
In this update:
- In the United States, daily COVID deaths and infections increased over the last two weeks, with an average loss of 453 lives per day.
- The US government is mailing free COVID test kits again, and US residents can anonymously report the results of at-home tests to NIH.
- Immune-escaping BQ variants continue to dominate in the US, though recombinant XBB lineages, which have been demonstrated to evade neutralizing antibodies in vaccinated people, are on the rise.
- Bivalent booster uptake is still insufficient to protect the US population this winter, with only 14.1% of the population up to date on COVID vaccines.
- In Monterey County, just over half of the population has received three vaccine doses, and only 16.1% have received the bivalent booster.
- Dr. Wright continues to recommend that everyone wear N95 or P100 masks when gathering indoors. This will help protect not only against COVID-19, but also against other respiratory viruses that are on the rise around the country, including RSV, flu, and measles. Anyone who is not up to date on flu and measles vaccines should get vaccinated as soon as possible.
Don’t want to miss an update?
Get the latest COVID updates from Dr. Wright delivered to your inbox as soon as they’re published!
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.

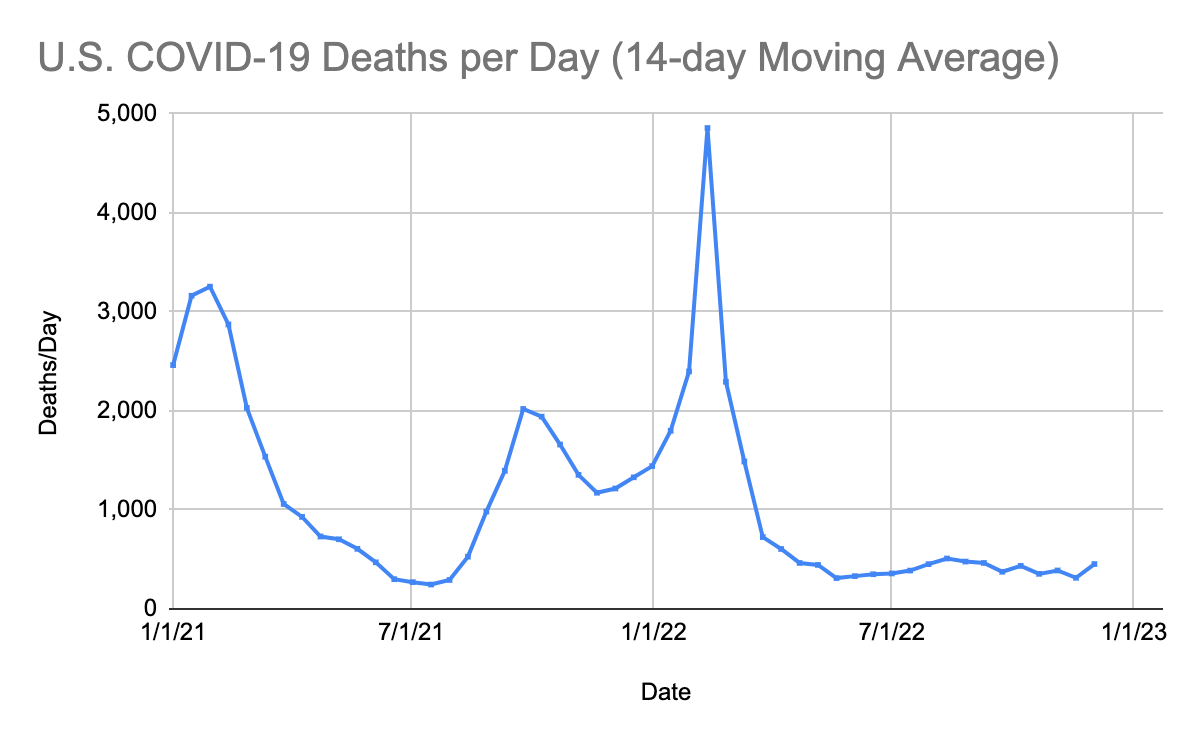
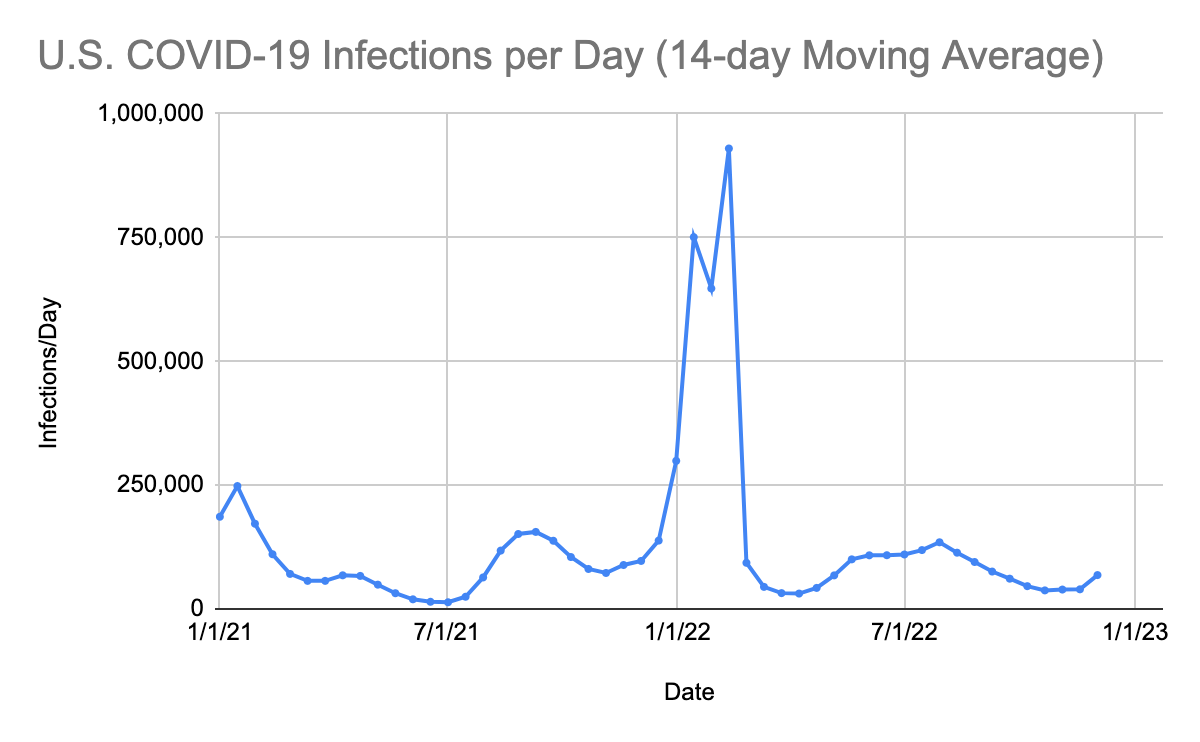
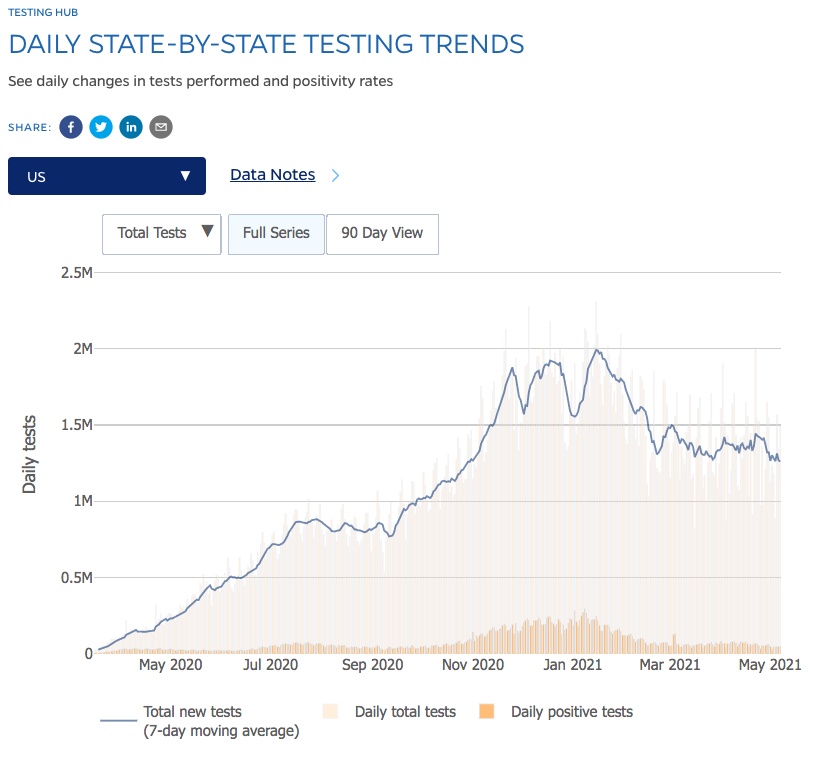
SARS-CoV-2 infections per day in the United States have increased for the fourth time in 8 weeks. There is still widespread underreporting by states, a failure to capture all positive home tests, and a decreased PCR screening program in most states. Deaths per day in the United States have increased by 157 deaths per day. Many states are not reporting deaths or infections in a timely manner. The number of infections per day has increased by 23,190 due to the lack of mask use in schools, businesses, and airports; a failure of adequate building ventilation; lack of social distancing; and low rates of bivalent booster uptake. Continued infection and death increases are expected in the next four weeks with 113 million people expected to travel during the holiday season. In late November of this year, the National Institutes of Health launched MakeMyTestCount.org, a website that allows users to anonymously report the results of at-home COVID tests. Unfortunately, it has thus far not been widely publicized. The US government has begun mailing free test kits again. Go to the following website to obtain free test kits: https://special.usps.com/testkits
Drug-Evading Mutants Continue to Dominate the Variant Soup
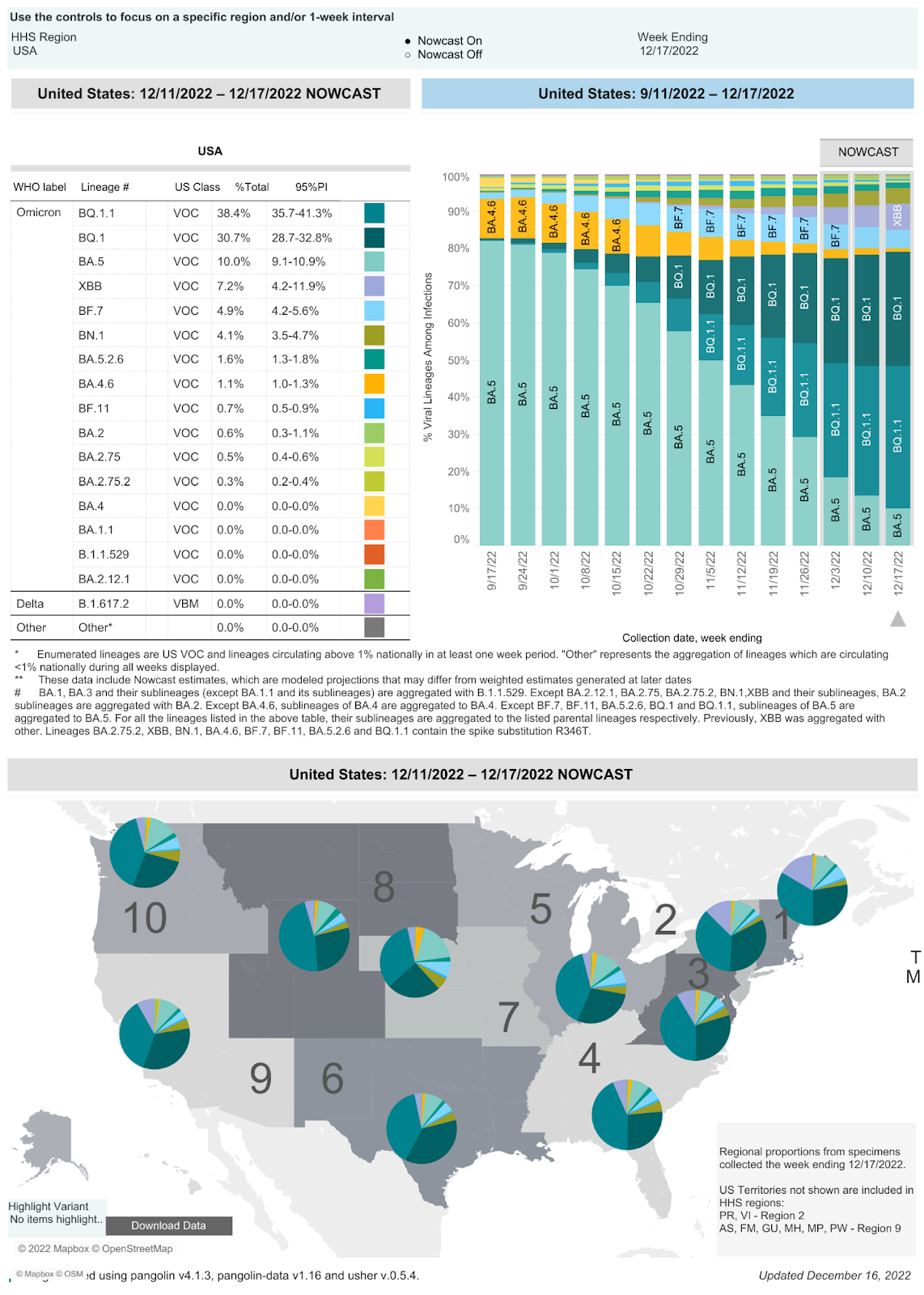
On 12/17/22 the CDC estimates that BA.5 accounted for 10% of infections (a 42.4% drop from 10/21/22), BQ.1 accounted for 30.7% (a 21.3% increase since 10/21/22), BQ.1.1 accounted for 38.4% (a 31.2% increase since 10/21/22), BA.4.6 accounted for 1.1% (a 8.4% decrease from 10/21/22), BF.7 accounted for 4.9% (a 4.1% decrease from 10/21/22), BN.1 accounted for 4.1% of isolates (a 1% decrease since 1/19/22), and BA.2.75.2 accounted for 0.3%. In the last four weeks, three isolates were added to the CDC’s reporting: XBB (7.2% an increase of 1.7% since 12/2/22), BA.5.2.6 (1.6% a decrease of 0.2% since 12/2/22), and BF.11 (0.7% decrease of 0.2% since 12/2/22). In the week ending December 17, 2022, BQ isolates accounted for 69.1% of infections (a 33.8% increase in infections caused by these BQ variants since 10/21/22). BQ.1.1 has five spike mutations that are different from BA.5. Four of these mutations allow escape from immunity from monoclonal antibodies, any prior infection (including Omicron BA.5), or any vaccine to include the bivalent Omicron BA.5 vaccine. Infections are occurring in our clinic in patients that received the Omicron BA.5 bivalent vaccine.
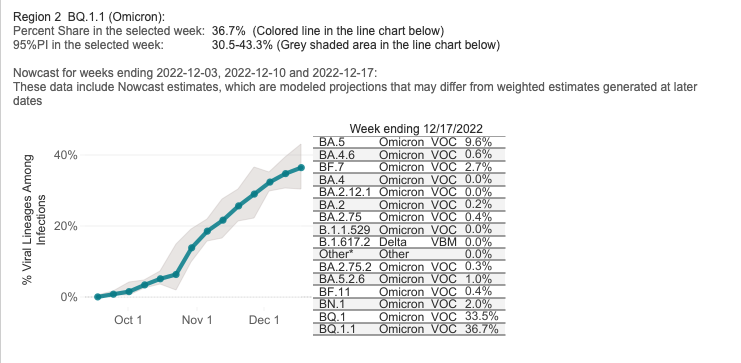
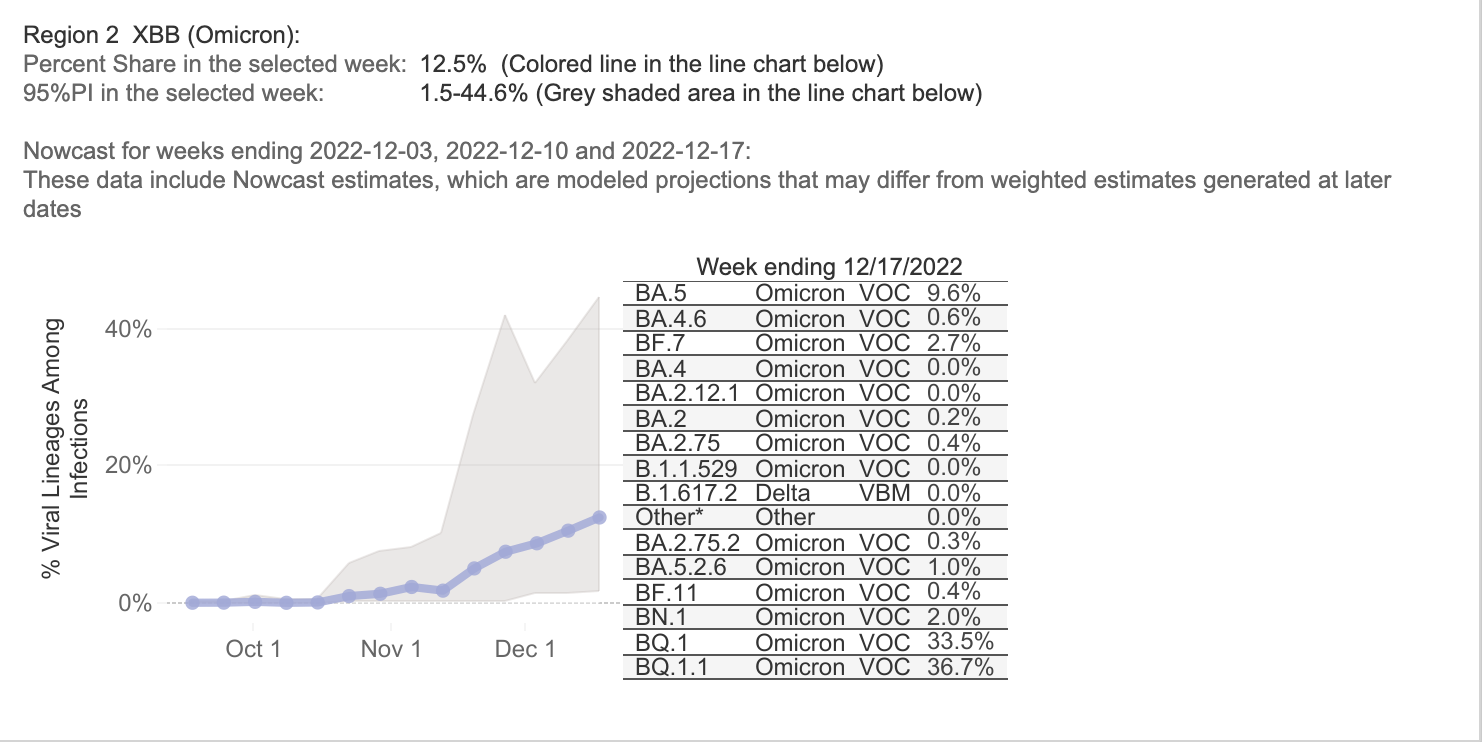
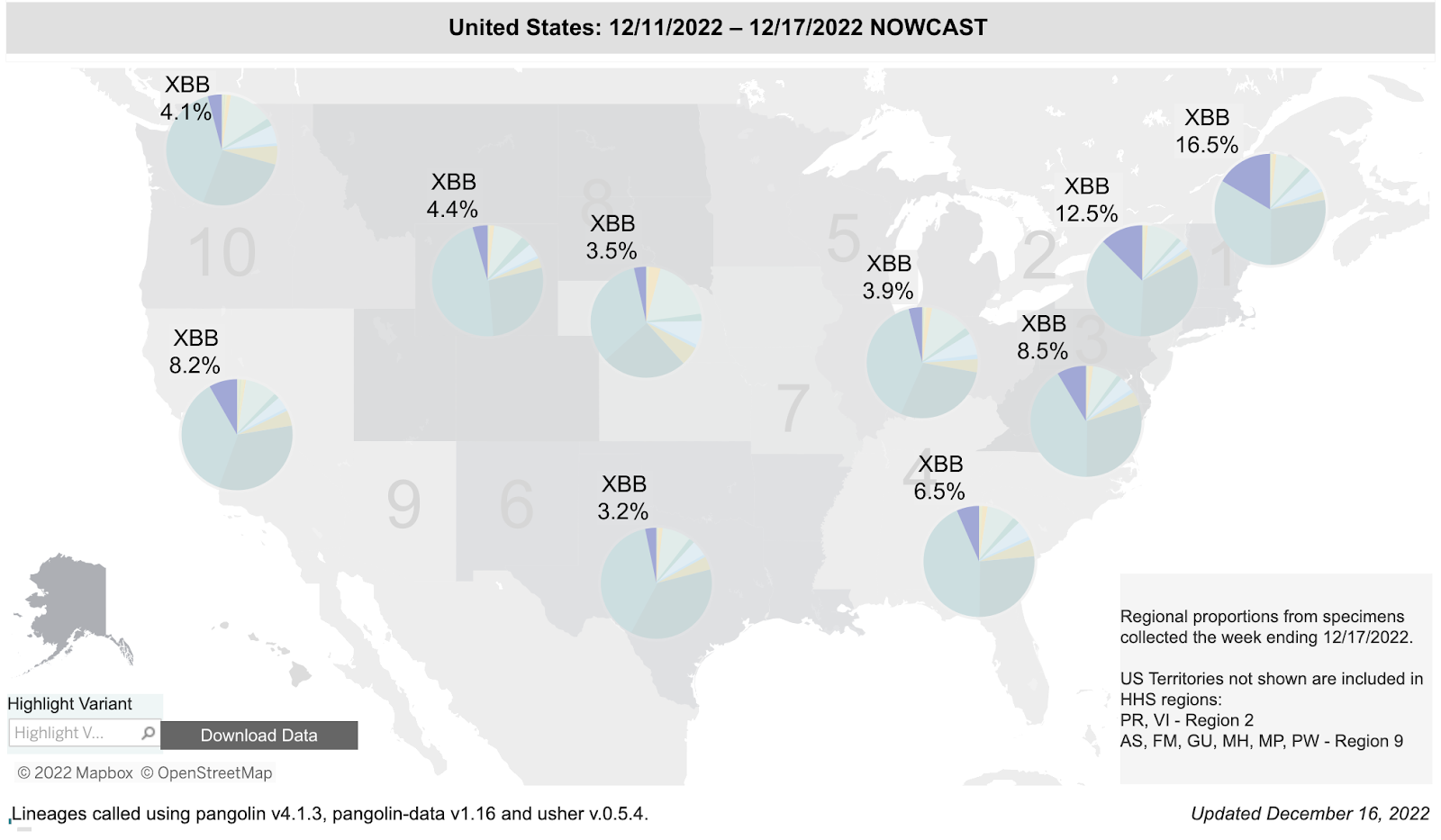
The total percentage of BQ variant infections in the region that includes New York and New Jersey was 72.4% two weeks ago and is now 70.2%. BA.5 accounts for 9.6% of infections, BF.7 accounts for 2.7%, BN.1 accounts for 2.0%, BA.5.2.6 accounts for 1%, and BA.2.75 lineages account for 0.7% of infections. XBB isolates (STILL not shown in above chart) are 12.5% of isolates in Region 2 (see below).
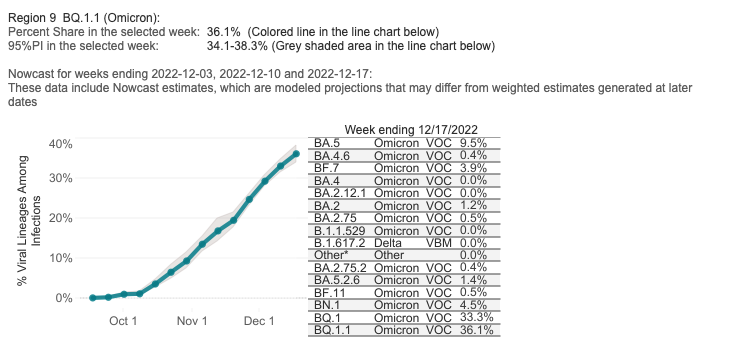
The total percentage of BQ variant infections in the region that includes California, Nevada, Arizona, and Hawaii was 62.6% on 12/3/22 and is now 69.4%. BA.5 accounts for 9.5% of isolates, and BA.5.2.6 accounts for 1.4%. The BA.2.75 lineages account for 1.2%. BF.7 accounts for 3.9%, BN.1 accounts for 4.5%, and BA.2 isolates account for 1.2%. Again, CDC is not reporting XBB in the Region 9 chart above. XBB isolates are 8.2% of isolates in region 9.
Data on the rapid spread of a dangerous variant category, the BQ variants, was withheld by the CDC in their weekly reports until seven weeks ago. This data on BQ.1 and BQ.1.1 should have been disclosed earlier.
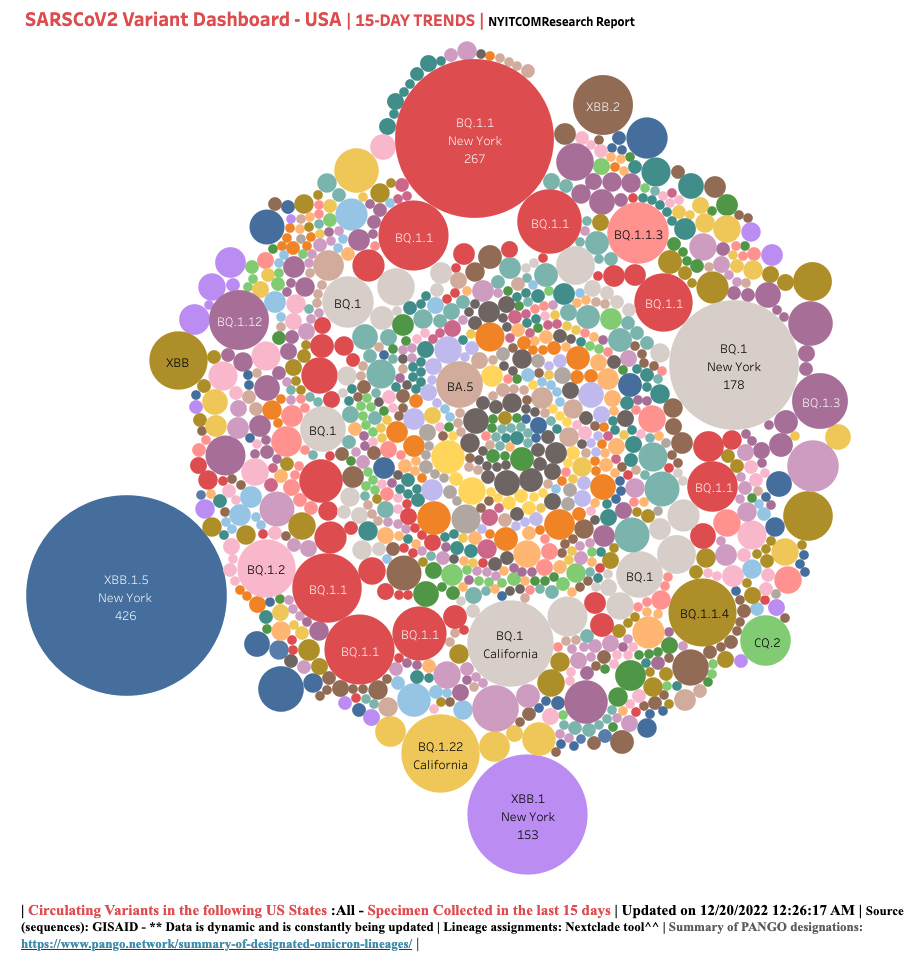
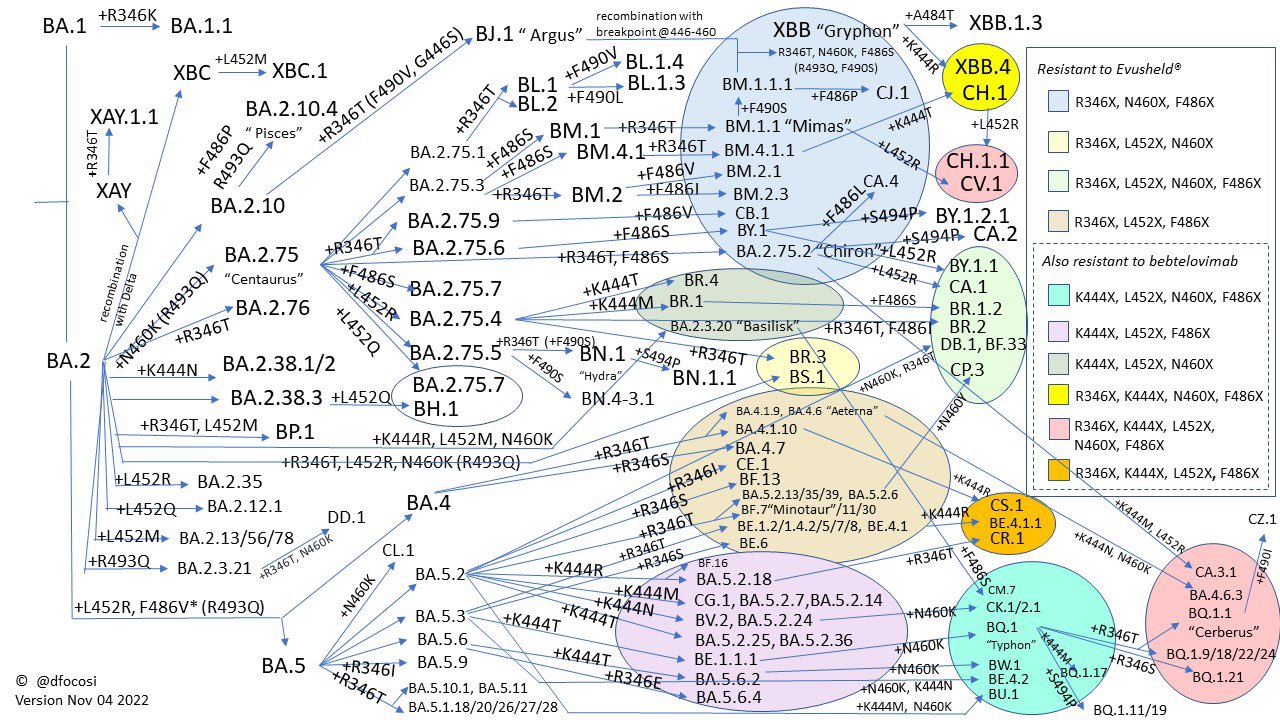
For a more detailed picture of COVID variant evolution in the United States, we recommend checking out the dashboard put together by Raj Rajnarayanan, Assistant Dean of Research and Associate Professor at NYITCOM at Arkansas State University. We can see that XBB already has a few subvariants that are gaining prevalence in New York.
To understand the true impact of these variants, it’s helpful to examine their evolution. Two virologists collaborated on Twitter to create the figure below, which Professor Johnson titled “Convergent Evolution on Steroids.” It shows the key mutations present in many of the currently-circulating Omicron subvariants and demonstrates that mutation at site 346 is becoming more and more common.
Past infections with a BA.1, BA.2 or BA.5 variants will not prevent infections with any of the newer variants. Monoclonal antibodies are no longer effective against newer BQ variants and other spike protein mutated variants. The last remaining monoclonal antibody, bebtelovimab, was removed from use by the FDA on 12/2/22. Paxlovid was only 89% effective in the original clinical trials against SARS-CoV-2. If resistance develops this winter to oral Paxlovid, we will have more Paxlovid failures and increased hospitalizations and deaths.
The November 25 UK Health Security Agency Technical Briefing identifies lineages BA.5, BA.5.2.35, BA.5.7, BQ.1, BQ.1.1, XBB, and BN1 (BA.2.75.5.1) as isolates of concern.
| Variant | Sublineage of | Mutations | Global Sequences outside UK | UK Sequences |
| BQ.1 | BA.5 | L452RN460KK444T | 33,206 (81 countries) | 9,285 (> 40% of all sequenced samples) |
| BQ.1.1 | BA.5 | N460KK444TR346T | 17,621(70 countries) | 4,715 |
| BA.5.2.35 | BA.5.2 | R346T, 2 synonymous single nucleotide polymorphisms (SNPs) G28423C and C7006T | 447 | 848 |
| BN.1 | BA.2.75.5 | R346T F490S | 1,127 | 190 |
| XBB | Recombinant of BJ.1 and BM.1.1.1 (both descended from BA.2), approximate break point between spike mutations G446S and N460K | E: T11A, Spike: V83A, H146Q, Q183E, F486S, F490S.Spike mutations inherited from BJ.1 are G339H, R346T, V445P, G446S and from BM.1.1.1 areN460K, F486V, F490S, and R493Q | 4,831 (51 countries) | 345 |
Disappointing Vaccine Uptake, Especially Among Children
Our monoclonal antibody therapies do not work for these isolates, but these emerging BQ variants are descendants of BA.5, so the new BA.5 bivalent vaccine should offer some protection, when combined with an N95 mask. It’s troubling that, despite the availability of this vaccine, few people are getting vaccinated. As of December 14, 2022, the CDC reports that 44,154,294 people in the United States (5 years and up) have received the bivalent vaccine. That’s only 19.4% of people (5 and up) who received the primary series and 14.1% of the overall population.
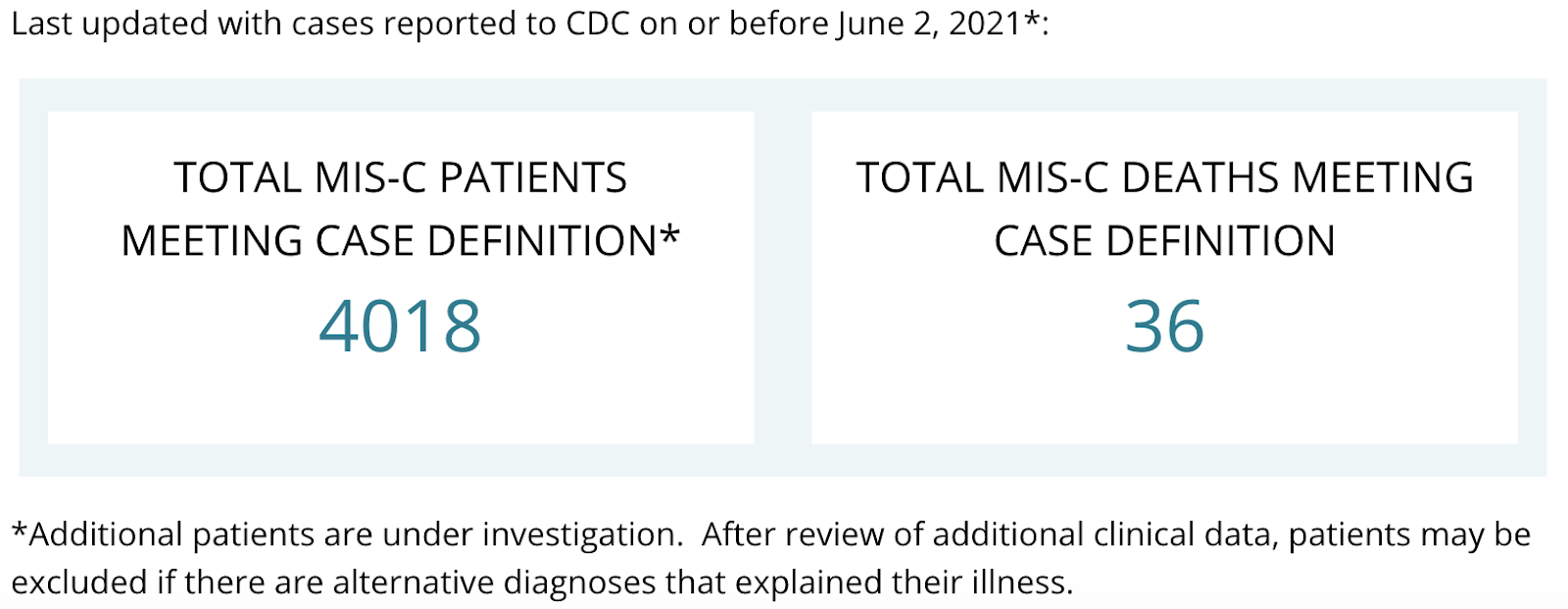
Children under the age of 5 have not been approved to receive either Omicron BA.5 mRNA booster. Sadly, in children between 0 and 5 years of age only 1.61 million have received at least one dose of any SARS-CoV-2 mRNA vaccine based on the original Wuhan isolate. In the United States, at least 1,390 children have died of COVID-19, and another 74 have died of multisystem inflammatory syndrome (MIS-C). Worldwide, according to UNICEF, over 16,100 children and young adults aged 0-20 have died of COVID-19.
The Monterey County Health Department reports that, as of 12/19/22, 3.7% of 0-4 year-olds and 40.2% of 5-11 year-olds have received the first two doses of vaccine, while 73.4% of 12-17 year-olds have received two doses. Only 55.5% of Monterey County residents have received a third dose of the vaccine. The Monterey County Health Department does not publish data on how many residents have received the new BA.5 bivalent booster vaccine, but the Monterey Weekly reported on December 8 that only 16.1% of county residents had received it. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. All Monterey County residents should get up to date on COVID-19 vaccinations, including the bivalent BA.5 booster, as soon as possible.
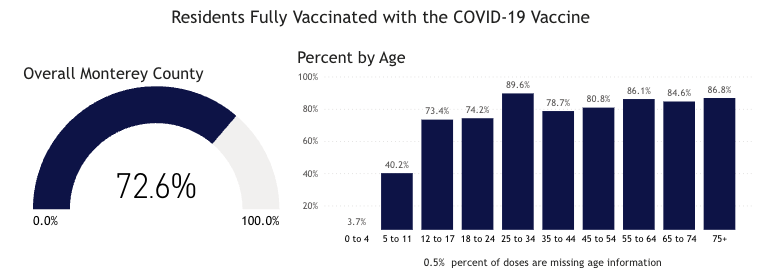
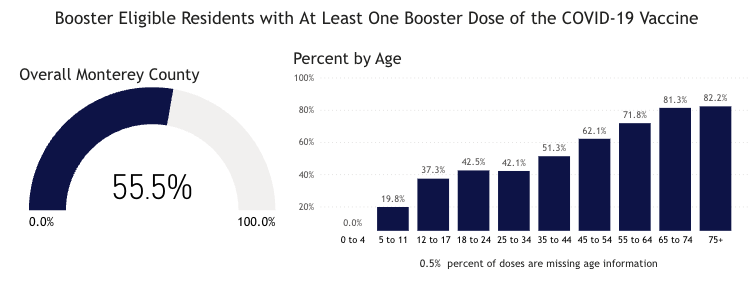
Source: Monterey County Health Department
Mask Up to Protect Against Additional Viral Threats This Winter
In a new preprint on respiratory syncytial virus (RSV) in young children, researchers from Case Western University write, “Among RSV-infected children in 2022, 19.2% had prior documented COVID-19 infection, significantly higher than the 9.7% among uninfected children, suggesting that prior COVID-19 could be a risk factor for RSV infection or that there are common risk factors for both viral infections.” Wearing a well-fitting, high-filtration mask not only protects against COVID but also protects against other viruses like RSV, influenza, and measles. The recent surge in respiratory infections among children that has overwhelmed hospitals around the country is most certainly a result of the removal of mask mandates throughout the United States. A new study of COVID infection data in Massachusetts public schools from February to June 2022, after many districts rescinded mask mandates, shows that “the lifting of masking requirements was associated with an additional 44.9 cases per 1000 students and staff,” compared to in schools where mask requirements were upheld. The authors explain that the districts which kept mask requirements in place were ones that tended to have less updated buildings and whose student populations had a greater percentage of low-income families, students with disabilities, English learners, and Black and Latinx students. As such, they conclude, “we believe that universal masking may be especially useful for mitigating effects of structural racism in schools, including potential deepening of educational inequities.” This is something that we’ve been saying since the beginning of the pandemic; removing nonpharmaceutical interventions always disproportionately harms the most vulnerable members of our society.
Two weeks ago, we mentioned an Arstechnica report that the state of Ohio had had 54 cases of measles this year, 50 of which were in the Columbus area, 20 of which required hospitalization, and all of which were in unvaccinated people. As of December 20, the number of measles cases in Central Ohio has risen to 81, and 29 of these have been hospitalized.
As of December 15, the CDC has reported 106 cases of measles in the United States in five (undisclosed) jurisdictions. We’re certain that with no airborne disease mitigations for holiday travel, measles cases will increase over the next month.
A Deeper Dive into U.S. COVID Data
On 12/16/22, the United States had 28,877 documented new infections. There were also 147 deaths. Thirty-five states did not report their infections, and 36 states didn’t report their deaths. In the United States on 12/17/22 the number of hospitalized patients (40,374) has increased (+16.5% compared to the previous 14 days) and was 34,646 on December 2. On 12/17/22 there were 4,627 patients who were seriously or critically ill (a 15.5% increase); that number was 4,005 two weeks ago. The number of critically ill patients has increased by 643 in the last 14 days, while at least 4,168 new deaths occurred. The number of critically ill patients has increased for the eighth time in thirty-two 14-day periods. Patients are still dying each day (average 298/day).
As of 12/16/22, we have had 1,112,944 deaths and 101,743,845 SARS-CoV-2 infections in the United States. We have had 956,066 new infections in the last 14 days. We are adding an average of 478,033 new infections every seven days. For the pandemic in the United States we are averaging one death for every 91.41 infections or over 10,939 deaths for each one million infections. As of 12/16/22, thirty-nine states have had greater than 500,000 total infections, and 38 states and Puerto Rico have had greater than 5,000 total deaths. Forty-six states have had greater than 2,000 deaths, and 33 states have greater than 3,000 deaths per million population. Eight states have over 4,000 deaths per million population: Mississippi (4,389), Arizona (4,387), Alabama (4,223), West Virginia (4,275), New Mexico (4,179), Tennessee (4,160), Arkansas (4,194) and Michigan (4,056). Eighteen states (Alabama, Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Eight states have had greater than 40,000 deaths: Florida (83,380 deaths), Texas (92,108 deaths), New York (74,759 deaths), Pennsylvania (48,662 deaths), Georgia (41,244 deaths), Ohio (40,747 deaths) , Illinois (40,502 deaths), Michigan (40,508), and California (98,034 deaths, 20th most deaths in the world).
On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. Since 11/20/20 (25 months), there were 845,843 new deaths from SARS-CoV-2. For twenty-one of those months, vaccines have been available to all adults. During these twenty-one months, 540,845 people have died of SARS-CoV-2 infections. Clearly, a vaccine-only approach is not working anywhere, especially not in the United States. In addition to getting more people vaccinated, most of the hospitalizations and deaths could have been prevented by proper masking (N95 or better), social distancing, and treatment with oral antiviral agents like Paxlovid. We recommend all of these precautions and treatments to every patient in our clinic, and we have only lost one patient to COVID in 2.5 years.
As of 12/16/22, California was ranked 33rd in the USA in infection percentage at 29.45%. In California, 25.48% of the people were infected in the last 21 months. As of 12/16/22, 29 states have had greater than 30% of their population infected. Fifty states, the District of Columbia and Puerto Rico have greater than 20% of their population infected.
Worldwide, average deaths per day are 1,760 for the last 14 days. The United States accounts for 25.73% (453 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 546,064 the last two weeks. The United States accounts for 12.50% of those infections (or 68,294 infections per day).
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Watching World Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
| Location | Total Infections as of 12/16/22 | New Infections on 12/16/22 | Total Deaths | New Deaths on 12/16/22 | % of Pop.Infected | SARS-CoV-2 Isolates Currently Known in Location | National/ State Mask Mandate | Currently in Lockdown |
| World | 656,953,845(7,644,889 new infections in 14 days). | 473,615 | 6,669,730(24,636 new deaths in last 14 days) | 1,104 | 8.42% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1 (USA)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BF.7BJ.1XBBBQ.1BQ.1.1BS.1BN.1 | No | No |
| USA | 101,743,845(ranked #1) 956,066 new infections in the last 14 days or 68,294/day. | 28,877(ranked #5) 35 states and D,C. failed to report infections on 12/2/22. | 1,112,944(ranked #1) 6,337 new deaths reported in the last 14 days or 388/day. | 147 33 states and D.C. failed to report deaths on 12/2/22. | 30.38% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BQ.1BQ.1.1BN.1 | No | No |
| Brazil | 35,874,528(ranked #5) 498,995 new infections in the last 14 days. | 64,696 (ranked#3) | 691,776(ranked #2; 1,647 new deaths in 14 days) | 124 | 16.65% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21) | No | No |
| India | 44,676,911(ranked #2); 2,716 new infections in 2 weeks. | 220 | 530,663(ranked #3) 36 new deaths in 2 weeks. | – | 3.17% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India) | No | No |
| United Kingdom | 24,053,576(ranked #9) 28,830 new infections in 2 weeks. | – | 197,723 (ranked #7) 470 new deaths in 2 weeks | – | 35.11% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22) | No | No |
| California, USA | 11,639,487(ranked #13 in the world; 155,919 new infections in the last 14 days). | 3,235 | 98,034 (ranked #20 in world) 176 new deaths in the last 14 days | 20 | 29.45% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BQ.1BQ.1.1BN.1 | No | No |
| Mexico | 7,174,464(ranked #19) 41,672 new infections in 14 days). | – | 330,743(ranked #5)218 new deaths in 14 days) | – | 5.45% | No | No | |
| South Africa | 4,046,568(ranked #37; 4,347 new infections in 14 days). | 418 | 102,568 (ranked #18) 104 new deaths in 14 days) | – | 6.66% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.4 (South Africa 11/21)BA.5 (South Africa 11/21) | No | No |
| Canada | 4,440,839(ranked #34) 32,563 new infections in 14 days). | – | 48,353(ranked #25 ) 572 new deaths in the last 14 days | – | 11.56% | No | No | |
| Poland | 6,360,843 (ranked #21; 6,993 new infections in 14 days). | 604 | 118,419 (ranked #15)87 new deaths in the last 14 days | 7 | 16.85% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3 | No | No |
| Russia | 21,701,321 (ranked #10), 103,708 new infections in 14 days). | 8,451 (ranked #10) | 392,891(ranked #4)831 new deaths in 14 days | 59 | 14.88% | No | No | |
| Peru | 4,405,843(ranked #35, 139,592 new infections in 14 days). | 6,770 (ranked #11) | 217,821(ranked #6) 393 new deaths in the last 14 days | 39 | 13.07% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Iran | 7,560,372(ranked #18; 635 new infections in last 14 days) | 49 | 144,659(ranked #12) 25 new deaths in the last 14 days | – | 8.78% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Spain | 13,651,239(ranked #12; 39,187 new infections in 14 days). | 2,656 (ranked #15) | 116,658 (ranked #16)577 new deaths in 14 days | 32 | 29.21% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| France | 38,801,884 (ranked #3; 885,832 new infections in the last 14 days). | 56,361 (ranked #4) | 160,359 (ranked #10)1,333 new deaths in 14 days. | 131 | 59.16% a 1.35% increase in 14 days. | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinantBQ.1.1 | No | No |
| Germany | 36,980,882(ranked #4; 450,862 new infections in 14 days.) | 34,308 (ranked #5) | 159,889 (ranked #11)1,776 new deaths in 14 days | 147 | 44.08% 0.54% increase in 14 days | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinantBQ.1.1 | No | No |
| South Korea | 28,062,679 (ranked #6 906,866 new infections in 14 days). | 66,953(ranked #2) | 31,298 (ranked #35) 730 new deaths in 14 days | 66 | 54.67%1.77% increase in 14 days | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Vietnam | 11,522,431 (ranked #13; 5,942 new infections in 14 days). | 333 | 43,179(ranked #26) | – | 11.64% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Netherlands | 8,556,131 (ranked #16; 12,293 new infections in 14 days). | 868 | 22,943 (ranked #41) | – | 49.71% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Denmark | 3,157,132 (ranked #40) 8,922 new infections in 14 days. | 569 | 7,635(ranked #77 98 new deaths in the last 14 days) | 9 | 54.10% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Taiwan | 8,547,306(ranked #17)218,306 new infections in 14 days | 15,407 (153,602ranked #9) | 14,820 (ranked #58 433 new deaths in the last 14 days) | 24 | 35.77% 0.41% of population has been infected in the last 14 days | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Japan | 26,821,853(ranked #7)1,910,466 new infections in the last 14 days | 156,602(ranked #1) | 52,823(ranked #23) 2,997 new deaths in the last 14 days | 182 | 21.35% 1.52% of the population infected in the last 14 days. | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)BA.2*BA.5* | No | No |
| Argentina | 9,766,975, (ranked #15)39,728 new infections in the last 14 days. | – | 130,041(ranked #14) | – | 21.22% | No | No | |
| Italy | 24,884,034 (ranked #8) 556,370 new infections in the last 14 days. | – | 183,138(ranked #8) 1,405 new deaths in the last 14 days | – | 41.29% 0.93% of population infected in last 14 days. | No | No | |
| Chile | 4,975,862(ranked #28) 50,811 new infections in14 days.. | 4,009 (ranked#13) | 62,822(ranked #22) 338 new deaths in the last 14 days. | 27 | 25.84% 0.56% of population infected in the last 14 days. | No | No | |
| Colombia | 6,330,843(ranked #22) 12,822 new infections in the last 14 days. | – | 141,996(ranked #13) | – | 12.28% | No | No | |
| Australia | 10,966,207(ranked #14) 240,968 new infections in 14 days. | 20,033 (ranked #7) | 16,673(ranked #55) 486 new deaths in 14 days. | 42 | 42.06% 0.82% of population infected in last 14 days. | No | No | |
| Turkey | 17,042,722(ranked #11)37,185 new infections in 14 days. | – | 101,492(ranked #19) 92 new deaths in 14 days.. | – | 19.91% | No | No | |
| Indonesia | 6,707,504 (ranked #20) 37,683 new infections in last 14 days. | 1,451 | 160,362 (ranked #9) 478 new deaths in the last 14 days. | 27 | 24.03% | No | No | |
| Malaysia | 5,016,023 (ranked #27) 21,480 new infections in the last 14 days. | 1,138 | 36,795 (ranked #29) 107 new deaths in the last 14 days. | 8 | 15.05% | No | No | |
| Hong Kong | 2,323,123(ranked#44) 194,741 new infections in the last 14 days. | 15,726 (ranked #8) | 11,107 (ranked#64)345 new deaths in the last 14 days. | 32 | 30.55% 2.57% of population infected in the last 14 days. | No | No | |
| China | 374,075 (ranked #98) 50,389 new infections in 14 days | 2,157 (ranked#19) | – | – | – | – | – |
What Our Team Is Reading This Week
- SARS-CoV-2 infection and persistence in the human body and brain at autopsy (Nature) https://doi.org/10.1038/s41586-022-05542-y
- Lifting Universal Masking in Schools — Covid-19 Incidence among Students and Staff (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMoa2211029
- FDA Announces Bebtelovimab is Not Currently Authorized in Any US Region (FDA) https://www.fda.gov/drugs/drug-safety-and-availability/fda-announces-bebtelovimab-not-currently-authorized-any-us-region
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 48, 25 November 2022 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1120304/technical-briefing-48-25-november-2022-final.pdf
- Omicron sublineage BQ.1.1 resistance to monoclonal antibodies (The Lancet) https://doi.org/10.1016/S1473-3099(22)00733-2
- SARS-CoV-2 Infection and Increased Risk for Pediatric Stroke (Pediatric Neurology) https://www.pedneur.com/article/S0887-8994(22)00210-7/fulltext
- Single-cell multiomics revealed the dynamics of antigen presentation, immune response and T cell activation in the COVID-19 positive and recovered individuals https://doi.org/10.3389/fimmu.2022.1034159
- Novel treatment combining antiviral and neutralizing antibody-based therapies with monitoring of spike-specific antibody and viral load for immunocompromised patients with persistent COVID-19 infection (Experimental Hematology & Oncology) https://ehoonline.biomedcentral.com/articles/10.1186/s40164-022-00307-9
- Covid-19 is a leading cause of death in children and young people ages 0-19 years in the United States (Preprint) https://doi.org/10.1101/2022.05.23.22275458
- Post-COVID-19-associated morbidity in children, adolescents, and adults: A matched cohort study including more than 157,000 individuals with COVID-19 in Germany (PLOS Medicine) https://journals.plos.org/plosmedicine/article?id=10.1371%2Fjournal.pmed.1004122
- Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies (Acta Pharmacologica Sinica) https://doi.org/10.1038/s41401-022-00998-0
- Cognitive Deficits in Long Covid-19 (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMcibr2210069
- Brain 18F-FDG PET imaging in outpatients with post-COVID-19 conditions: findings and associations with clinical characteristics (European Journal of Nuclear Medicine and Molecular Imaging) https://doi.org/10.1007/s00259-022-06013-2
- Acute and postacute sequelae associated with SARS-CoV-2 reinfection (Nature) https://doi.org/10.1038/s41591-022-02051-3
- Associations between indoor relative humidity and global COVID-19 outcomes (Journal of the Royal Society) https://doi.org/10.1098/rsif.2021.0865
- Successful treatment of prolonged, severe COVID-19 lower respiratory tract disease in a B-cell ALL patient with an extended course of remdesivir and nirmatrelvir/ritonavir (Clinical Infectious Diseases) https://doi.org/10.1093/cid/ciac868
- Impact of SARS-CoV-2 ORF6 and its variant polymorphisms on host responses and viral pathogenesis (Preprint) https://doi.org/10.1101/2022.10.18.512708
- Anti-PF4 antibodies associated with disease severity in COVID-19 (PNAS) https://www.pnas.org/doi/10.1073/pnas.2213361119
- A multinational Delphi consensus to end the COVID-19 public health threat (Nature) https://doi.org/10.1038/s41586-022-05398-2
- Pfizer and BioNTech Announce Updated Clinical Data for Omicron BA.4/BA.5-Adapted Bivalent Booster Demonstrating Substantially Higher Immune Response in Adults Compared to the Original COVID-19 Vaccine https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-updated-clinical-data-omicron
- Paxlovid and Long Covid (Ground Truths, Eric Topol) https://erictopol.substack.com/p/paxlovid-and-long-covid?utm_source=substack&utm_medium=email
- Risk of Infection and Hospitalization Among Children and Adolescents in New York After Emergence of the SARS-CoV-2 Omicron Variant – Comment and Response (JAMA) https://jamanetwork.com/journals/jama/article-abstract/2797231
- Myocarditis (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMra2114478
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 47 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1115077/Technical-Briefing-47.pdf
- Effectiveness of Monovalent mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States — IVY Network, 18 States, December 26, 2021–August 31, 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7142a3.htm
- “Three-dose monovalent mRNA VE estimates against COVID-19–associated hospitalization decreased with time since vaccination. Three-dose VE during the BA.1/BA.2 and BA.4/BA.5 periods was 79% and 60%, respectively, during the initial 120 days after the third dose and decreased to 41% and 29%, respectively, after 120 days from vaccination.”
- Saliva antibody-fingerprint of reactivated latent viruses after mild/asymptomatic COVID-19 is unique in patients with myalgic-encephalomyelitis/chronic fatigue syndrome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.949787
- SARS-CoV-2 Nsp6 causes cardiac defects through MGA/MAX complex-mediated increased glycolysis (Preprint) https://doi.org/10.21203/rs.3.rs-1677754/v1
- WHO’s Therapeutics and COVID-19 Living Guideline on mAbs needs to be reassessed (The Lancet) https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)01938-9/fulltext
- SARS-CoV-2 disrupts host epigenetic regulation via histone mimicry (Nature) https://doi.org/10.1038/s41586-022-05282-z
- Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: an observational study (The Lancet) https://doi.org/10.1016/S0140-6736(22)01586-0
- An ACE2-dependent Sarbecovirus in Russian bats is resistant to SARS-CoV-2 vaccines (PLOS Pathogens) https://doi.org/10.1371/journal.ppat.1010828
- Plasma cytokine levels reveal deficiencies in IL-8 and gamma interferon in Long-COVID (Preprint) https://doi.org/10.1101/2022.10.03.22280661
- Lingering cardiac involvement in previously well people after mild COVID-19 (Nature Medicine) https://www.nature.com/articles/s41591-022-02002-y
- SARS-CoV-2 variants of concern and variants under investigation in England: technical briefing 46 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1109820/Technical-Briefing-46.pdf
- Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients (Ear, Nose, and Throat Journal) https://doi.org/10.1177/01455613221123737
- SARS-CoV-2 Omicron boosting induces de novo B cell response in humans (Preprint) https://doi.org/10.1101/2022.09.22.509040
- Imprinted SARS-CoV-2 humoral immunity induces converging Omicron RBD evolution (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.15.507787v2
- Note: This is a frightening paper and if the conclusions are accurate humans in general are in trouble. From other papers the facts that HERV-M and EBV are activated by SARS-CoV-2 infection does not bode well for humans moving forward.
- SARS-CoV-2 Omicron boosting induces de novo B cell response in humans (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.22.509040v1
- Evolution of antibody immunity following Omicron BA.1 breakthrough infection (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.21.508922v1
- SARS-CoV-2 Spike protein promotes vWF secretion and thrombosis via endothelial cytoskeleton-associated protein 4 (CKAP4) (Signal Transduction and Targeted Therapy) https://www.nature.com/articles/s41392-022-01183-9
- Long-term neurologic outcomes of COVID-19 (Nature Medicine) https://www.nature.com/articles/s41591-022-02001-z
- Pulmonary Dysfunction after Pediatric COVID-19 (Radiology) https://pubs.rsna.org/doi/10.1148/radiol.221250
- Severe Respiratory Illnesses Associated with Rhinoviruses and/or Enteroviruses Including EV-D68 – Multistate, 2022 (CDC) https://emergency.cdc.gov/han/2022/han00474.asp












































You must be logged in to post a comment.