in world)
203
18.90%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 (South Africa November 2021)B.1.640 (Congo/France)
No
No
California, USA
5,363,784(ranked #13 in world)
39,043
78,739 (ranked #20 in world)
49
13.67%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 (South Africa November 2021)
No
No
Mexico
3,969,686(ranked #16)
8,024
299,285(ranked #5)
153
3.03%
B2 lineageAlpha/B.1.1.7 (UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
South Africa
3,276,529(ranked #18)
Exponential growth of Omicron occurring in South Africa. Children under 5 are infected.Quadrupling of daily infections in last four days.
11,754 on 12/31/21
16,055on 12/3/21,11,535 on 12/2/21,8,561on 12/1/21,4,373on 11/30/21,789on 11/19/21339on 11/5/21
91,145 (ranked #17)
84
5.72%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 (South Africa, November 2021)B.1.640 (Congo/France)
No
No
Canada
2,183,527(ranked #26)
41,217
30,319(ranked #29)
12
4.87%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)B.1.640 (Congo/France)
No
No
Poland
4,108,215(ranked #15)
13,613
97,054 (ranked #15)
638
10.87%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Turkey
9,482,550(ranked #7)
40,786
82,361 (ranked #19)
163
11.06%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Russia
10,499,982(ranked #5)
20,638
308,860(ranked #4 in world)
912
7.19%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)R1(Japan) B.1.640 (Congo/France)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Argentina
5,654,468(ranked #12)
47,663
117,169 (ranked #13 in world)
23
12.34%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gama/P.1 (Brazil)Delta/B.1.617.2 (India)Lambda/C.37 (Peru)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Colombia
5,157,440(ranked #13)
1,803
129,942 (ranked #11 in world)
41
9.97%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Epsilon/B.1.427 + B.1.429 (USA)*Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Peru
2,296,831(ranked #23)
4,577
202,690(ranked #6)
37
6.82%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Indonesia
4,262,720(ranked #14)
180
144,094 (ranked #8)
=6
1.53%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Eta/B.1.525 (Nigeria/UK)Theta/P.3 (Philippines) Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)B.1.640 (Congo/France)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Iran
6,194,401(ranked 10th; was 12th eighteen weeks ago)
1,703
131,606 (ranked #10)
34
7.23%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 (South Africa November 2021)
No
No
Spain
6,294,745(ranked 9th)
———-
89,405 (ranked #18)
——-
13.45%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 South Africa November 2021)B.1.640 (Congo/France)
Frequent Occurrence of SARS-CoV-2 Transmission among Non-close Contacts Exposed to COVID-19 Patients (Journal of Korean Medical Science) https://doi.org/10.3346/jkms.2021.36.e233
Characteristics and Clinical Outcomes of Children and Adolescents Aged <18 Years Hospitalized with COVID-19 — Six Hospitals, United States, July–August 2021 (MMWR) https://www.cdc.gov/mmwr/volumes/70/wr/mm705152a3.htm
Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: a meta-analysis (The Lancet) https://doi.org/10.1016/S2666-5247(21)00267-6
“Vaccination reduces the risk of delta variant infection and accelerates viral clearance. Nonetheless, fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts. Host–virus interactions early in infection may shape the entire viral trajectory.”
Pediatric COVID-19 Cases in Counties With and Without School Mask Requirements — United States, July 1–September 4, 2021 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7039e3
Association Between K–12 School Mask Policies and School-Associated COVID-19 Outbreaks — Maricopa and Pima Counties, Arizona, July–August 2021 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7039e1
Decreased Incidence of Infections Caused by Pathogens Transmitted Commonly Through Food During the COVID-19 Pandemic — Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2017–2020 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7038a4
Starr, T.N., Czudnochowski, N., Liu, Z. et al. SARS-CoV-2 RBD antibodies that maximize breadth and resistance to escape. Nature 597, 97–102 (2021). https://doi.org/10.1038/s41586-021-03807-6
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
In the United States, SARS-CoV-2 deaths have increased for the first time in five 14-day periods. There were 43 more deaths per day than in the last 14-day period. In the last 14 days, the number of infections has increased by 8,237 infections per day compared to the preceding 14-day period. Our infections per day have increased for the second time over the last 12 weeks. With travel and multiple holidays and events occurring in the next 60 days, I expect the infections to continue to increase. Unless people get vaccinated and get their third dose of the vaccine we will see further spread of Delta variants like AY4.2 and an increase in deaths particularly in people with risk factors and over the age of 55. Anyone over the age of 5 years can now get vaccinated in the United States at no cost. This should get done immediately.
A new variant, B.1.1.529 (Omicron), was first seen in South Africa on 11/8/21 with multiple new mutations, deletions and an insertion that is causing a doubling of new infections every 1.3 days in Gauteng, South Africa. In just 26 days, as of 12/03/21, Omicron has been found in 42 countries and 12 states in the United States.Unlike Delta variants in South Africa, Omicron is infecting and hospitalizing patients in all age groups but particularly children under five years of age and adults greater than 60 years of age. Increased vaccinations, vaccines against new mutants, drugs against 3C-like protease, increased mask usage and social distancing, which are part of the Biden SARS-CoV-2 plan, are all necessary to continue to stop further spread of mutants and reduce infections, hospitalizations, and deaths. The Delta variants still account for 99% of new infections in the United States. On 12/03/21, the United States had 147,434 new infections with one state failing to report (Iowa). There were also 1,352 deaths (with six other states failing to report deaths). Florida continues to consistently under-report daily infections and deaths. The number of hospitalized patients had been decreasing in many areas but now 13,714 patients are seriously or critically ill; that number was 11,767 two weeks ago. The number of critically ill patients has increased by 1,947 in the last 14 days, while at least 17,018 new deaths occurred. The number of critically ill patients has increased for the second time in eleven 14-day periods and a large number of patients are still dying each day (average 1,216/day).
As of 12/03/21, we have had 808,116 deaths and 49,378,049 SARS-CoV-2 infections in the United States. We have had 1,356,453 new infections in the last 14 days. We are adding an average of 678,227 infections every seven days. For the pandemic in the United States we are averaging one death for every 60.4 infections reported or over 16,533 deaths for each one million infections. As of 12/03/21, thirty-one states have had greater than 500,000 total infections, and 35 states have had greater than 5,000 total deaths. Eleven states (Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York, and California) have had greater than 50,000 deaths.
On 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota 9.18% of the population was infected (ranked #1), and in South Dakota 8.03% of the population was infected (ranked #2). As of 12/03/21, in the United States, 14.94% of the population has had a documented SARS-CoV-2 infection. In the last 12.5 months, over 11% of our country became infected with SARS-CoV-2. On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. In the last 12 months, there were 547,885 new deaths from SARS-CoV-2. For nearly nine of those months, vaccines have been available to all adults. During these nine months, 203,345 people have died of SARS-CoV-2 infections. Many of these hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 12/03/21, California was ranked 41st in infection percentage at 12.50% and9.74% of Californians were infected in the last 12 months. And now let’s look at the top 26 infected states (all greater than 16%, which is not a list that you’d like to be on in 2021. North Dakota was at 21.53% (ranked #1), Alaska was at 20.03% (ranked #2), Tennessee was at 19.37% (ranked #3), Wyoming 19.37% (ranked #4), South Dakota was at 19.02% (ranked #5), Utah at 18.77% (ranked #6), South Carolina was at 17.90% (ranked #10), Rhode Island was at 18.39% (ranked #7), Montana was at 17.98% (ranked #9), Iowa was at 18.08% (ranked #8), Florida was at 17.43% (ranked #14), Arkansas was at 17.63% (ranked #12), Kentucky was at 17.79% (ranked #11), Alabama was at 17.28% (ranked #16), Mississippi was at 17.32% (ranked #15), Idaho was at 17.27% (ranked #17), Arizona was at 17.43% (ranked #13) Oklahoma was at 16.94% (ranked #19), Louisiana was at 16.622% (ranked #21), Wisconsin was at 17.13% (ranked #18), West Virginia was at 16.66% (ranked #20), Indiana was at 16.61% (ranked#22), Kansas was at 16.28%(ranked #23), Minnesota was at 16.24% (ranked#25) and Nebraska at 16.22% of the population infected (ranked #2). Forty-two states now have greater than 12% of their population infected. Only one state has less than 7% of their population infected: Hawaii (6.21%). Hawaii, Vermont, and the US Virgin Islands still remain the safest places in the United States. Although Hawaii has just had its first patient with an Omicron (B.1.1.529) SARS-CoV-2 infection.
The table below shows that if we rank the US states with the highest death rates per million population within the world rankings, we see that Mississippi has the sixth highest COVID-19 deaths per million in the world. Alabama, New Jersey and Louisiana would be tied at the 7th highest number of deaths per million in the world, followed by Arizona, NewYork tied at 9th, Florida at 11th, Arkansas, Massachusetts and Rhode Island tied at 12th. The United States as a whole ranks 20th in the world for deaths per million population (2,390 deaths per million). California ranks 35th in the USA (and 36th in the world). If we look at the death rates per million in South Korea (73), Iceland (102), Japan (146), and Israel (879), they suggest that treatment outcomes are somehow different in these four countries. The same phenomenon can be seen in Scandinavia, where the death rate in Sweden is 1,486 per million, compared to 199 per million in Norway and 245 per million in Finland. The United States should take a closer look at how countries with low death rates (like South Korea, Iceland, Japan, Finland, and Norway) are preventing COVID-19 infections and treating COVID-19 patients.
State or Country
COVID-19 Deaths per million population
Rank in USA
Ranked within World
Mississippi
3,460
1st
6th
New Jersey
3,201
3rd
7th tied
Louisiana
3,189
4th
7th tied
New York
2,994
6th
9th tied
Alabama
3,298
2nd
7th tied
Arizona
3,077
5th
9th
Massachusetts
2,828
11th
12th tied
Rhode Island
2,776
12th
12th tied
Arkansas
2,883
8th
12th tied
Florida
2,870
9th
11th
California
1,898
35th
35th
USA
2,421
20th
Peru
5,988
1st
Bosnia-Herzegovina
3,902
3rd
North Macedonia
3,696
5th
Hungary
3,649
6th
Montenegro
3,696
4th
Bulgaria
4,185
2nd
Gibraltar
2,940
10th
Czechia
3,122
7th
Brazil
2,866
11th
San Marino
2,733
12th
Georgia
3,081
8th
Sweden
1,486
56th
Israel
879
86th
Canada
778
94th
Finland
245
136th
Norway
199
141st
Japan
146
153rd
Iceland
102
163rd
South Korea
73
169th
Data from Worldometers
A New Drug for SARS-CoV-2 Treatment
Pfizer has developed a reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, called Compound 6, is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. I would anticipate that the drug would be approved in the next 21 days. In my opinion, this agent, if approved, will markedly alter the course of every coronavirus infection throughout the world.
The Threat of SARS-CoV-2 Variants
In response to the need for “easy-to-pronounce and non-stigmatising labels,” at the end of May, the World Health Organization assigned a letter from the Greek alphabet to each SARS-CoV-2 variant. GISAID, Nextstrain, and Pango will continue to use the previously established nomenclature. For our purposes, we’ll be referring to each variant by both its Greek alphabet letter and the Pango nomenclature.
The WHO has sorted variants into two categories: Variants of Concern (VOC) and Variants of Interest (VOI). The criteria for Variants of Concern are as follows:
Increase in transmissibility or detrimental change in COVID-19 epidemiology; or
Increase in virulence or change in clinical disease presentation; or
Decrease in effectiveness of public health and social measures or available diagnostics, vaccines, therapeutics.
The WHO categorizes the following five variants as Variants of Concern (VOC):
Source: World Health Organization
The criteria for Variants of Interest (VOI) are as follows:
has been identified to cause community transmission/multiple COVID-19 cases/clusters, or has been detected in multiple countries; OR
is otherwise assessed to be a VOI by WHO in consultation with the WHO SARS-CoV-2 Virus Evolution Working Group.
The WHO categorizes the following six variants as Variants of Interest (VOI):
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 12/03/21
New Infections on 12/03/21
Total Deaths
New Deaths on 12/03/21
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate?
Currently in Lockdown?
World
265,161,705(8,234,681 new infections in 14 days; an increase of 1,142,190 infections from the preceding 14 days)
705,574
5,258,046(102,708 deaths in 14 days; an increase of 5,145 deaths from the preceding 14 days).
7,915
3.40%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 (South Africa November 2021)
No
No
USA
49,878,049 (ranked #1) 1,356,453 new infections in the last 14 days)
147,434 (ranked #1)
808,116 (ranked #1)17,018 new deaths in the last 14 days)
1,352
14.94%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 (South Africa November 2021)
No
No
Brazil
22,129,409(ranked #3)
10,627
615,454(ranked #2)
2,229
10.30%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 (South Africa November 2021)
No
No
India
34,624,360(ranked #2)
8,603
470,530(ranked #3)
415
2.47%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 (South Africa November 2021)
No
No
United Kingdom
10,349,647(ranked #4; was #6 fourteen weeks ago)
50,584
145,424 (ranked #7 in world)
143
15.17%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 (South Africa November 2021)
No
No
California, USA
4,978,179(ranked #14 in world)
8,547
75,013 (ranked #20 in world)
90
12.59%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 (South Africa November 2021)
No
No
Mexico
3,894,364(ranked #15)
3,146
294,715(ranked #4)
287
2.97%
B2 lineageAlpha/B.1.1.7 (UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
No
No
South Africa
3,004,203(ranked #18) Exponential growth of Omicron occurring in South Africa. Children under 5 are infected.Quadrupling of daily infections in last four days.
16,055on 12/3/21,11,535 on 12/2/21,8,561on 12/1/21,4,373on 11/30/21,789on 11/19/21339on 11/5/21
89,940
25
4.97%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 South Africa, November 2021)
No
No
Canada
1,802,359(ranked #26)
3,487
29,757
20
4.71%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 (South Africa November 2021)
Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: a meta-analysis (The Lancet) https://doi.org/10.1016/S2666-5247(21)00267-6
“Vaccination reduces the risk of delta variant infection and accelerates viral clearance. Nonetheless, fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts. Host–virus interactions early in infection may shape the entire viral trajectory.”
Pediatric COVID-19 Cases in Counties With and Without School Mask Requirements — United States, July 1–September 4, 2021 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7039e3
Association Between K–12 School Mask Policies and School-Associated COVID-19 Outbreaks — Maricopa and Pima Counties, Arizona, July–August 2021 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7039e1
Decreased Incidence of Infections Caused by Pathogens Transmitted Commonly Through Food During the COVID-19 Pandemic — Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2017–2020 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7038a4
Starr, T.N., Czudnochowski, N., Liu, Z. et al. SARS-CoV-2 RBD antibodies that maximize breadth and resistance to escape. Nature 597, 97–102 (2021). https://doi.org/10.1038/s41586-021-03807-6
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
In the United States, SARS-CoV-2 deaths have decreased for the eighth time in a 14-day period. There were 137 fewer deaths per day than in the last 14-day period. In the last 14 days, the number of infections has decreased by 12,293 infections per day.Our infections per day are still high, probablysecondary to SARS-CoV-2 mutants, to include the Alpha/B.1.1.7 isolate, the Iota/B.1.526 isolate, the Epsilon/B.1.427 + B.1.429 isolate, the Beta/B.1.351 isolate, the Gamma/P.1 and Zeta/P.2 isolates, and the new isolate, Deta/B.1.617+. I would predict that the opening of schools, places of worship, bars, restaurants, indoor dining and travel all will contribute to further spread of multiple SARS-CoV-2 mutants and rising numbers in infections, hospitalizations and deaths in the coming months. Increased traveling as well as summer vacations, and the July 4 holiday will all cause further increases. Vaccinations, increased mask usage and social distancing, which are a part of the Biden SARS-CoV-2 plan (day 136 of plan) will be necessary to stop spread of mutants and cause further reductions in infections, hospitalizations and deaths in the future. On 6/04/21, 16,925 new infections occurred in the United States. There were also 520 deaths. The number of hospitalized patients is decreasing, but 5,631 patients are still seriously or critically ill. The number of critically ill patients has decreased by 1,761 in the last 14 days, while 6,577 new deaths occurred. The number of critically ill patients is decreasing for the fourth 14-day period, but a large number of patients are still dying each day.
As of 6/04/21, we have had 612,249 deaths and 34,192,023 SARS-CoV-2 infections in the United States. We have had 271,267 new infections in the last 14 days. We are adding an average of 135,633 infections every 7 days. Each million infections usually results in 10,000 to 20,000 deaths. On 6/04/21, twenty-two states have had greater than 500,000 total infections, and 33 states have had greater than 5,000 total deaths. Nine states (Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York and California) have had greater than 35,000 deaths.
For comparison, on 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota 9.18% of the population was infected (ranked #1), and in South Dakota 8.03% of the population was infected (ranked #2).
As of 6/04/21, in the United States, 10.32% of the population has had a documented SARS-CoV-2 infection. In the last 6 months, over 6% of our country became infected with SARS-CoV-2.
As of 6/04/21, California was still ranked 36th in infection percentage at 9.60%. In North Dakota 14.45% of the population was infected (ranked #1), while Rhode Island was at 14.34% (ranked #2) and South Dakota was at 14.04% of the population infected (ranked #3). Thirty-one states have greater than 10% of their population infected and 42 states have greater than 9% of their population infected. Only one state has less than 3% of their population infected: Hawaii (2.52%).
New Mutants
In a response for the need for “easy-to-pronounce and non-stigmatising labels,” at the end of May, the World Health Organization assigned a letter from the Greek alphabet to each SARS-CoV-2 variant. GISAID, Nextstrain, and Pango will continue to use the previously established nomenclature. For our purposes, we’ll be referring to each variant by both its Greek alphabet letter and the Pango nomenclature.
The WHO has sorted variants into two categories: Variants of Concern (VOC) and Variants of Interest (VOI). The criteria for Variants of Concern are as follows:
Increase in transmissibility or detrimental change in COVID-19 epidemiology; or
Increase in virulence or change in clinical disease presentation; or
Decrease in effectiveness of public health and social measures or available diagnostics, vaccines, therapeutics.
The WHO categorizes the following four variants as Variants of Concern (VOC):
The criteria for Variants of Interest (VOI) are as follows:
has been identified to cause community transmission/multiple COVID-19 cases/clusters, or has been detected in multiple countries; OR
is otherwise assessed to be a VOI by WHO in consultation with the WHO SARS-CoV-2 Virus Evolution Working Group.
The WHO categorizes the following six variants as Variants of Interest (VOI):
A new mutant SARS-CoV-2 virus (lineage B.1.1.7, now referred to by WHO as Alpha), first seen in the UK in September 2020, has now been found in multiple other countries. This isolate has now been found in 50 states and the District of Columbia. This isolate is more infectious than other previously circulating B2 lineage isolates. There are two deletions and six other mutations in its spike protein. One mutation involves a change of one amino acid, an asparagine at position 501 in the receptor binding motif with a tyrosine. This enhances binding (affinity) to the ACE-2 receptor and may alone be responsible for the increased infectivity of this isolate. A study published March 10 in the British Medical Journal (BMJ) found that the risk of death increased by 64% in patients infected with the B.1.1.7 variant compared to all other isolates. Due to air and other travel, this isolate will become the dominant isolate worldwide.
On 4/10/21, the CDC stopped providing data to the public on the number of reported cases of all variants of SARS-CoV-2, both nationally and by state. This data used to be available at https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant-cases.html. The CDC claims that the data is available in its COVID-19 Data Tracker, but only percentages, not actual case numbers, are available, and the data ends on May 8, 2021.
Luckily, GISAID is still reporting variant data. The United States has had more isolations of the Alpha variant (B.1.1.7) in the last four weeks (9,795) than any other country in the world, to include the United Kingdom. There have been a total of 160,842 cases of Alpha/B.1.1.7 identified in the US to date. (See chart below.)
At 1,842 cases, the United States has the fourth highest number of isolations of the Beta variant (B.1.351, first identified in South Africa), and 76 of these were in the last four weeks.
And the United States has now surpassed Brazil for the most isolations of the Gamma variant (P.1) in the world, with 12,887 overall and 1,527 in the past four weeks.
As for the Delta Variant (B.1.617+), the variant recently identified in India, only India and the United Kingdom have more isolated cases than in the United States, which has 1,888 total cases, 546 of which were identified in the last four weeks.
The United States has also surpassed both the UK and Nigeria for the most isolations of the Eta varian (B.1.525) in the world, with 1,064 overall and 32 in the past four weeks.
A disturbing report out of the UK has found a second mutation in Alpha/B.1.1.7. This mutation, which occurs in the loop sequence, has also been found in the Beta/B.1.351 and Gamma/P.1 variants. (The loop sequence is in the receptor binding motif in the receptor binding domain of the S1 sequence of the spike protein.) This mutation involves a change of one amino acid of the spike protein, number 484, from glutamic acid to lysine. This point mutation allows the virus to bind better to the ACE2 receptor, which increases infectivity. People who are exposed to one of these variants (versus the old B2 isolate) are more likely to be infected and are more likely to transmit the virus to others.
In our last three updates we summarized a research letter published in Clinical Infectious Diseases about a patient in the UK who was first infected in April with a B2 isolate and experienced only mild symptoms but was infected with the new Alpha/B.1.1.7 variant in December and became critically ill. The patient described in this research letter was not protected by a natural infection with a B2 lineage SARS-CoV-2 isolate in April 2020 from having a potentially lethal second infection with a B.1.1.7 lineage variant in December 2020, suggesting that folks who have had a past SARS-CoV-2 infection should not expect to have any immunity to new variants such as Alpha/B.1.1.7. All of the currently available vaccines were developed with spike protein from B2 lineages. Moderna, Pfizer, and AstraZeneca/Oxford are currently remaking their spike protein vaccines to address the mutations in the South African variant of SARS-CoV-2 because the AstraZeneca/Oxford vaccine did not work in a small trial in South Africa, where most of the patients had the Beta/B.1.351 mutant.
New Mutant Delta/B.1.617+ Arrives in California
Stanford University announced five weeks ago that they have identified five infections with the Delta/B.1.617+ variant in the San Francisco Bay Area. There are actually three different B.1.617 variants: B.1.617.1, B.1.617.2 and B.1.617.3. The most common variant appears to be B.1.617.2. This isolate is a double-mutant responsible for greater than 50% of the infections in India. The data from India the last 14 days ending on 6/04/21 is still disturbing. India has had 2,541,685 infections in the last 14 days or an average of 181,549 infections per day. During this 14-day period India reported 59,354 deaths or 4,240 deaths per day. On May 21, 2021, India reported 121,476 new infections and 3,382 new deaths. On 6/04/21 the total deaths due to SARS-CoV-2 infections in India stood at 344,101. India, with a population of 1,390,456,911, has had only 2.06% of the country infected. Their hospitals are still running out of vaccines, oxygen, medications, beds and ventilators. Sadly a health disaster continues in the world’s most populous country. I would predict that prior SARS-CoV-2 infection in India or first generation SARS-CoV-2 vaccines will have a decreased effect on this mutant discussed in the next paragraph.
Many of you may now be familiar with the E484K mutation present in the Beta/B.1.351 isolate, the Gamma/P.1 isolate, the Iota/B.1.526 isolate, and the double mutant Eta/B.1.525. When vaccine manufacturers make booster vaccines to address these variants, they will only account for the E484K mutation. What sets this Delta/B.1.617+ variant apart from the other variants is that it has a different point mutation at amino acid 484 that involves a change of one amino acid of the spike protein, number 484, from glutamic acid to glutamine (E484Q). This point mutation, like E484K, probably allows the virus to bind to the ACE2 receptor and evade neutralizing antibodies directed against the original Wuhan sequence. A vaccine created to address E484K would not address this isolate.
The second mutation in Delta/B.1.617+ is L452R, which is one of the same mutations seen in Epsilon/B.1.427 + B.1.429. This mutation is also not being covered by any vaccine currently being made as a booster. It’s possible that people in California who were infected by the Epsilon mutant in the last six months might have some additional cross protective antibodies to Delta/B.1.617+.
Watching the Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC, whose most recent data on variants is from May 8.
Location
Total Infections as of 6/04/21
New Infections on 6/04/21
Total Deaths
New Deaths on 5/21/21
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate?
Currently in Lockdown?
World
173,713,909
400,075
3,736,099
9,283
2.22%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617+ (India)BV-1 (Texas, USA)
I’m pleased to see that COVID-19 cases and MIS-C (PIMS) cases in children in the US are finally getting national attention. The CDC now tracks total MIS-C cases and deaths in children and young adults up to 20 years old in the United States. As of June 2, CDC reported 4,018 cases of MIS-C that meet the case definition and 36 deaths—that’s 276 new cases and one new death since the May 3 report. The CDC notes, “As of October 1, the number of cases meeting the case definition for multisystem inflammatory syndrome in children (MIS-C) in the United States surpassed 1,000. As of February 1, this number surpassed 2,000, and exceeded 3,000 as of April 1.” This means it took seven months to reach 1,000 MIS-C cases, only four months to reach an additional 1,000 cases, and only two months to add an additional 1,185 cases. This suggests to us that Alpha/B.1.1.7 is causing more MIS-C.
Date of Reporting
Total MIS-C Patients
Change Since Last Report
Total MIS-C Deaths
Change Since Last Report
6/2/2021
4018
+276
36
+1
5/3/2021
3742
+557
35
-1
3/29/2021
3185
+568
36
+3
3/1/2021
2617
—
33
—
Schools in the United States have been open throughout the pandemic, with teachers and education support professionals demonstrating their extraordinary ability to adapt in adverse circumstances. Teachers all over the country reinvented their teaching, taking their classrooms online in order to provide safe and remote learning experiences for students. The so-called “reopening” of schools, which more accurately refers to the opening of school buildings, as schools never closed, has been highly politicized, with many governors issuing mandates for in-person instruction, even as case counts, hospitalizations, and deaths in their states rose exponentially. The CDC has maintained that transmission risk in schools is minimal, provided that adequate safety measures are taken; however, we know that many states have not properly enforced universal masking (and some are repealing mask mandates this week), and we know that many school facilities are not equipped with the proper air handling systems. With more school buildings opening, there is a growing body of research that suggests that COVID-19 transmission can and does happen in schools.
After recommending for months that school buildings be open, in mid-February (a year into the pandemic), The American Academy of Pediatrics, in collaboration with the Children’s Hospital Association, finally began tracking data on COVID-19 in children at the state and national level. Data reporting by states is still voluntary, and every state is different in its willingness to collect and disclose data on infections, hospitalizations, deaths, and testing rates in children.
As of the APA’s May 27 report, only 11 states provide age distribution for testing. This makes it difficult to hold states accountable for testing each age group in proportion to its population. We’ve seen a trend in states where testing data with age distribution is available that children are tested at lower rates than adults. Hospitalization data by age group is only available in 24 states and New York City, so we only understand the severity of COVID-19 infections in children for about half the country. Age distribution for cases is provided by 49 states, New York City, the District of Columbia, Puerto Rico, and Guam. Age distribution for deaths is provided in 43 states, New York City, Puerto Rico, and Guam. It’s worth noting that New York State does not provide age data for cases, testing, hospitalizations, and deaths. Two states, Florida and Utah, only report cases in children aged 0-14, so the number of cases, hospitalizations, and deaths in children ages 15-17 is unknown in these states.
As of May 27, A total of 322 child deaths due to COVID-19 were reported in 43 states (an increase of 6 child deaths in one week). In the United States, The following states do not report child mortality due to COVID-19: Michigan, Montana, New Mexico, New York, Rhode Island, South Carolina, and West Virginia. Texas only reports age data for 3% of confirmed COVID-19 cases, so state-level data from Texas is extremely limited for assessing the incidence of COVID-19 in children. Even considering this, Texas reported 52 child deaths. Arizona reported 33, California 23, Colorado 15 (+2), Florida 7, Georgia 10, Illinois 18, Maryland 10, Tennessee 10, Massachusetts 8 (+1), Pennsylvania 11, and New York City 24.
If we truly want to keep children safe, especially as many school buildings open for in-person instruction, we need to collect more complete data in every state on child testing rates, cases, hospitalizations, and deaths.
The New York Times reports that nationally, children 12 and up have higher vaccination rates than the general population, with 50% of children 12 and up vaccinated, and 53% of children 18 and up fully vaccinated, according to the CDC.
However, some states are falling far behind when it comes to getting children—and the general population—fully vaccinated. Idaho, Alabama, Mississippi, and Louisiana have given at least one shot to less than 10% of children 12-17 years old. Massachusetts, Hawaii, and Vermont are the only three states that have given at least one shot to at least 50% of children 12-15. California has given at least one shot to 36% of children 12-17 years old.
The Road Ahead
We are on Day 122 of the Biden-Harris administration.The President has made the pandemic a first priority and has now ordered enough vaccines to vaccinate everyone who wants a vaccination by July 2021. As of 6/5/21, 170.8 million people (approximately 51.5% of the population) have had one dose of any vaccine. 138.9 million people (41.9% of the population) are fully vaccinated.
As of May 10, all people in the U.S. over the age of 12 are eligible to receive a vaccine. The Biden administration has already exceeded its goal of administering 200 million doses of vaccine in the first 100 days of the administration. The Pfizer-BioNtech is already approved for ages 12-15 and the Moderna vaccine should be approved in June 2021. Moderna has applied for emergency use authorization to administer their mRNA vaccines to children aged 12-15. Testing is ongoing for children in younger age groups and may be approved for ages 2-11 by the end of September 2021.
Testing, wearing masks, social distancing and washing our hands frequently should no longer be political issues. These are non-pharmaceutical interventions used by most successful countries and some states to protect their citizens and their economies. New Zealand, Taiwan, and Australia are three countries that have done this successfully. In the United States, Hawaii is doing a better job handling the pandemic than many of our states. These interventions and vaccination should keep the pandemic from overwhelming our health care delivery systems world-wide. New mutations like Epsilon/B.1.427 + B.1.429 and the Alpha, Beta, Gamma, and Delta variants will probably spread rapidly throughout the United States over the next 90 days as many states (ex. Texas, Florida, Iowa, Mississippi, Wyoming and South Carolina) open up everything and do away with masking and social distancing. We will probably see increased new infections per day in the United States. In the UK, Alpha/B.1.1.7, has increased the number of infections, hospitalizations and deaths. This and other mutants may do the same thing in the USA.
The Pfizer and Moderna RNA vaccines and the Johnson & Johnson single dose vaccination adenovirus vaccine are all being used to immunize people in the USA. The Oxford-AstraZeneca vaccine and the Novavax vaccine may be available in the fourth quarter of 2021.
The bad news is that all currently available vaccines are based on the spike protein sequence identified in China in December 2019. Mutated isolates, as discussed above, may overtake our ability to produce new vaccines and vaccinate the populace. Like Influenza vaccines, we may have to reformulate vaccines based on active, worldwide surveillance at least every 4 to 6 months. The FDA is currently putting together a guidance document for how to develop booster vaccines for SARS-CoV-2 mutations. A surrogate marker of protection like antibody to the mutated Receptor Binding Domains of SARS-CoV-2 should be considered for vaccine approval.
The ideal approach to addressing the major mutations on at least five continents would be to make vaccines against each of the mutations. I’d get all of the vaccine companies and contract production companies on a call and “suggest” that two companies at least make and mass produce one of the four mutations. The government would pay the cost and buy at least 200 million doses in advance for each variant at say $40 a dose. The total cost to purchase the vaccine (800 million doses) would only be 32 billion dollars. Give each company a billion dollars each for development costs (another 8 billion dollars). Spend another two billion dollars for syringes and you’ve got enough booster doses to vaccinate 200 million people for all 4 variants. 42 billion dollars would be a small price to pay to catch up with the current mutations. Even if you had to do this every two years, it would be well worth the dollars spent.
We are not doing adequate numbers of PCR or antigen detection assays in the United States. According to JHU, in January of 2021, we were doing up to 2,307,949 tests per day. In March 2021, the highest number of tests per day was 1,709,210, and in April, the highest number of tests per day was 2,008,319. Currently, we’re doing 710,675 tests per day (7-day moving average); that’s 1,297,644 fewer tests per day than the April high.
We still need to perform more virus isolations and perform more DNA sequencing of viruses in each country, state, populous city, and county if we are to rapidly identify new mutations. I’m more hopeful that we will have the facilities, the equipment, and the trained staff needed to perform this work. As a nation we still need to make and distribute more vaccines to other countries, new vaccines directed against mutants, and the necessary rapid tests and protective equipment needed by medical staff, first responders, essential workers and especially teachers and students. I’m still hopeful we can work together on our and the world’s infectious disease problems.
SARS-CoV-2 Myocarditis in a High School Athlete after COVID-19 and Its Implications for Clearance for Sports (Children) https://doi.org/10.3390/children8060427
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
In the United States, SARS-CoV-2 deaths have decreased for the sixth time in a 14-day period. There were 96 fewer deaths per day than in the last 14-day period. In the last 14 days, the number of infections has decreased by 17,267 infections per day.Our infections per day are still high, probably secondary to SARS-CoV-2 mutants, to include the B.1.1.7 (UK isolate), a New York isolate B.1.526, the CAL.20C isolate, the South African isolate B.1.351, the Brazilian isolates P.1 and P.2, and the new Indian isolate B.1.617. I would predict that the opening of schools, places of worship, bars, restaurants, indoor dining and travel all will contribute to further spread of multiple SARS-CoV-2 mutants and rising numbers in infections, hospitalizations and deaths in the coming months. Increased traveling as well as upcoming Memorial Day weekend, summer vacations, and the July 4 holiday will all cause further increases. Vaccinations, increased mask usage and social distancing, which are a part of the Biden SARS-CoV-2 plan (day 122 of plan) will be necessary to stop spread of mutants and cause further reductions in infections, hospitalizations and deaths in the future. On 5/21/21, 29,014 new infections occurred in the United States. There were also 603 deaths. The number of hospitalized patients is decreasing, but 7,392 patients are still seriously or critically ill. The number of critically ill patients has decreased by 1,748 in the last 14 days, while 8,497 new deaths occurred. The number of critically ill patients is decreasing for the third 14 day period but a large number of patients are still dying each day.
As of 5/21/21, we have had 603,408 deaths and 33,862,398 SARS-CoV-2 infections in the United States. We have had 443,372 new infections in the last 14 days. We are adding an average of 221,686 infections every 7 days. Each million infections usually results in 10,000 to 20,000 deaths. On 5/21/21, twenty-two states have had greater than 500,000 total infections, and 33 states have had greater than 5,000 total deaths. Nine states (Michigan, Georgia, Illinois, New Jersey, Pennsylvania,Florida, Texas, New York and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York and California) have had greater than 35,000 deaths.
For comparison, on 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota 9.18% of the population was infected (ranked #1), and in South Dakota 8.03% of the population was infected (ranked #2).
As of 5/21/21, in the United States, 10.17% of the population has had a documented SARS-CoV-2 infection. In the last 6 months, over 6% of our country became infected with SARS-CoV-2.
As of 5/21/21, California was still ranked 36th in infection percentage at 9.55%. In North Dakota 14.30% of the population was infected (ranked #1), while Rhode Island was at 14.27% (ranked #2) and South Dakota was at 14.00% of the population infected (ranked #3). Thirty-one states have greater than 10% of their population infected and 41 states have greater than 9% of their population infected. Only one state has less than 3% of their population infected: Hawaii (2.52%). Ten states still have greater than 1,000 new infections per day with Florida leading again on 5/21/21 with 2,371 infections.
New Mutants
A new mutant SARS-CoV-2 virus (lineage B.1.1.7), first seen in the UK in September 2020, has now been found in multiple other countries. There are 3,170 reported cases in the USA as of 3/11/21, 8337 cases as of 3/25/21 and 20,915 cases as of 4/10/21 in the US. This isolate has now been found in 50 states and the District of Columbia. This isolate is more infectious than other previously circulating B2 lineage isolates. There are two deletions and six other mutations in its spike protein. One mutation involves a change of one amino acid, an asparagine at position 501 in the receptor binding motif with a tyrosine. This enhances binding (affinity) to the ACE-2 receptor and may alone be responsible for the increased infectivity of this isolate. A study published March 10 in the British Medical Journal (BMJ) found that the risk of death increased by 64% in patients infected with the B.1.1.7 variant compared to all other isolates. Due to air and other travel, this isolate will become the dominant isolate worldwide.
On 4/10/21, the CDC stopped providing data to the public on the number of reported cases of all variants of SARS-CoV-2, both nationally and by state. This data used to be available at https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant-cases.html. The CDC claims that the data is available in its COVID-19 Data Tracker, but only percentages, not actual case numbers, are available, and the data ends on April 10, 2021.
Luckily, GISAID is still reporting variant data. The United States has had more isolations of B.1.1.7 in the last four weeks (15,909) than any other country in the world, to include the United Kingdom. There have been a total of 132,214 cases of B.1.1.7 identified in the US to date. 22,300 have occurred in the last 4 weeks. (See chart below.)
At 191 cases, the United States has the fourth highest number of isolations of B.1.351 (the South African variant) in the last four weeks and a total of 1,564 isolations.
And the United States has now surpassed Brazil for the most isolations of P.1 in the world, with 10,362 overall and 3,003 in the past four weeks.
As for B.1.617, the variant recently identified in India, only India and the United Kingdom have more isolated cases than in the United States, which has 1,051 total cases, 506 of which were identified in the last four weeks.
The United States has also surpassed both the UK and Nigeria for the most isolations of B.1.525 in the world, with 938 overall and 109 in the past four weeks.
A disturbing report out of the UK has found a second mutation in B.1.1.7. This mutation, which occurs in the loop sequence, has also been found in the South African (B.1.351) and Brazilian (P.1) variants. (The loop sequence is in the receptor binding motif in the receptor binding domain of the S1 sequence of the spike protein.) This mutation involves a change of one amino acid of the spike protein, number 484, from glutamic acid to lysine. This point mutation allows the virus to bind better to the ACE2 receptor, which increases infectivity. People who are exposed to one of these variants (versus the old B2 isolate) are more likely to be infected and are more likely to transmit the virus to others.
In our last three updates we summarized a research letter published in Clinical Infectious Diseases about a patient in the UK who was first infected in April with a B2 isolate and experienced only mild symptoms but was infected with the new B.1.1.7 variant in December and became critically ill. The patient described in this research letter was not protected by a natural infection with a B2 lineage SARS-CoV-2 isolate in April 2020 from having a potentially lethal second infection with a B.1.1.7 lineage variant in December 2020, suggesting that folks who have had a past SARS-CoV-2 infection should not expect to have any immunity to new variants such as B.1.1.7. All of the currently available vaccines were developed with spike protein from B2 lineages. Moderna, Pfizer, and AstraZeneca/Oxford are currently remaking their spike protein vaccines to address the mutations in the South African variant of SARS-CoV-2 because the AstraZeneca/Oxford vaccine did not work in a small trial in South Africa, where most of the patients had the South African mutant (B.1.351).
A California Mutant
A fourth mutant isolate of SARS-CoV-2, B.1.429 + B.1.427 (CAL.20C), is the predominant mutation identified in California. This isolate does not have any of the mutations mentioned above, but contains five mutations, three of which are in the spike protein, but not in the receptor binding motif. This mutant may be partially responsible for the massive increase in infections in California, to include infections of people who had already recovered from a SARS-CoV-2 infection earlier. In California to date, we have had 3,775,758 infections and 62,858 total deaths. California is averaging 45 deaths per day in the last 14 days, which is a 13 deaths per day decrease from the preceding 14 day period. Currently, 9.55% of the population in California is infected. Nationally, we rank 35th in the percentage of people in the state infected. To my knowledge, only one privately held company is currently modifying their vaccine to cover the B.1.429 + B.1.427 mutant.
New Indian Mutant B.1.617 Arrives in California
Stanford University announced five weeks ago that they have identified five infections with the Maharashtra India VOC 32421 (new variant designation B.1.617) in the San Francisco Bay Area. There are actually three different B.1.617 variants: B.1.617.1, B.1.617.2 and B.1.617.3. The most common variant appears to be B.1.617.2 This isolate is a double-mutant responsible for greater than 50% of the infections in India. The data from India the last 14 days ending on 5/21/21 is still disturbing. India has had 4,398,458 infections in the last 14 days or an average of 314,176 infections per day. During this 14-day period India reported 57,243 deaths or 4,089 deaths per day. On May 21, 2021, India reported 254,395 new infections and 4,143 new deaths. On 5/21/21 the total deaths due to SARS-CoV-2 infections in India stood at 295,508. India, with a population of 1,390,456,911, has had only 1.88% of the country infected. Their hospitals are still running out of vaccines, oxygen, medications, beds and ventilators. Sadly a health disaster continues in the world’s most populous country. I would predict that prior SARS-CoV-2 infection in India or first generation SARS-CoV-2 vaccines will have a decreased effect on this mutant discussed in the next paragraph.
Many of you may now be familiar with the E484K mutation present in the South African isolate, the Brazilian isolate, the New York isolate (B.1.256), and the new Nigerian/UK double mutant. When vaccine manufacturers make booster vaccines to address these variants, they will only account for the E484K mutation. What sets this Maharashtra India B.1.617 variant apart from the other variants is that it has a different point mutation at amino acid 484 that involves a change of one amino acid of the spike protein, number 484, from glutamic acid to glutamine (E484Q). This point mutation, like E484K, probably allows the virus to bind to the ACE2 receptor and evade neutralizing antibodies directed against the original Wuhan sequence. A vaccine created to address E484K would not address this isolate.
The second mutation in Maharashtra India VOC B.1.617 is L452R, which is one of the same mutations seen in CAL.20C (B.1.429 + B.1.427). This mutation is also not being covered by any vaccine currently being made as a booster. It’s possible that people in California who were infected by the Cal.20C mutant in the last six months might have some additional cross protective antibodies to B.1.617.
Watching the Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC, whose most recent data on variants is from May 8.
Location
Total Infections as of 5/21/21
New Infections on 5/21/21
Total Deaths
New Deaths on 5/21/21
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate?
Currently in Lockdown?
World
166,465,183
621,048
3,457,500
12,778
2.13%
B2 lineageB.1.1.7 (UK)B.1.525 (Nigeria/UK)B.1.526 (USA-NYC)B.1.351 (SA)B.1.429 + B.1.427 (USA)*P.1 (Brazil)P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421B.1.617+ (India)BV-1 (Texas, USA)
I’m pleased to see that COVID-19 cases and MIS-C (PIMS) cases in children in the US are finally getting national attention. The CDC now tracks total MIS-C cases and deaths in children and young adults up to 20 years old in the United States. As of May 3, CDC reported 3,742 cases of MIS-C that meet the case definition and 35 deaths—that’s 557 new cases and no new deaths since the March 29 report. The CDC notes, “As of October 1, the number of cases meeting the case definition for multisystem inflammatory syndrome in children (MIS-C) in the United States surpassed 1,000. As of February 1, this number surpassed 2,000, and exceeded 3,000 as of April 1.” This means it took seven months to reach 1,000 MIS-C cases, only four months to reach an additional 1,000 cases, and only two months to add an additional 1,185 cases. This suggests to us that B.1.1.7 is causing more MIS-C. We’re averaging over 500 new cases of MIS-C each month for the last two months, despite decreases in the number of SARS-CoV-2 infections in the United States.
Date of Reporting
Total MIS-C Patients
Change Since Last Report
Total MIS-C Deaths
Change Since Last Report
5/3/2021
3742
+557
35
-1
3/29/2021
3185
+568
36
+3
3/1/2021
2617
—
33
—
Schools in the United States have been open throughout the pandemic, with teachers and education support professionals demonstrating their extraordinary ability to adapt in adverse circumstances. Teachers all over the country reinvented their teaching, taking their classrooms online in order to provide safe and remote learning experiences for students. The so-called “reopening” of schools, which more accurately refers to the opening of school buildings, as schools never closed, has been highly politicized, with many governors issuing mandates for in-person instruction, even as case counts, hospitalizations, and deaths in their states rose exponentially. The CDC has maintained that transmission risk in schools is minimal, provided that adequate safety measures are taken; however, we know that many states have not properly enforced universal masking (and some are repealing mask mandates this week), and we know that many school facilities are not equipped with the proper air handling systems. With more school buildings opening, there is a growing body of research that suggests that COVID-19 transmission can and does happen in schools.
After recommending for months that school buildings be open, in mid-February (a year into the pandemic), The American Academy of Pediatrics, in collaboration with the Children’s Hospital Association, finally began tracking data on COVID-19 in children at the state and national level. Data reporting by states is still voluntary, and every state is different in its willingness to collect and disclose data on infections, hospitalizations, deaths, and testing rates in children.
As of the APA’s May 20 report, only 11 states provide age distribution for testing. This makes it difficult to hold states accountable for testing each age group in proportion to its population. We’ve seen a trend in states where testing data with age distribution is available that children are tested at lower rates than adults. Hospitalization data by age group is only available in 24 states and New York City, so we only understand the severity of COVID-19 infections in children for about half the country. Age distribution for cases is provided by 49 states, New York City, the District of Columbia, Puerto Rico, and Guam. It’s worth noting that New York State does not provide age data for cases, testing, hospitalizations, and deaths. Two states, Florida and Utah, only report cases in children aged 0-14, so the number of cases, hospitalizations, and deaths in children ages 15-17 is unknown in these states.
As of May 20, A total of 316 child deaths due to COVID-19 were reported in 43 states (an increase of 8 child deaths in one week). In the United States, The following states do not report child mortality due to COVID-19: Michigan, Montana, New Mexico, New York, Rhode Island, South Carolina, and West Virginia. Texas only reports age data for 3% of confirmed COVID-19 cases, so state-level data from Texas is extremely limited for assessing the incidence of COVID-19 in children. Even considering this, Texas reported 52 child deaths. Arizona reported 33 (+2), California 23 (+2), Colorado 13, Florida 7 (+1), Georgia 10, Illinois 18, Maryland 10, Tennessee 10, Massachusetts 7 (+2), Pennsylvania 11 (+1), and New York City 24.
If we truly want to keep children safe, especially as many school buildings open for in-person instruction, we need to collect more complete data in every state on child testing rates, cases, hospitalizations, and deaths.
The Road Ahead
We are on Day 122 of the Biden-Harris administration.The President has made the pandemic a first priority and has now ordered enough vaccines to vaccinate everyone who wants a vaccination by July 2021. As of 5/24/21, 164.3 million people have had one dose of any vaccine. 131 million people are fully vaccinated.
As of May 10, all people in the U.S. over the age of 12 are eligible to receive a vaccine. The Biden administration has already exceeded its goal of administering 200 million doses of vaccine in the first 100 days of the administration. The Pfizer-BioNtech is already approved for ages 12-15 and the Moderna vaccine should be approved in June 2021. Moderna has applied for emergency use authorization to administer their mRNA vaccines to children aged 12-15. Testing is ongoing for children in younger age groups and may be approved for ages 2-11 by the end of September 2021.
Testing, wearing masks, social distancing and washing our hands frequently should no longer be political issues. These are non-pharmaceutical interventions used by most successful countries and some states to protect their citizens and their economies. New Zealand, Taiwan, and Australia are three countries that have done this successfully. In the United States, Hawaii is doing a better job handling the pandemic than many of our states. These interventions and vaccination should keep the pandemic from overwhelming our health care delivery systems world-wide. New mutations like B.1.429 + B.1.427 (Cal.20C) and the UK, Brazillian, South African, and Indian variants will probably spread rapidly throughout the United States over the next 90 days as many states (particularly in Texas, Florida, Iowa, Mississippi, Wyoming and South Carolina) open up everything and do away with masking and social distancing. We will probably see increased new infections per day in the United States. In the UK, B.1.1.7, has increased the number of infections, hospitalizations and deaths. This and other mutants may do the same thing in the USA.
The Pfizer and Moderna RNA vaccines and the Johnson & Johnson single dose vaccination adenovirus vaccine are all being used to immunize people in the USA. The Oxford-AstraZeneca vaccine and Novavax vaccine may be available in the fourth quarter of 2021.
The bad news is that all currently available vaccines are based on the Chinese spike protein sequence from December 2019. Mutated isolates, as discussed above, may overtake our ability to produce new vaccines and vaccinate the populace. Like Influenza vaccines, we may have to reformulate vaccines based on active, worldwide surveillance at least every 4 to 6 months. The FDA is currently putting together a guidance document for how to develop booster vaccines for SARS-CoV-2 mutations. A surrogate marker of protection like antibody to the mutated Receptor Binding Domains of SARS-CoV-2 should be considered for vaccine approval.
The ideal approach to spreading major mutations on at least five continents would be to make vaccines against each of the mutations. I’d get all of the vaccine companies and contract production companies on a call and “suggest” that two companies at least make and mass produce one of the four mutations. The government would pay the cost and buy at least 200 million doses in advance for each variant at say $40 a dose. The total cost to purchase the vaccine (800 million doses) would only be 32 billion dollars. Give each company a billion dollars each for development costs (another 8 billion dollars). Spend another two billion dollars for syringes and you’ve got enough booster doses to vaccinate 200 million people for all 4 variants. 42 billion dollars would be a small price to pay to catch up with the current mutations. Even if you had to do this every two years, it would be well worth the dollars spent.
We are not doing adequate numbers of PCR or antigen detection assays in the United States. According to JHU, in January of 2021, we were doing up to 2,307,949 tests per day. In March 2021, the highest number of tests per day was 1,709,210, and in April, the highest number of tests per day was 2,008,319. Currently, we’re doing 975,589 tests per day (7-day moving average); that’s 453,963 fewer tests per day than the April high.
We still need to perform more virus isolations and perform more DNA sequencing of viruses in each country, state, populous city, and county if we are to rapidly identify new mutations. I’m more hopeful that we will have the facilities, the equipment, and the trained staff needed to perform this work. As a nation we still need to make and distribute more vaccines for other countries, new vaccines directed against mutants, and the necessary rapid tests and protective equipment needed by medical staff, first responders, essential workers and especially teachers and students. I’m still hopeful we can work together on our and the world’s infectious disease problems.
It’s time for our next 14-day moving average determinations and projections for infections and deaths from SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
In the United States, SARS-CoV-2 deaths have decreased for the sixth time in a 14-day period. There were 28 fewer deaths per day than in the last 14-day period. In the last 14 days, the number of infections has decreased by 17,700 infections per day.Our infections per day is still extremely high, probablysecondary to SARS-CoV-2 mutants, to include the B.1.1.7 (UK isolate), a New York isolate B.1.526, the CAL.20C isolate, the South African isolate and the Brazilian isolates and the new Indian isolate. I would predict that the opening of schools, places of worship, bars, restaurants, indoor dining and travel all will contribute to further spread of multiple SARS-CoV-2 mutants and rising numbers in infections, hospitalizations and deaths in the coming months. Increased traveling as well as upgoing Memorial Day weekend, summer vacations and the July 4th holiday will all cause further increases. Vaccinations, increased mask usage and social distancing, which are a part of the Biden SARS-CoV-2 plan (day 108 of plan) will be necessary to stop spread of mutants and cause further reductions in infections, hospitalizations and deaths in the future. On 5/07/21, 49,491 new infections occurred in the United States. There were also 770 deaths. The number of hospitalized patients is decreasing, but 9,140 patients are still seriously or critically ill. The number of critically ill patients has decreased by 692 in the last 14 days, while 9,836 new deaths occurred. The number of critically ill patients is decreasing for the second 14 day period but a large number of patients are still dying each day.
As of 5/07/21, we have had 594,911 deaths and 33,418,826 SARS-CoV-2 infections in the United States. We have had 683,122 new infections in the last 14 days. We are adding an average of 341,561 infections every 7 days. Each million infections usually results in 10,000 to 20,000 deaths. On 5/07/21, twenty-two states have had greater than 500,000 total infections, and 32 states have had greater than 5,000 total deaths. Eight states (Geogia, illinois, New Jersey, Pennsylvania,Florida, Texas, New York and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York and California) have had greater than 35,000 deaths.
For comparison, on 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota 9.18% of the population was infected (ranked #1), and in South Dakota 8.03% of the population was infected (ranked #2).
As of 5/07/21, in the United States, 10.04% of the population has had a documented SARS-CoV-2 infection. In the last 5 months nearly 6% of our country became infected with SARS-CoV-2.
As of 5/07/21, California was still ranked 35th in infection percentage at 9.50%. In North Dakota 14.21% of the population was infected (ranked #1), while Rhode Island was at 14.11% (ranked #2) and South Dakota was at 13.93% of the population infected (ranked #3). Thirty states have greater than 10% of their population infected. Only one state has less than 3.5% of their population infected: Hawaii (2.30%). Fourteen states still have greater than 1,000 new infections per day with Florida leading again on 5/7/21 with 4,175 infections.
New Mutants
A new mutant SARS-CoV-2 virus (lineage B.1.1.7), first seen in the UK in September 2020, has now been found in multiple other countries. There are 3,170 reported cases in the USA as of 3/11/21, 8337 cases as of 3/25/21 and 20,915 cases as of 4/10/21 in the US. This isolate has now been found in 50 states and the District of Columbia. This isolate is more infectious than other previously circulating B2 lineage isolates. There are two deletions and six other mutations in its spike protein. One mutation involves a change of one amino acid, an asparagine at position 501 in the receptor binding motif with a tyrosine. This enhances binding (affinity) to the ACE-2 receptor and may alone be responsible for the increased infectivity of this isolate. A study published March 10 in the British Medical Journal (BMJ) found that the risk of death increased by 64% in patients infected with the B.1.1.7 variant compared to all other isolates. Due to air and other travel, this isolate will become the dominant isolate worldwide.
On 4/10/21, the CDC stopped providing data to the public on the number of reported cases of all variants of SARS-CoV-2, both nationally and by state. This data used to be available at https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant-cases.html. The CDC claims that the data is available in its COVID-19 Data Tracker, but only percentages, not actual case numbers, are available, and the data ends on April 10, 2021.
Luckily, GISAID is still reporting variant data. The United States has had more isolations of B.1.1.7 in the last four weeks (15,909) than any other country in the world, to include the United Kingdom. There have been a total of 85,324 cases of B.1.1.7 identified in the US to date. (See chart below.)
At 197 cases, the United States has the fourth highest number of isolations of B.1.351 (the South African variant) in the last four weeks and a total of 1,161 isolations.
And the United States has now surpassed Brazil for the most isolations of P.1 in the world, with 5,355 overall and 1,955 in the past four weeks.
As for B.1.617, the variant recently identified in India, only India and the United Kingdom have more isolated cases than in the United States, which has 334 total cases, 197 of which were identified in the last four weeks. This also means that we had 137 known cases of this variant in the US more than a month ago, despite the fact that American news media and the CDC have only recently begun educating the public about this variant.
A disturbing report out of the UK has found a second mutation in B.1.1.7. This mutation, which occurs in the loop sequence has also been found in the South African (B.1.351) and Brazilian (P.1) variants. (The loop sequence is in the receptor binding motif in the receptor binding domain of the S1 sequence of the spike protein.) This mutation involves a change of one amino acid of the spike protein, number 484, from glutamic acid to lysine. This point mutation allows the virus to bind better to the ACE2 receptor, which increases infectivity. People who are exposed to one of these variants (versus the old B2 isolate) are more likely to be infected and are more likely to transmit the virus to others.
In our last three updates we summarized a research letter published in Clinical Infectious Diseases about a patient in the UK who was first infected in April with a B2 isolate and experienced only mild symptoms but was infected with the new B.1.1.7 variant in December and became critically ill. The patient described in this research letter was not protected by a natural infection with a B2 lineage SARS-CoV-2 isolate in April 2020 from having a potentially lethal second infection with a B.1.1.7 lineage variant in December 2020, suggesting that folks who have had a past SARS-CoV-2 infection should not expect to have any immunity to new variants such as B.1.1.7. All of the currently available vaccines were developed with spike protein from B2 lineages. Moderna, Pfizer, and AstraZeneca/Oxford are currently remaking their spike protein vaccines to address the mutations in the South African variant of SARS-CoV-2 because the AstraZeneca/Oxford vaccine did not work in a small trial in South Africa, where most of the patients had the South African mutant (B.1.351).
A California Mutant
A fourth mutant isolate of SARS-CoV-2, B.1.429 + B.1.427 (CAL.20C), is the predominant mutation identified in California. This isolate does not have any of the mutations mentioned above, but contains five mutations, three of which are in the spike protein, but not in the receptor binding motif. This mutant may be partially responsible for the massive increase in infections in California, to include infections of people who had already recovered from a SARS-CoV-2 infection earlier. In California to date, we have had 3,756,393 infections and 62,220 total deaths. California is averaging 58 deaths per day in the last 14 days, which is a 22 deaths per day decrease from the preceding 14 day period. Currently, 9.50% of the population in California is infected. Nationally, we rank 35th in the percentage of people in the state infected. To my knowledge, only one privately held company is currently modifying their vaccine to cover the B.1.429 + B.1.427 mutant.
New Indian Mutant B.1.617 Arrives in California
Stanford University announced three weeks ago that they have identified five infections with the Maharashtra India VOC 32421 (new variant designation B.1.617) in the San Francisco Bay Area. Two additional isolates were PCR positive and pending sequencing. This isolate is a double-mutant responsible for greater than 40% of the infections in India. In the last 14 day update India had had 2,080,793 new infections in the 7 days prior which was a 58% change in the number of infections from the preceding 7 days (1,318,900 infections). Indian had reported the three highest numbers of new infections per day at 349,165 on 3/24/21, 345,147 on 2/23/21, and 332,503 new infections on 4/22/21. India is the only country to report over a million infections in three days. The previous one day record was 302,000 infections in the United States. In India 13,876 new SARS-CoV-2 deaths had occurred in the last seven days compared to 7,206 deaths in the preceding seven days. This was a 93% increase in the death rate in the last seven days.
The data from India the last 14 days ending on 5/07/21 is even more disturbing. India has had 5,284,155 infections in the last 14 days with an average of 377,440 infections per day or 1,132,320 infections every three days. During this 14 day period India reported 48,716 deaths or 3,480 deaths per day. On May 7, 2021 India reported 401,326 new infections and 4,194 new deaths. On 5/7/21 the total deaths due to SARS-CoV-2 infections in India now stands at 238,265. India with a population of 1,390,456,911 has had only 1.57% of the country infected. Their hospitals are still running out of oxygen, medications, beds and ventilators. They had only been able to vaccinate approximately 140 million people.Sadly a health disaster is now occurring in the world’s most populous country. I would predict that prior SARS-CoV-2 infection in India or first generation SARS-CoV-2 vaccines will have little effect on this mutant discussed in the next paragraph.
Many of you may now be familiar with the E484K mutation present in the South African isolate, the Brazilian isolate, the New York isolate (B.1.256), and the new Nigerian/UK double mutant. When vaccine manufacturers make booster vaccines to address these variants, they will only account for the E484K mutation. What sets this Maharashtra India B.1.617 variant apart from the other variants is that it has a different point mutation at amino acid 484 that involves a change of one amino acid of the spike protein, number 484, from glutamic acid to glutamine (E484Q). This point mutation, like E484K, probably allows the virus to bind to the ACE2 receptor and evade neutralizing antibodies directed against the original Wuhan sequence. A vaccine created to address E484K would not address this isolate.
The second mutation in Maharashtra India VOC B1.617 is L452R, which is one of the same mutations seen in CAL.20C (B.1.429 + B.1.427). This mutation is also not being covered by any vaccine currently being made as a booster. It’s possible that people in California who were infected by the Cal.20C mutant in the last six months might have some cross protective antibodies to B.1.617.
Watching the Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 5/07/21
New Infections on 5/7/21
Total Deaths
New Deaths on 5/07/21
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate?
Currently in Lockdown?
World
157,526,509
836,031
3,283,260
13,741
2.02%
B2 lineageB.1.1.7 (UK)B.1.525 (Nigeria/UK)B.1.526 (USA-NYC)B.1.351 (SA)B.1.429 + B.1.427 (USA)*P.1 (Brazil)P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Maharashtra India VOC B.1.617 BV-1 (Texas, USA)
No
No
USA
33,418,826 (ranked #1)
49,491 (ranked #3)
594,911 (ranked #1)
790
10.04%
B2 lineageB.1.1.7 (UK)B.1.525 (Nigeria/UK)B.1.526 (USA-NYC)B.1.351 (SA)B.1.429 + B.1.427 (USA)*P.1 (Brazil)P.2 (Brazil)Maharashtra India VOC B.1.617BV-1 (Texas, USA)
We are on Day 108 of the Biden-Harris administration.The President has made the pandemic a first priority and has now ordered enough vaccine to vaccinate everyone who wants a vaccination by July 2021. As of 5/7/21, 149.5 million people have had one dose of any vaccine. 8.6 million have had a single-dose vaccine (J&J). 108.9 million people are fully vaccinated. Therefore, 32 million people still need a second dose of either the Pfizer or the Moderna vaccine.
As of April 16, all people in the U.S. over the age of 16 are eligible to receive a vaccine. The Biden administration has already exceeded its goal of administering 200 million doses of vaccine in the first 100 days of the administration. Pfizer and Moderna have applied for emergency use authorization to administer their mRNA vaccines to children aged 12-15, and the FDA is expected to authorize the Pfizer vaccine for this age group next week. Testing is ongoing for children in younger age groups and may be approved for ages 2-11 by September 2021.
Testing, wearing masks, social distancing and washing our hands frequently should no longer be political issues. These are non-pharmaceutical interventions used by most successful countries and some states to protect their citizens and their economies. New Zealand, Taiwan, and Australia are three countries that have done this successfully. In the United States, Hawaii is doing a better job handling the pandemic than many of our states. These interventions and vaccination should keep the pandemic from overwhelming our health care delivery system. New mutations like B.1.429 + B.1.427 (Cal.20C) and the UK, Brazillian, South African, and Indian variants will probably spread rapidly throughout the United States over the next 90 days as several states (including Texas, Florida, Iowa, Mississippi) open up everything and do away with masking and social distancing. We will probably see increased new infections per day in the United States. In the UK, B.1.1.7, has increased the number of infections, hospitalizations and deaths. This and other mutants may do the same thing in the USA.
The Pfizer and Moderna RNA vaccines and the Johnson & Johnson single dose vaccination adenovirus vaccine are all being used to immunize people in the USA. The Oxford-AstraZeneca vaccine and Novavax vaccine may be available in the second or third quarter of 2021.
The bad news is that all currently available vaccines are based on the Chinese spike protein sequence from December 2019. Mutated isolates, as discussed above, may overtake our ability to produce new vaccines and vaccinate the populace. Like Influenza vaccines, we may have to reformulate vaccines based on active, worldwide surveillance at least every 4 to 6 months. The FDA is currently putting together a guidance document for how to develop booster vaccines for SARS-CoV-2 mutations. A surrogate marker of protection like antibody to the mutated Receptor Binding Domains of SARS-CoV-2 should be considered for vaccine approval.
I still feel the current approach of companies and governments of making new vaccines against just the South African variant is wrong. In Brazil, where the P.1 isolate is dominant, they’ve had another 849,250 infections and 32,770 deaths in just the last 14 days. In the last 42 days in Brazil 2,762,595 infections have occurred and 115,667 deaths. In South Africa, the total number of infections during the pandemic is 1,592,326 and a total of 54,687 deaths. Brazil had more infections and deaths in one month than South Africa has had for the entire pandemic. It makes no sense to make a vaccine based on just the South African mutant and not make one for the Brazilian P.1 mutant. Even worse is the current situation with the Indian SARS-CoV-2 VOC B.1.617. In the last 14 days India has had 5,284,155 new infections and 48,716 deaths. If India shuts down, among other things the generic drug industry could fail.
The ideal approach to these spreading major mutations on at least five continents would be to make vaccines against each of the mutations. I’d get all of the vaccine companies and contract production companies on a call and “suggest” that two companies at least make and mass produce one of the four mutations. The government would pay the cost and buy at least 200 million doses in advance for each variant at say $40 a dose. The total cost to purchase the vaccine (800 million doses) would only be 32 billion dollars. Give each company a billion dollars each for development costs (another 8 billion dollars). Spend another two billion dollars for syringes and you’ve got enough booster doses to vaccinate 200 million people for all 4 variants. 42 billion dollars would be a small price to pay to catch up with the current mutations. Even if you had to do this every two years, it would be well worth the dollars spent.
We are not doing adequate numbers of PCR or antigen detection assays in the United States. According to JHU, in January of 2021, we were doing up to 2,307,949 tests per day. In March 2021, the highest number of tests per day was 1,709,210, and in April, the highest number of tests per day was 2,008,319. Currently, we’re doing 1,260,357 tests per day (7-day moving average); that’s 747,962 fewer tests than the April high.
We still need to perform more virus isolations and perform more DNA sequencing of viruses in each country, state, populous city, and county if we are to rapidly identify new mutations. I’m more hopeful that we will have the facilities, the equipment, and the trained staff needed to perform this work. As a nation we are finally preparing to make more vaccine, new vaccines directed against mutants, and the necessary rapid tests and protective equipment needed by medical staff, first responders, essential workers and especially teachers and students. I’m still hopeful we can work together on our and the world’s infectious disease problems.
What Our Team Is Reading This Week
Pathogenic priming likely contributes to serious and critical illness mortality in COVID-19 via autoimmunity Journal of Translational Autoimmunity 3(2020)100051 https://dx.doi.org/10.1016%2Fj.jtauto.2020.100051
Evaluating a commercially available in-duct bipolar ionization device for pollutant removal and potential byproduct formation (Building and Environment) https://doi.org/10.1016/j.buildenv.2021.107750



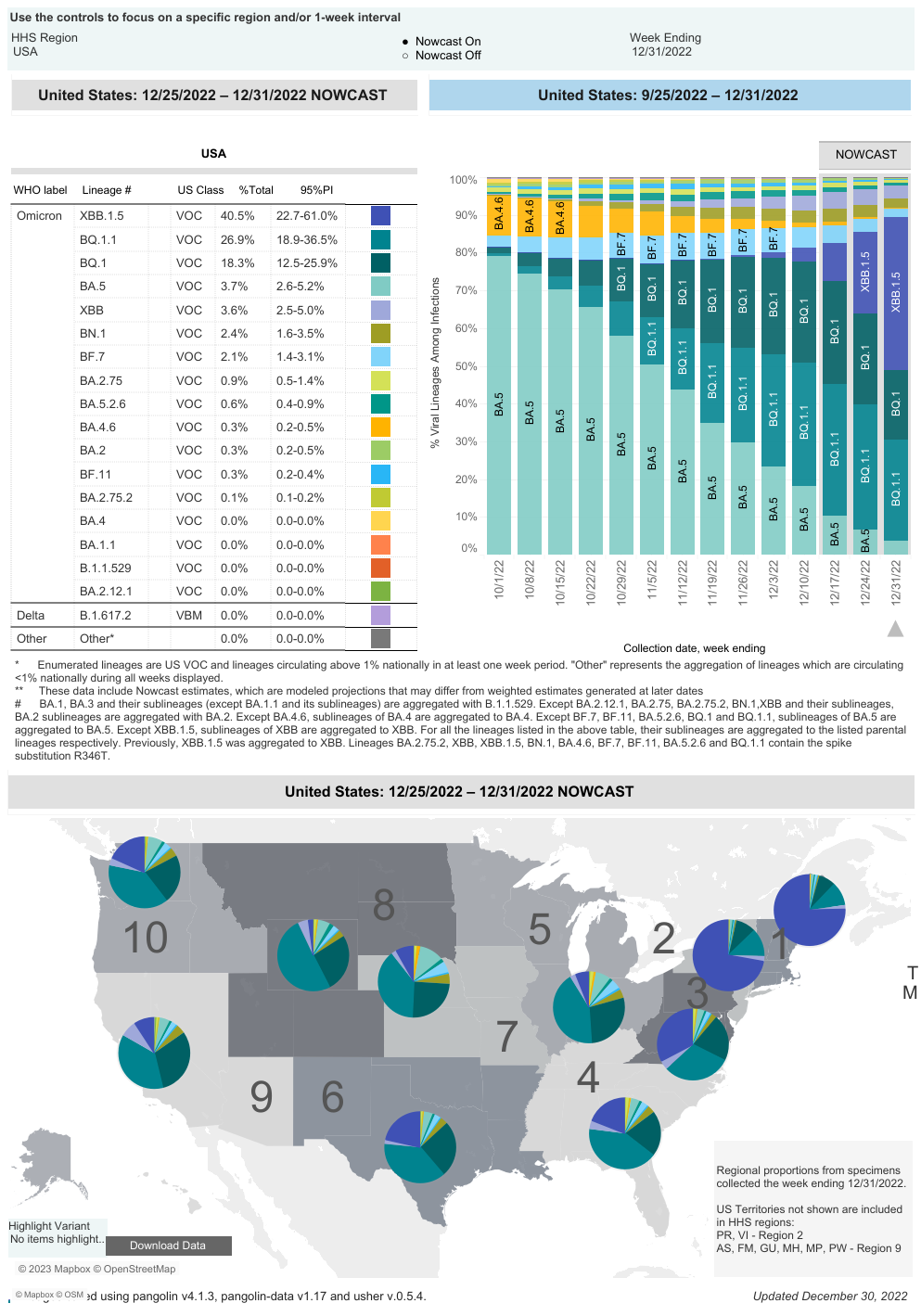
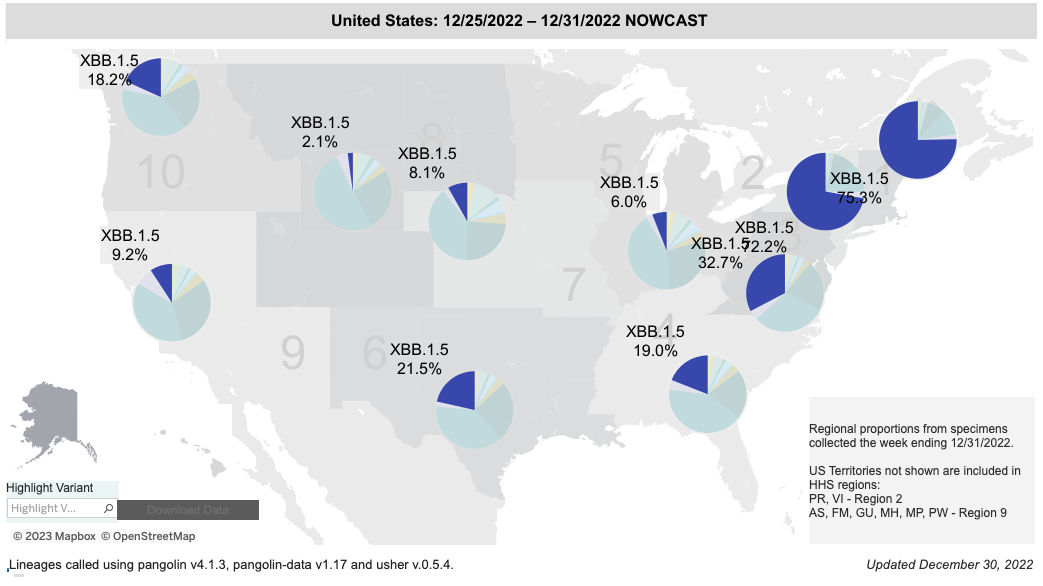

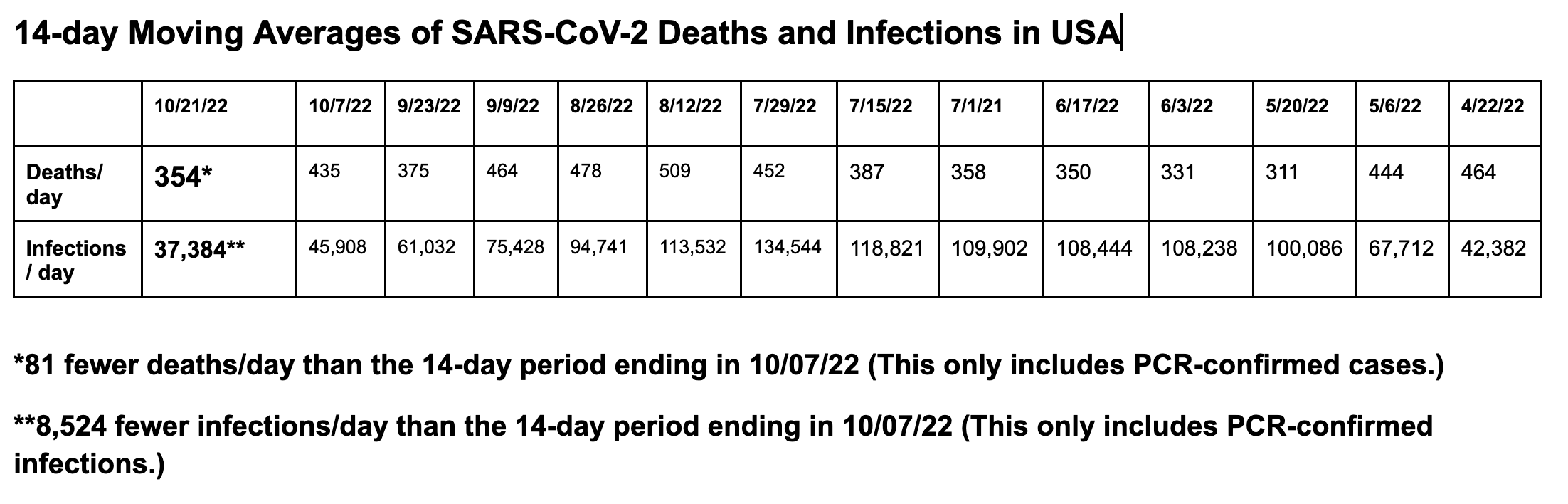
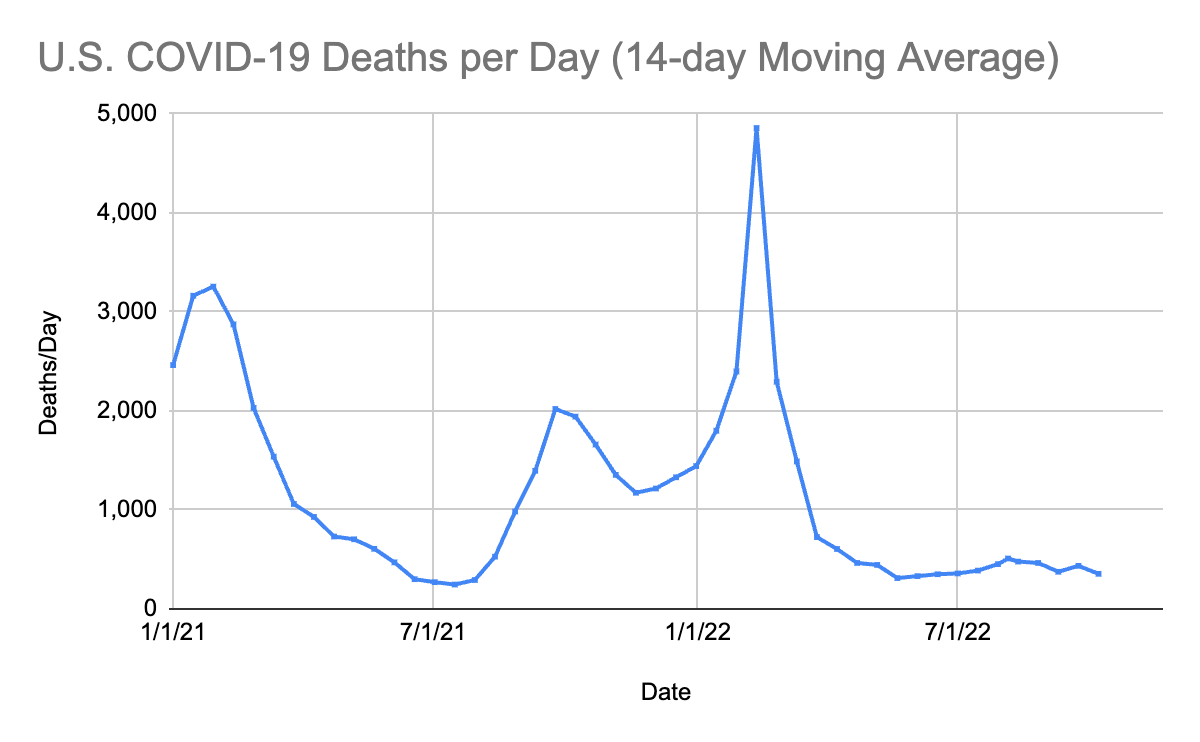
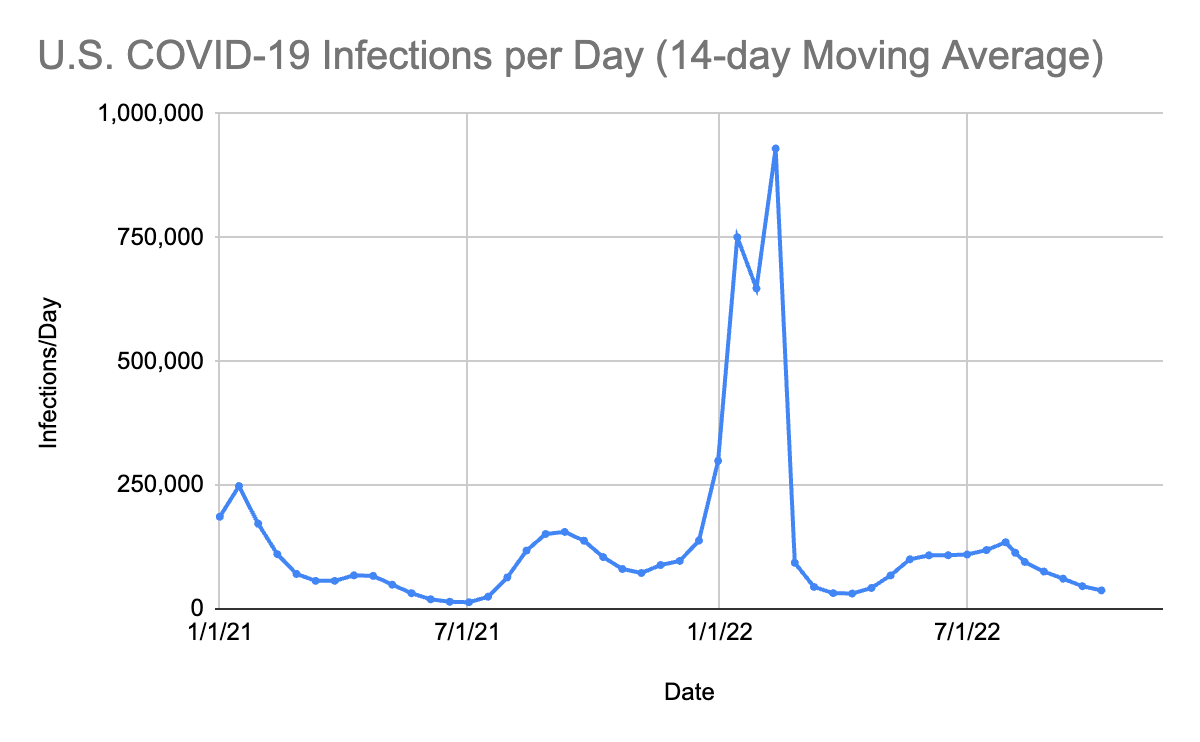
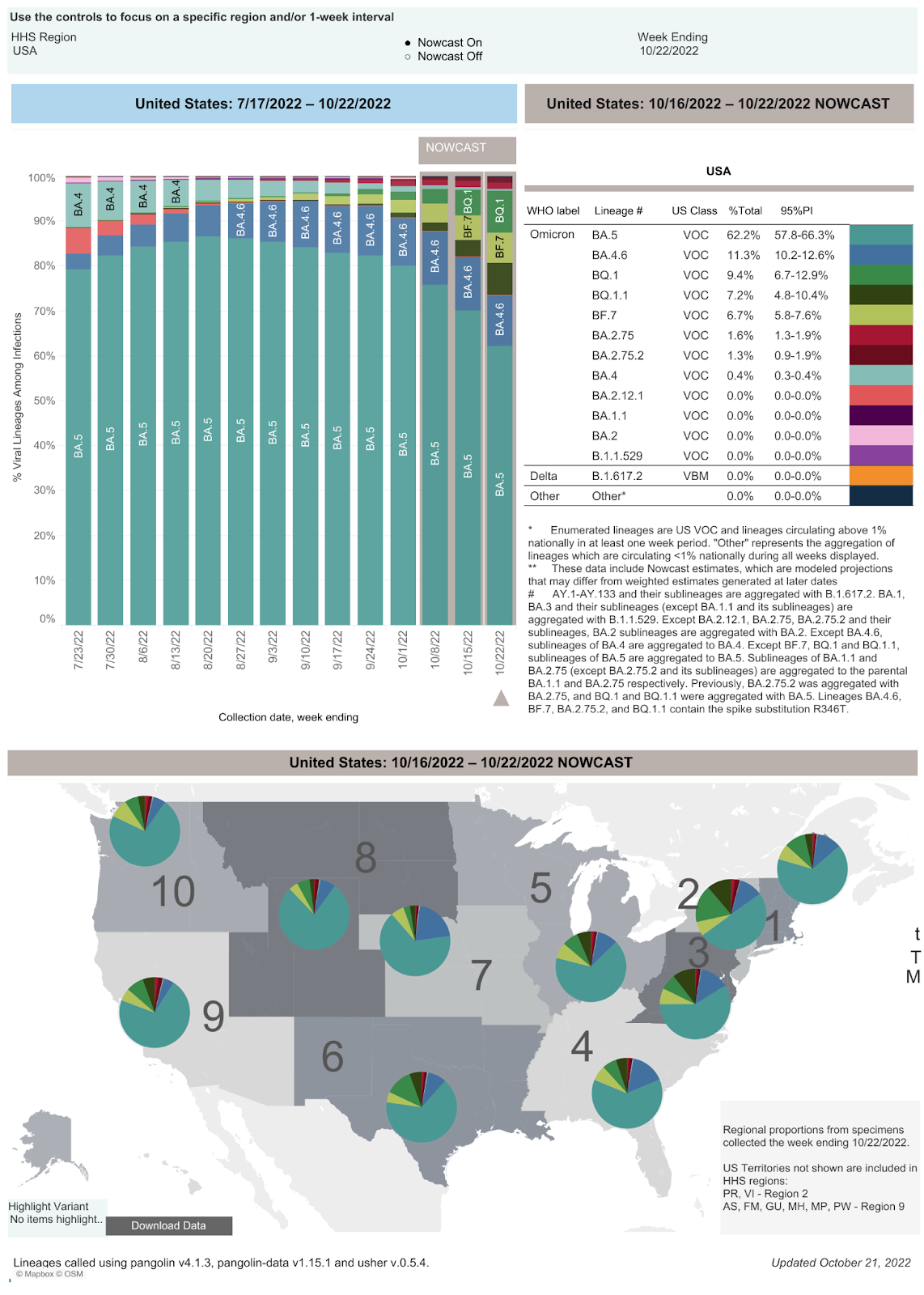
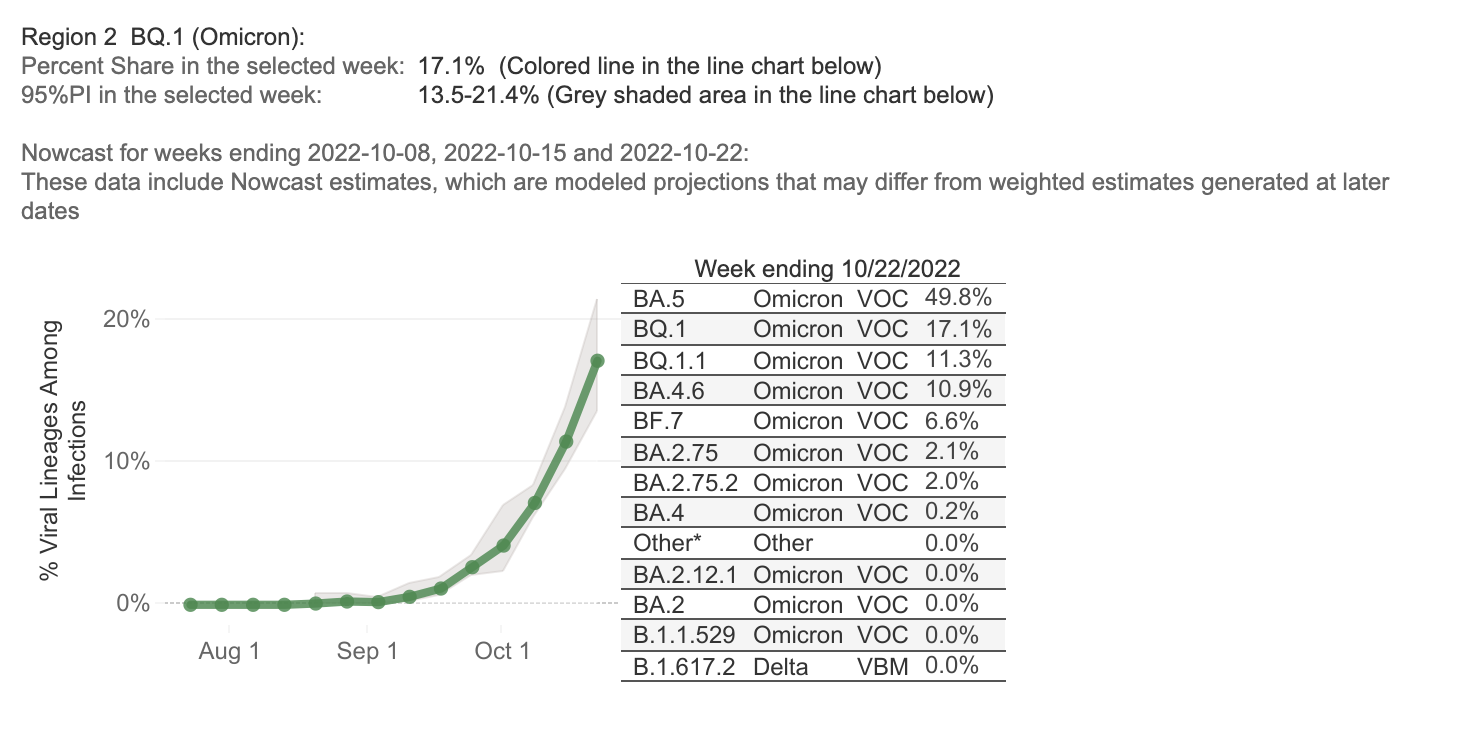
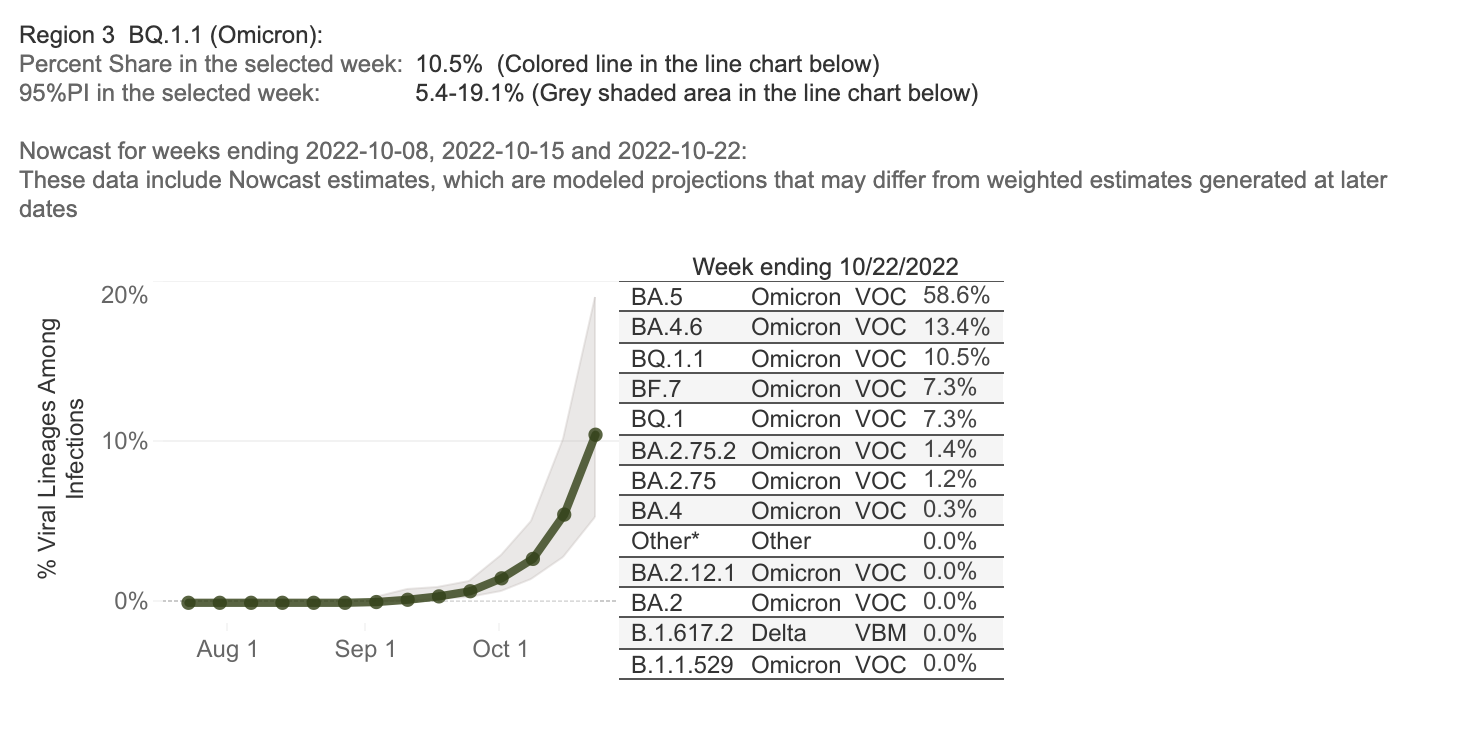
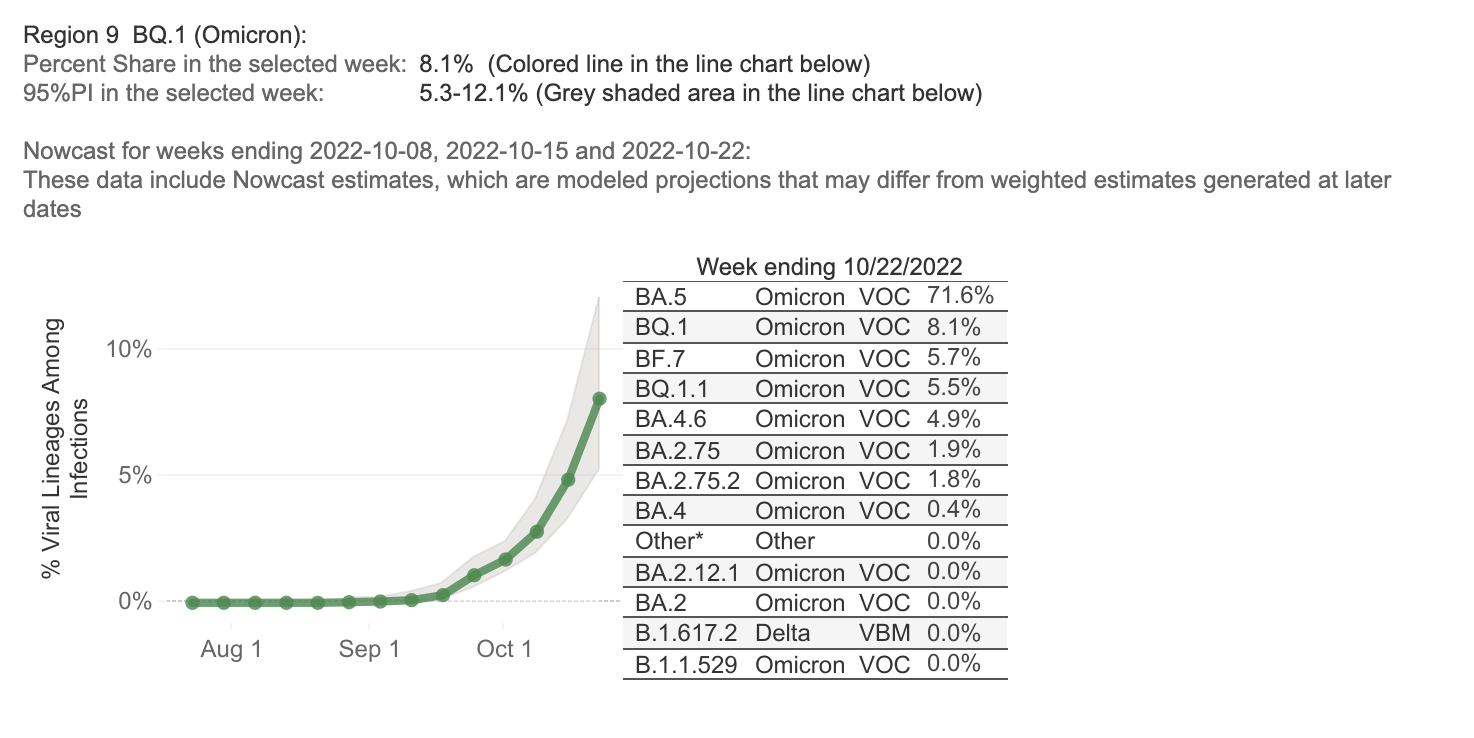
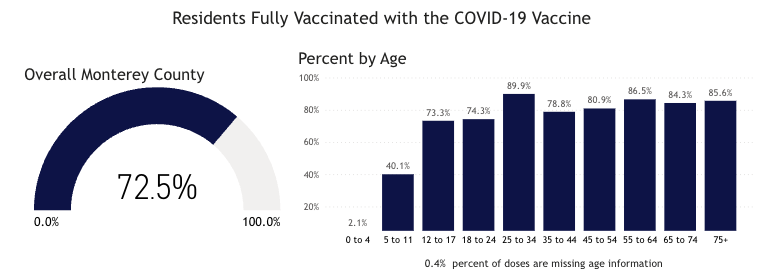
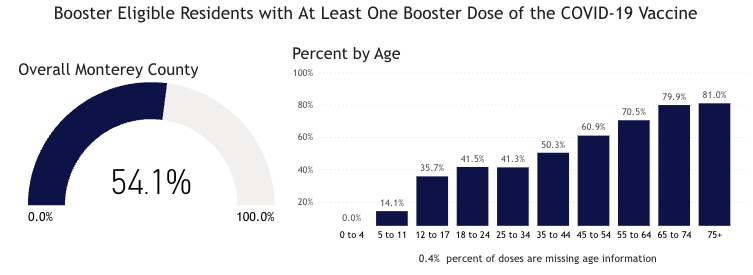

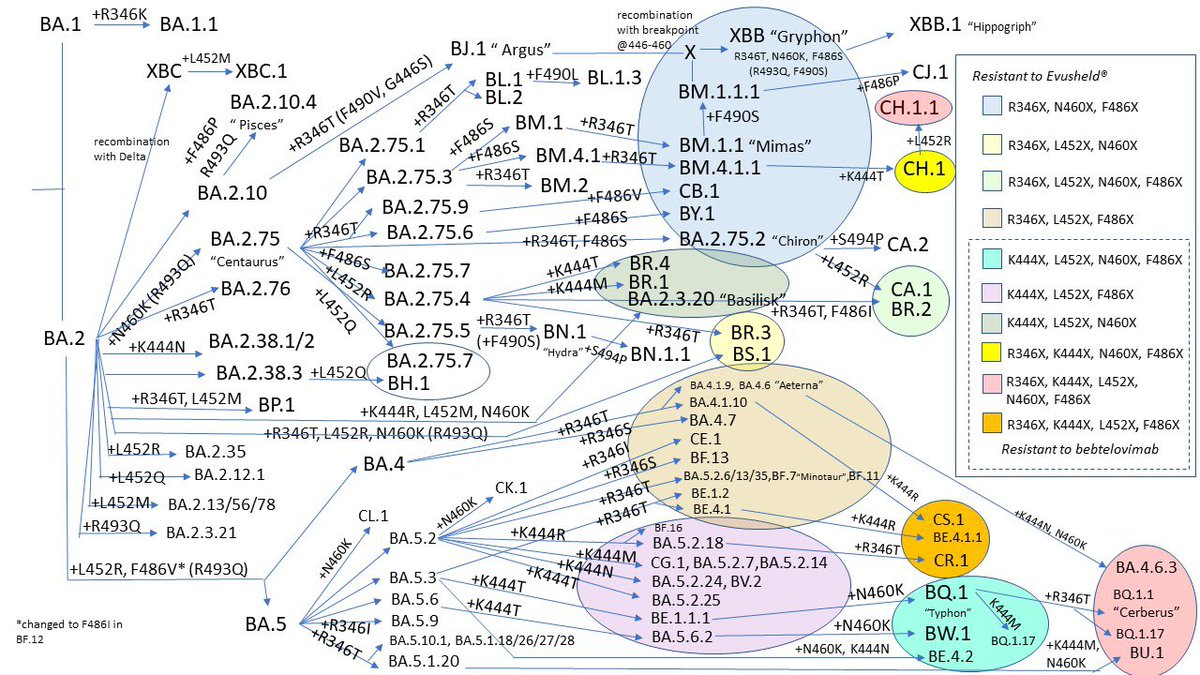

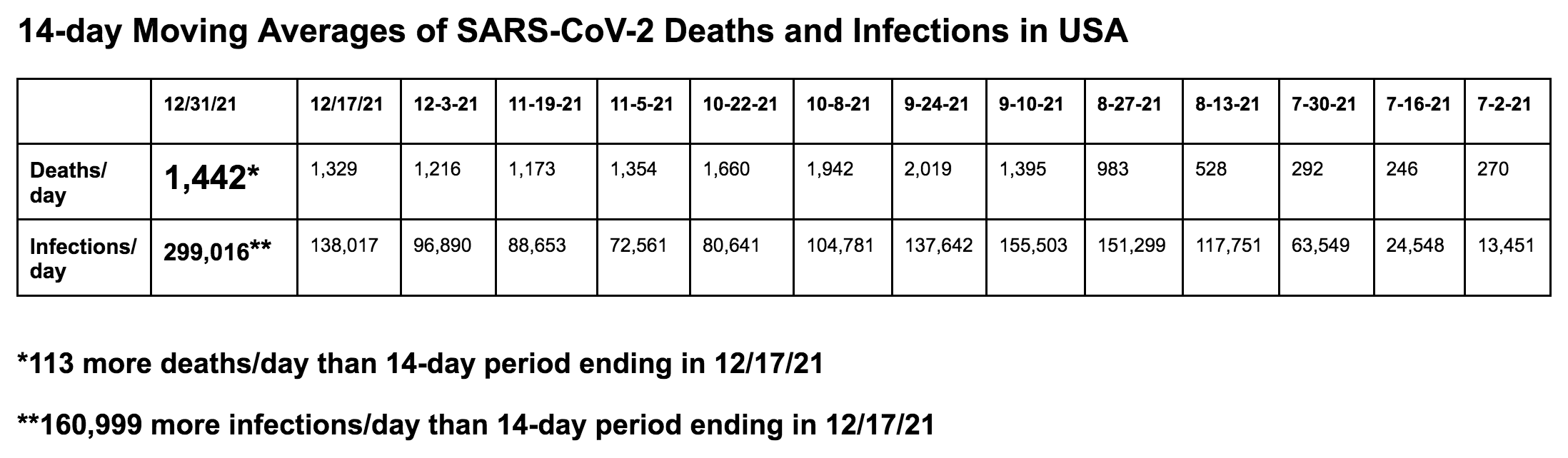


































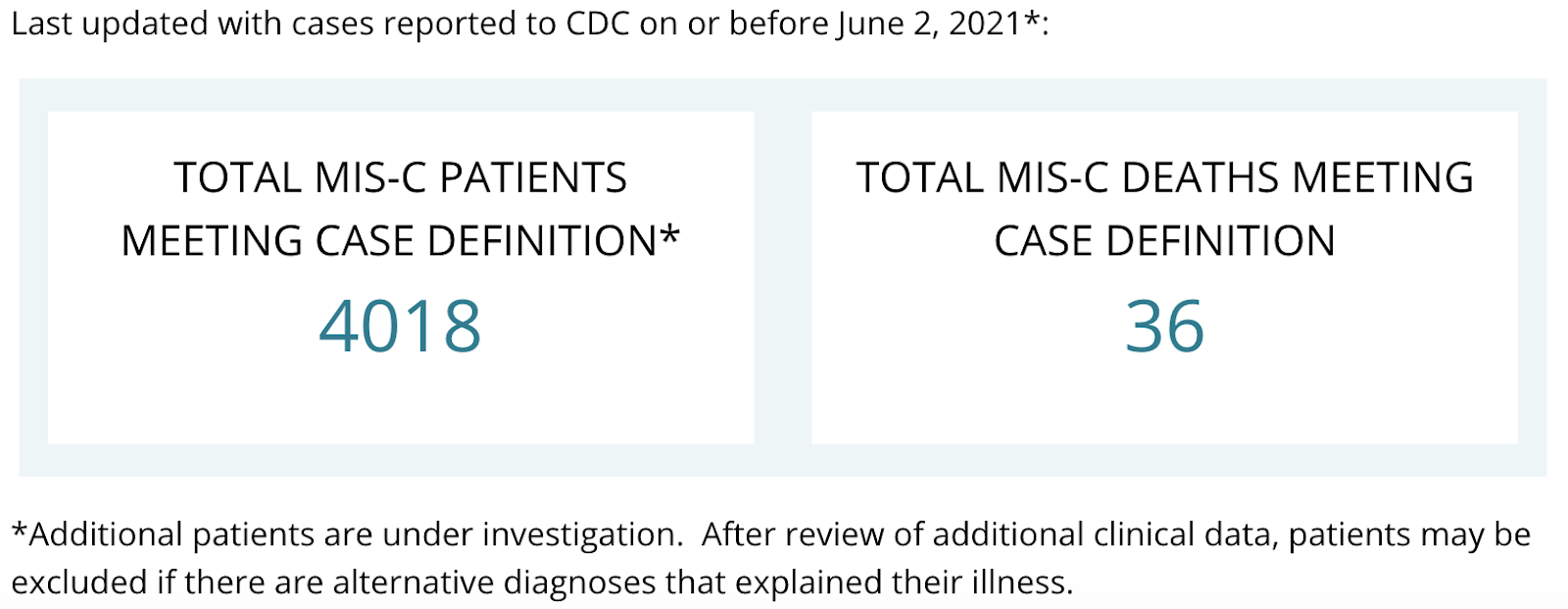


















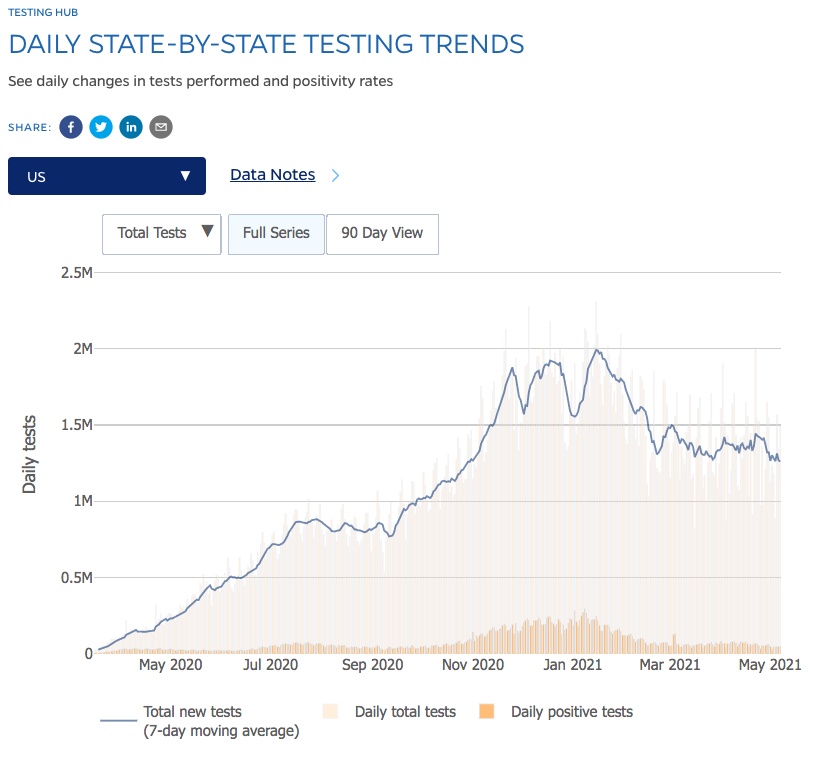

You must be logged in to post a comment.