When my daughter, Emily, and I started writing this blog in the spring of 2020, we did not anticipate that almost three years later, there would still be no end in sight for this pandemic. As we begin a new year, we wish we had better news, but the data continues to tell a grim story, and, as our long-time readers know, we always ground our outlook in the numbers.
In the United States, from March 2020 to December 31, 2021, we had 55,696,500 SARS CoV-2 infections and 846,905 deaths (66 infections per death). In the last 12 months we have had an additional 46,813,072 new infections and an additional 271,051 deaths (173 infections per death). That’s an average of 742 deaths per day. The majority of these deaths were in people over the age of 65, and all of them were preventable. In November 2022, KFF reported that COVID-19 was still the number 3 cause of death in the United States. It’s also worth noting that the number one cause of death, cardiovascular disease, is a known complication of COVID.
In late December 2021 the FDA approved both oral Paxlovid and oral Molnupiravir for outpatient treatment of SARS-CoV-2 with distribution beginning in January 2022. Unfortunately, all of the mask mandates were removed by individual states in 2022, and despite President Biden’s vow to institute a federal mask mandate during his 2020 campaign, the President and his administration adopted a decidedly anti-mask policy this year. CDC Director Rochelle Walensky even went so far as to describe masks as “the scarlet letter of this pandemic.” This irresponsible public health messaging has led to thousands of infections and deaths that could have been otherwise prevented by responsible mask wearing. We continue to urge our patients to protect themselves and others by wearing an N95 (or better) mask in public.
This year, multiple new Omicron variants BA.1, BA.2, BA.4, and BA.5 assaulted the world’s population of humans and other animals. By the time multiple companies made and tested Omicron BA.1 vaccines, BA.1 was no longer the dominant variant; in fact, it was no longer present. On August 31, 2022, the FDA allowed rapid introduction of an Omicron BA.5 bivalent vaccine. However, this has had no effect on new immune evading BQ variants. In December the first highly infectious recombinant variant, XBB, began spreading around the world. An additional variant, XBB.1.5, is now rapidly spreading across the country and the world causing increased numbers of hospitalizations and critically ill patients in the USA.
At the same time, we have had outbreaks and deaths from Influenza A H3N2 and RSV. Travel and lack of masking and social distancing have exacerbated the spread of these viruses. In addition, Mpox virus outbreaks occurred nationwide, a measles outbreak began in Ohio in unvaccinated children, and several cases of polio in New York were reported.
Part of why the United States’ vaccine-only approach to COVID-19 is so dangerous is that SARS-CoV-2 mutates, evading immune protection, and spreads more quickly than anyone can make, get approved, and distribute new vaccines. The Omicron BQ.1.1 variant is now being rapidly replaced by XBB.1.5. As an example, at D4 Labs, we designed, manufactured and packaged a new vaccine for Omicron BQ.1.1 in 6 weeks. Minimal animal testing, IRB approval, human testing, and expedited FDA approval under an EUA would probably require at least another 6 months. Even if we skipped or delayed animal testing, obtained IRB approval, and internally did a standard two-dose immunogenicity study in 20 humans using IgG antibody to the RBD of SARS-CoV-2 as the surrogate marker for protection, it would still take three months in our in-house human testing and assay facility to complete the study. This approach would probably not be acceptable to the FDA for even EUA approval but might be attempted in individual states. The timely production and distribution of any new vaccine against any new SARS-CoV-2 mutant will be difficult to accomplish by any company using the current regulatory framework for approval of vaccines in the United States. Using XBB.1.5 as an example, it is responsible for over 40% of the infections in the United States in the last 28 days. Vaccines would have to be designed, manufactured, and distributed in less than four weeks to stop an outbreak of a virulent, highly-infectious respiratory pathogen. Considerable thought needs to be entertained on how to accomplish this task rapidly.
Sadly, we do not see things improving in 2023 for respiratory virus control in the United States unless people wear high quality masks (N95 or better) and practice social distancing again. Continued infection and death increases are expected in the next eight weeks with 113 million people expected to travel during the holiday season, schools reopening on January 2, and people returning to work in poorly ventilated spaces.
Here are our 14-day moving average determinations for SARS-CoV-2 for the United States. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
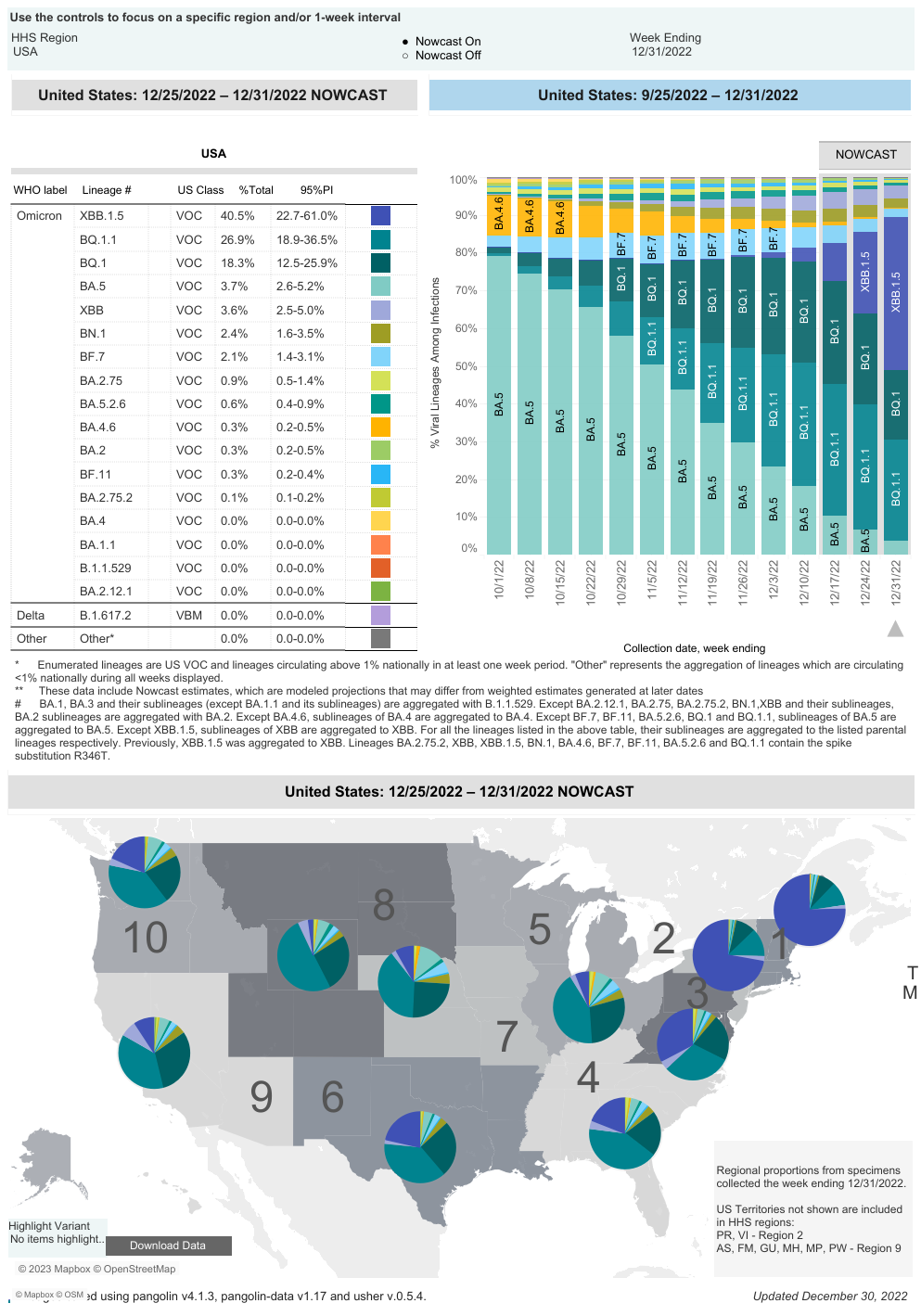
After Delays, CDC Discloses XBB.1.5 Variant Data
On 12/31/22 the CDC estimates that BA.5 accounted for 3.7% of infections (a 49.6% point drop from its peak), BQ.1 accounted for 18.3% (a 12.4% point drop decrease from its peak on 12/17/22), BQ.1.1 accounted for 26.9% (a 11.5% point drop from its peak on 12/17/22), BA.4.6 accounted for 0.3%, BF.7 accounted for 2.1% of infections, BN.1 accounted for 2.4% of isolates,andBA.2.75.2 accounted for 0.1%. XBB is 3.6% of isolates, XBB.1.5 is 40.5% of isolates, BA.5.2.6 is 0.6% of isolates, and BF.11 0.3% of isolates. In the week ending December 31, 2022, BQ isolates accounted for 45.2% of isolates (a 23.9% point decrease in infections caused by these BQ variants since 12/17/22).
CDC
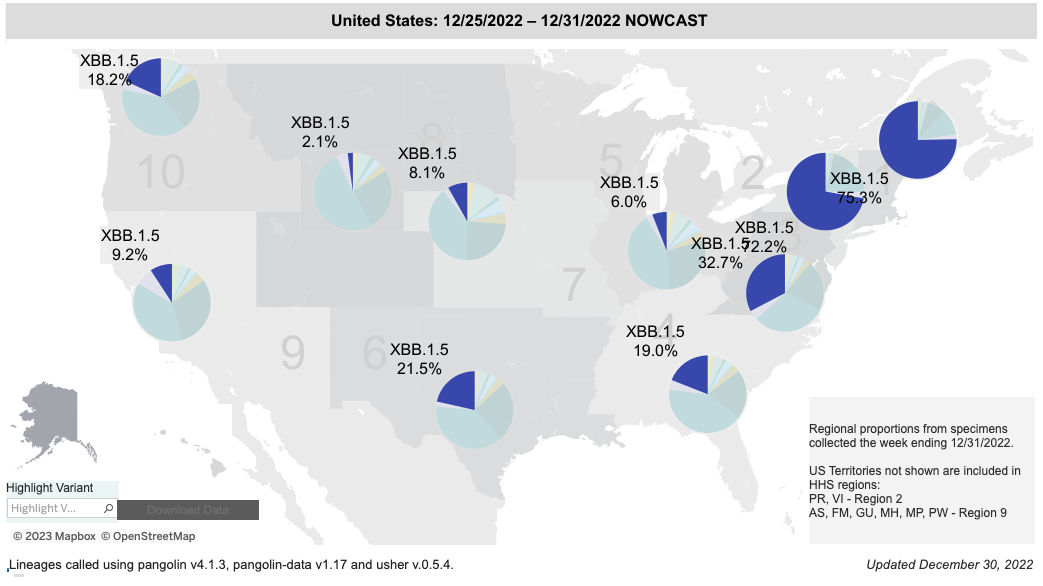
BQ.1.1 has five spike mutations that are different from BA.5. Four of these mutations allow escape from immunity from monoclonal antibodies, any prior infection (including Omicron BA.5), or any vaccine to include the bivalent Omicron BA.5 vaccine. Infections are still occurring in our clinic in patients that received the Omicron BA.5 bivalent vaccine. The XBB recombinant isolate XBB.1.5 has rapidly become the dominant infection in the USA. It took 28 days to become the cause of 40% of infections in the USA and it now causes over 70% of infections in Regions 1 and 2.
XBB.1.5 Proportion of Sequenced Isolates in the USA
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States, and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
Don’t want to miss an update?
Get the latest COVID updates from Dr. Wright delivered to your inbox as soon as they’re published!
SARS-CoV-2 infections per day in the United States have increased for the second time in 16 weeks.There is still widespread underreporting by states, a failure to capture positive home tests, and a decreased PCR screening program in most states. Deaths per day in the United States have decreased by 54 deaths per day. Many states are not reporting deaths or infections in a timely manner. The number of infections per day has increased by 494.In late November of this year, the National Institutes of Health launched MakeMyTestCount.org, a website that allows users to anonymously report the results of at-home COVID tests. Unfortunately, it has thus far not been widely publicized.
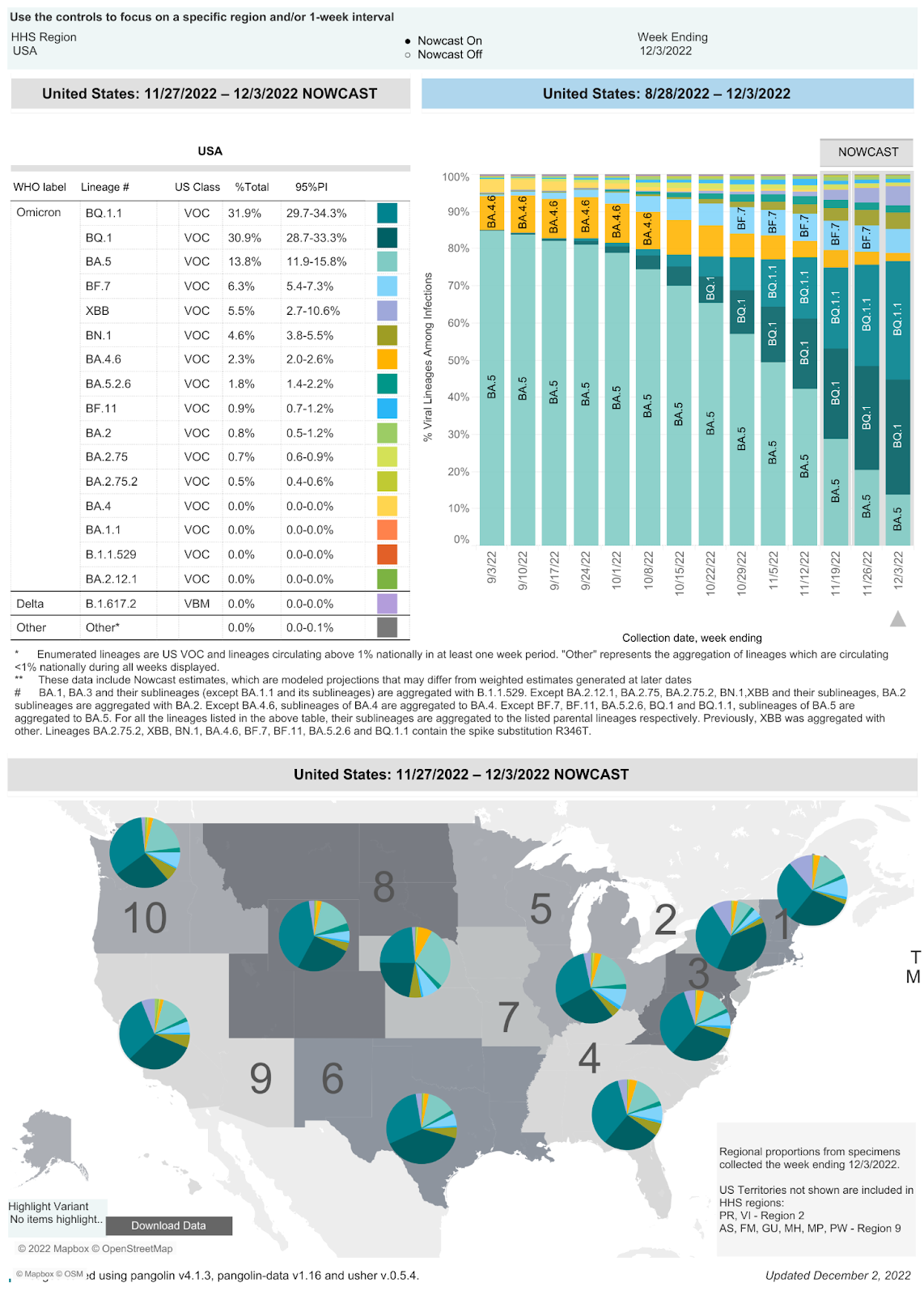
Drug-Evading Mutants Continue to Dominate the Variant Soup
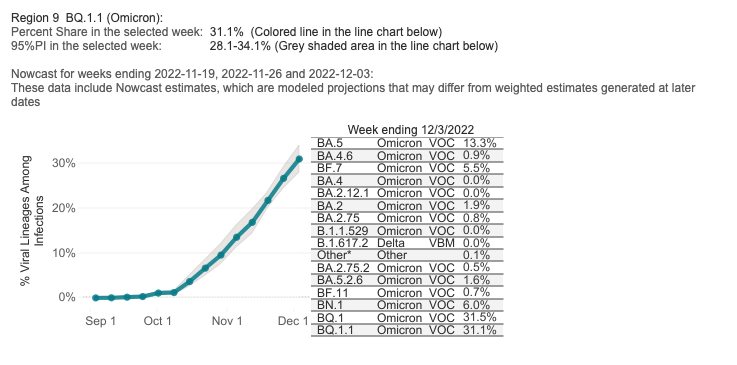
On 12/3/22 the CDC estimates that BA.5 accounted for 13.8% of infections (a 38.6% drop from 10/21/22), BQ.1 accounted for 30.9% (a 21.5% increase since 10/21/22), BQ.1.1 accounted for 31.9% (a 24.77% increase since 10/21/22), BA.4.6 accounted for 2.3% (a 7.2% decrease from 10/21/22), BF.7 accounted for 6.3% (a 2.7% decrease from 10/21/22), BN.1 accounted for 4.6% of isolates (a 0.5% decrease since 1/19/22),andBA.2.75.2 accounted for 0.5%. In the last two weeks, three isolates were added to the CDC’s reporting: XBB (5.5% of isolates), BA.5.2.6 (1.8%), and BF.11 (0.9%). In the week ending December 3, 2022, BQ isolates accounted for 62.8% of infections (a 27.5% increase in infections caused by these BQ variants since 10/21/22). BQ.1.1 has five spike mutations that are different from BA.5. Four of these mutations allow escape from immunity from monoclonal antibodies, any prior infection (including Omicron BA.5), or any vaccine to include the bivalent Omicron BA.5 vaccine.
CDC
CDC
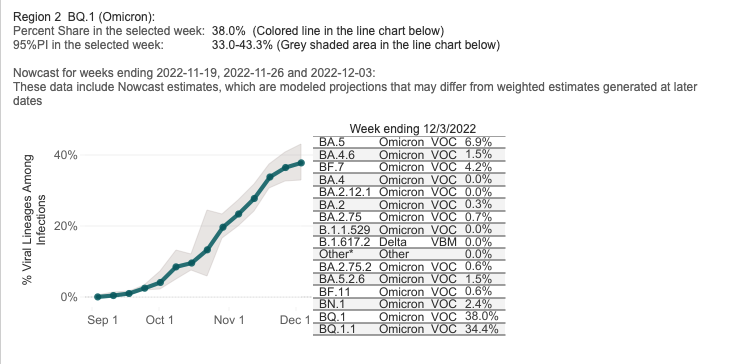
The total percentage of BQ variant infections in the region that includes New York and New Jersey was 64.8% two weeks ago and is now 72.4%. BA.5 accounts for 6.9% of infections, BF.7 accounts for 4.2%, BN.1 accounts for 2.4%, BA.5.2.6 accounts for 1.5%, and BA.2.75 lineages account for 1.3% of infections. Curiously, no XBB isolates are currently being reported in Region 2.
CDC
The total percentage of BQ variant infections in the region that includes California, Nevada, Arizona, and Hawaii was 36.9% two weeks ago and is now 62.6%. BA.5.2.6 isolates now account for 1.6% of cases. The BA.2.75 lineages account for 1.3%. BF.7 accounts for 5.5%, BN.1 accounts for 6.0%, and BA.2 isolates account for 1.9%. Again, CDC is not reporting XBB in Region 9.
Data on the rapid spread of a dangerous variant category, the BQ variants, was withheld by the CDC in their weekly reports until five weeks ago. The data on BQ.1 and BQ.1.1, the last being a variant with five significant spike protein mutations leading to escape from immunity from prior infections or vaccination. Similarly, the XBB variant wasn’t present in the CDC’s variant proportions reporting two weeks ago, but the December 3 iteration adds XBB going back at least three weeks.
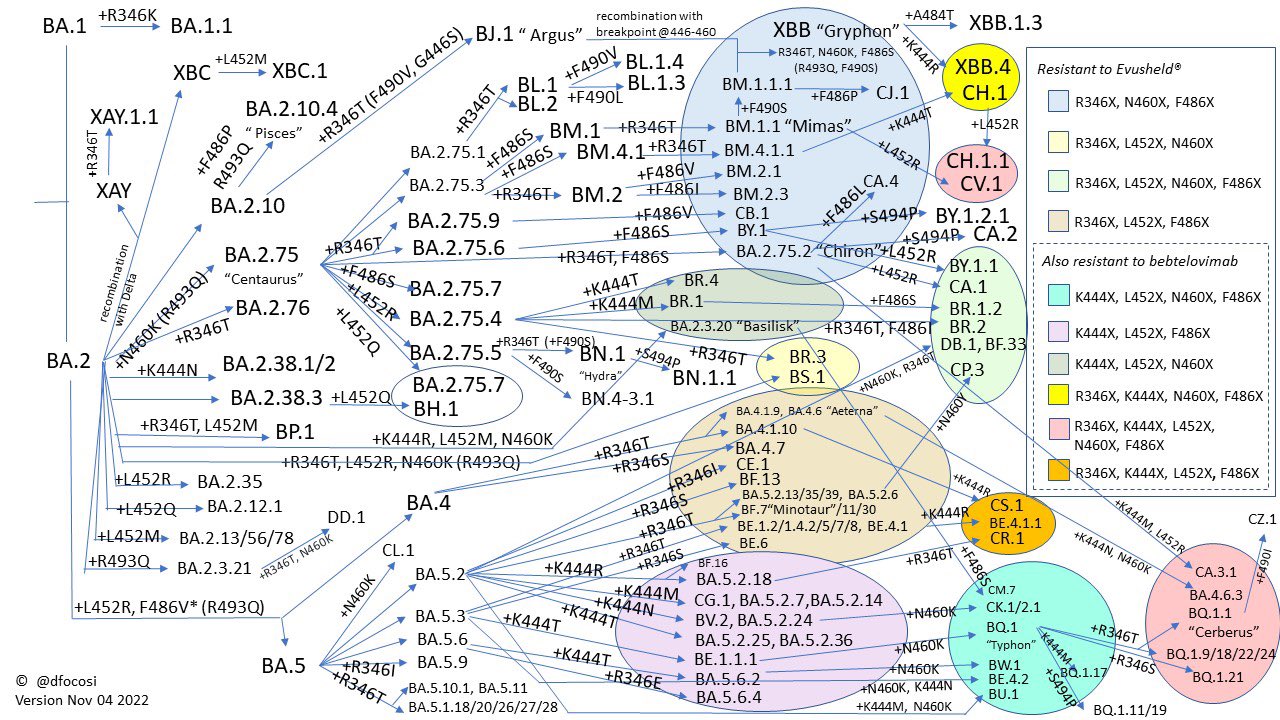
Two virologists collaborated on Twitter to create the figure below, which Professor Johnson titled “Convergent Evolution on Steroids.” It shows the key mutations present in many of the currently-circulating Omicron subvariants and demonstrates that mutation at site 346 is becoming more and more common.
From Daniele Focosi, M.D., Ph.D. @dfocosi on Twitter, November 4, 2022
Past infections with a BA.1, BA.2 or BA.5 variants will not prevent infections with any of the newer variants. Monoclonal antibodies are no longer effective against newer BQ variants and other spike protein mutated variants. The last remaining monoclonal antibody, bebtelovimab, was removed from use by the FDA on 12/2/22. Paxlovid was only 89% effective in the original clinical trials against SARS-CoV-2. If resistance develops this winter to oral Paxlovid, we will have more Paxlovid failures and increased hospitalizations and deaths.
The November 25 UK Health Security Agency Technical Briefing identifies lineages BA.5, BA.5.2.35, BA.5.7, BQ.1, BQ.1.1, XBB, and BN1 (BA.2.75.5.1) as isolates of concern.
Variant
Sublineage of
Mutations
Global Sequences outside UK
UK Sequences
BQ.1
BA.5
L452R, N460K, K444T
33,206 (81 countries)
9,285 (> 40% of all sequenced samples)
BQ.1.1
BA.5
N460K, K444T, R346T
17,621 (70 countries)
4,715
BA.5.2.35
BA.5.2
R346T, 2 synonymous single nucleotide polymorphisms (SNPs) G28423C and C7006T
447
848
BN.1
BA.2.75.5
R346T, F490S
1,127
190
XBB
Recombinant of BJ.1 and BM.1.1.1 (both descended from BA.2), approximate break point between spike mutations G446S and N460K
E: T11A, Spike: V83A, H146Q, Q183E, F486S, F490S. Spike mutations inherited from BJ.1 are G339H, R346T, V445P, G446S and from BM.1.1.1 are N460K, F486V, F490S, and R493Q
4,831 (51 countries)
345
Disappointing Vaccine Uptake, Especially Among Children
Our monoclonal antibody therapies do not work for these isolates, but these emerging BQ variants are descendants of BA.5, so the new BA.5 bivalent vaccine should offer some protection, when combined with an N95 mask. It’s troubling that, despite the availability of this vaccine, few people are getting vaccinated. As of November 30, 2022, the CDC reports that 39,719,443 people in the United States (5 years and up) have received the bivalent vaccine. That’s only 17.4% of people who received the primary series and 12% of the overall population.
Children under the age of 5 have not been approved to receive either Omicron BA.5 mRNA booster. Sadly, in children between 0 and 5 years of age only 1.61 million have received at least one dose of any SARS-CoV-2 mRNA vaccine based on the original Wuhan isolate. In the United States, at least 1,372 children have died of COVID-19, and another 74 have died of multisystem inflammatory syndrome (MIS-C). Worldwide, according to UNICEF, over 16,100 children and young adults aged 0-20 have died of COVID-19.
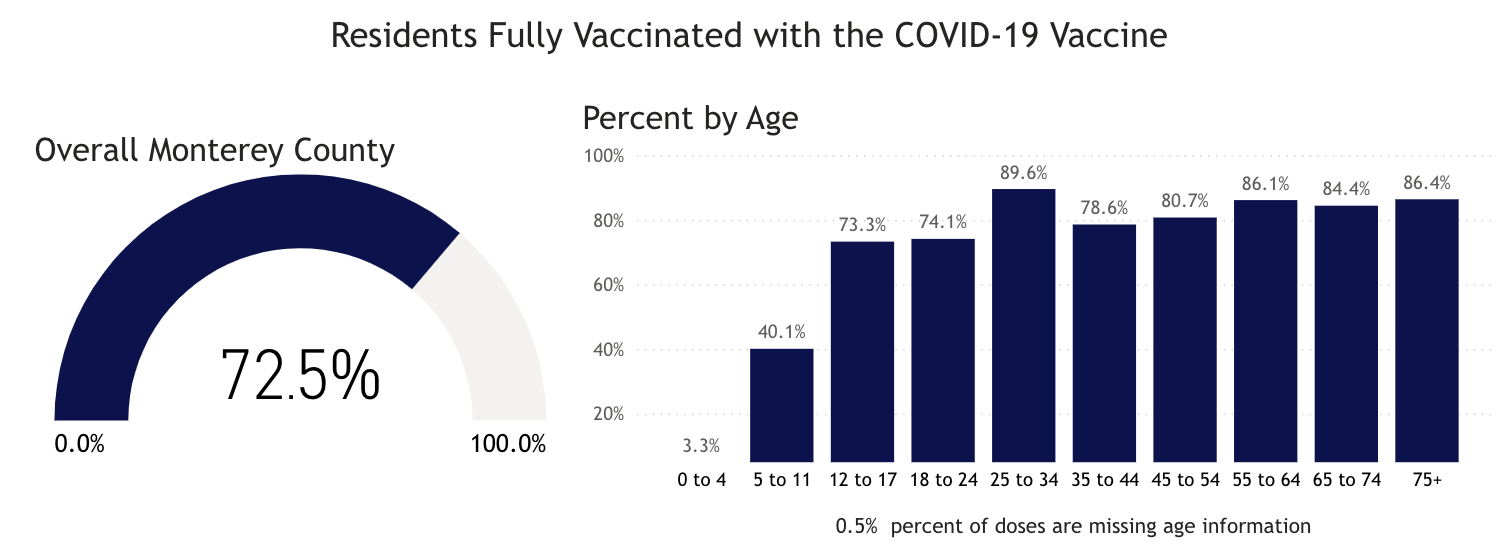
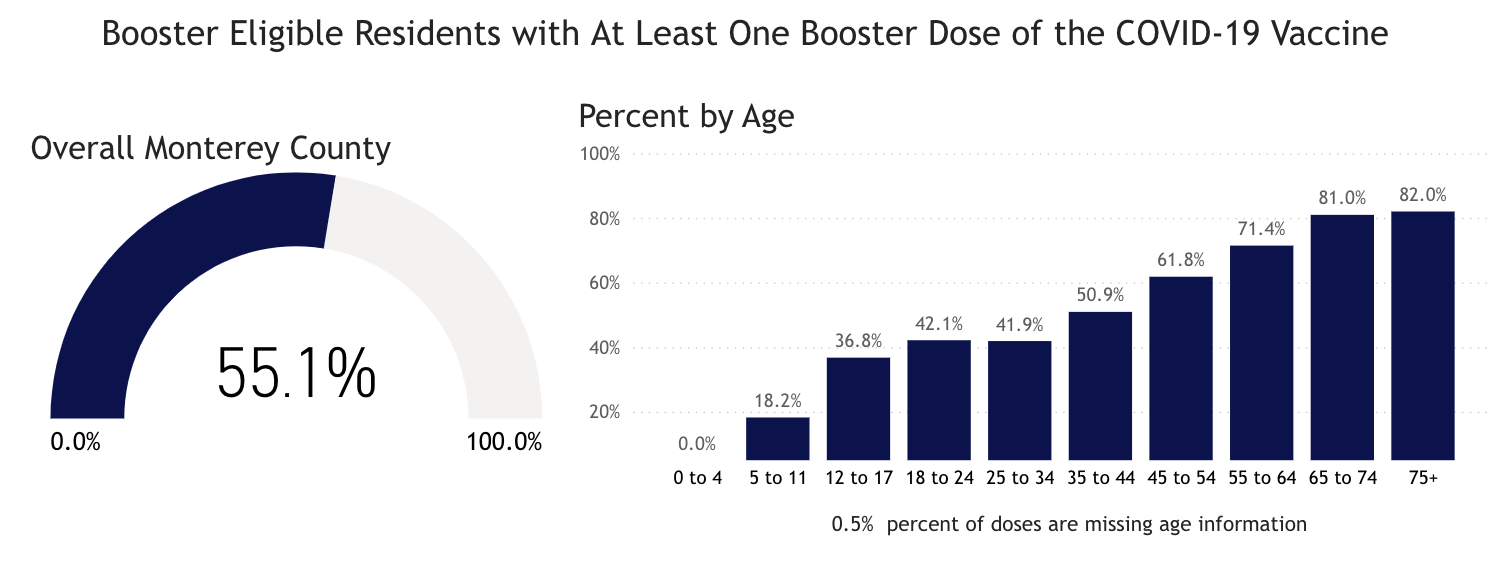
In Monterey County, during the pandemic we have had 96,851 reported SARS-CoV-2 infections, 3,022 hospitalizations and 797 reported deaths as of 12/3/22. The Monterey County Health Department reports that, as of 12/3/22, 3.3% of 0-4 year-olds and 40.1% of 5-11 year-olds have received the first two doses of vaccine, while 73.3% of 12-17 year-olds have received two doses. Only 55.1% of Monterey County residents have received a third dose of the vaccine. The Monterey County Health Department does not publish data on how many residents have received the new BA.5 bivalent booster vaccine. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. All Monterey County residents should get up to date on COVID-19 vaccinations, including the bivalent BA.5 booster, as soon as possible.
Monterey County Health Department
Mask Up to Protect Against Additional Viral Threats This Winter
In a new preprint on respiratory syncytial virus (RSV) in young children, researchers from Case Western University write, “Among RSV-infected children in 2022, 19.2% had prior documented COVID-19 infection, significantly higher than the 9.7% among uninfected children, suggesting that prior COVID-19 could be a risk factor for RSV infection or that there are common risk factors for both viral infections.” Wearing a well-fitting, high-filtration mask not only protects against COVID but also protects against other viruses like RSV, influenza, and measles. The recent surge in respiratory infections among children that has overwhelmed hospitals around the country is most certainly a result of the removal of mask mandates throughout the United States. A new study of COVID infection data in Massachusetts public schools from February to June 2022, after many districts rescinded mask mandates, shows that “the lifting of masking requirements was associated with an additional 44.9 cases per 1000 students and staff,” compared to in schools where mask requirements were upheld. The authors explain that the districts which kept mask requirements in place were ones that tended to have less updated buildings and whose student populations had a greater percentage of low-income families, students with disabilities, English learners, and Black and Latinx students. As such, they conclude, “we believe that universal masking may be especially useful for mitigating effects of structural racism in schools, including potential deepening of educational inequities.” This is something that we’ve been saying since the beginning of the pandemic; removing nonpharmaceutical interventions always disproportionately harms the most vulnerable members of our society.
The state of Ohio has had 54 cases of measles this year, 50 of which were in the Columbus area, and 20 of which have required hospitalization. All of the infected were unvaccinated. Arstechnica reports, “Nine of the cases are in babies under the age of 1 year, who are typically not yet eligible for vaccination. Twenty-six cases are in infants ages 1 to 2 years—who are eligible for their first dose. Ten cases are in toddlers ages 3 to 5—some of whom would have been eligible for their second dose—and there are five cases in children between the ages of 6 and 17.”
As of December 1, the CDC has reported 76 cases of measles in the United States in five (undisclosed) jurisdictions. We’re certain that with no COVID mitigations for holiday travel, the measles will not remain in Ohio.
A Deeper Dive into U.S. COVID Data
On 12/2/22, the United States had 32,724 documented new infections. There were also 149 deaths. Thirty-four states did not report their infections, and 38 states didn’t report their deaths. In the United States on 12/2/22 the number of hospitalized patients (34,646) has increased (+24% compared to the previous 14 days) and was 27,868 on November 18. On 12/2/22 there were 4,005 patients who were seriously or critically ill (a 20% increase); that number was 3,362 two weeks ago. The number of critically ill patients has increased by 643 in the last 14 days, while at least 4,168 new deaths occurred. The number of critically ill patients has increased for the eighth time in thirty-two 14-day periods. Patients are still dying each day (average 298/day).
As of 11/18/22, we have had 1,106,607 deaths and 100,787,799 SARS-CoV-2 infections in the United States. We have had 631,454 new infections in the last 14 days. We are adding an average of 315,727 new infections every seven days. For the pandemic in the United States we are averaging one death for every 91.08 infections or over 10,980 deaths for each one million infections. As of 12/02/22, thirty-nine states have had greater than 500,000 total infections, and 38 states and Puerto Rico have had greater than 5,000 total deaths. Forty-six states have had greater than 2,000 deaths, and 33 states have greater than 3,000 deaths per million population. Eight states have over 4,000 deaths per million population: Mississippi (4,380), Arizona (4,362), Alabama (4,212), West Virginia (4,256), New Mexico (4,150), Tennessee (4,145), Arkansas (4,168) and Michigan (4,014). Eighteen states (Alabama, Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Eight states have had greater than 40,000 deaths: Florida (82,875 deaths), Texas (91,934 deaths), New York (74,288 deaths), Pennsylvania (48,387 deaths), Georgia (41,070 deaths), Ohio (40,558 deaths) , Illinois (40,339 deaths), Michigan (40,085), and California (97,515 deaths, 20th most deaths in the world).
On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. Since 11/20/20 (24 months), there were 839,506 new deaths from SARS-CoV-2. For twenty of those months, vaccines have been available to all adults. During these twenty months, 534,508 people have died of SARS-CoV-2 infections. Clearly, a vaccine-only approach is not working anywhere, especially not in the United States. In addition to getting more people vaccinated, most of the hospitalizations and deaths could have been prevented by proper masking (N95 or better), social distancing, and treatment with oral antiviral agents like Paxlovid. We recommend all of these precautions and treatments to every patient in our clinic, and we have only lost one patient to COVID in 2.5 years.
As of 12/02/22, California was ranked 33rd in the USA in infection percentage at 29.06%. In California, 25.09% of the people were infected in the last 21 months. As of 12/2/22, 28 states have had greater than 30% of their population infected. Fifty states, the District of Columbia and Puerto Rico have greater than 20% of their population infected.
Worldwide, average deaths per day are 1,444 for the last 14 days. The United States accounts for 20.63% (298 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 482,580 the last two weeks. The United States accounts for 9.34% of those infections (or 45,104 infections per day).
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Watching World Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 12/2/22
New Infections on 12/2/22
Total Deaths
New Deaths on 12/2/22
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate
Currently in Lockdown
World
649,308,956(6,756,121 new infections in 14 days).
429,743
6,645,094(20,221 new deaths in last 14 days)
1,029
8.33%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1 (USA)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BF.7BJ.1XBBBQ.1BQ.1.1BS.1BN.1
No
No
USA
100,787,779(ranked #1) 631,454 new infections in the last 14 daysor 45,104/day.
32,724(ranked #5) 34 states and D,C. failed to report infections on 12/2/22.
1,106,607(ranked #1) 4,168 new deaths reported in the last 14 days or 388/day.
149 38 states and D.C. failed to report deaths on 12/2/22.
30.10%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BQ.1BQ.1.1BN.1
No
No
Brazil
35,375,733(ranked #5) 336,119 new infections in the last 14 days.
399251 (ranked#4)
690,129(ranked #2; 1,171 new deaths in 14 days)
131
16.42%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
India
44,674,195(ranked #2); 4,668 new infections in 2 weeks.
211
530,627(ranked #3) 94 new deaths in 2 weeks.
3
3.17%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India)
No
No
United Kingdom
24,024,746(ranked #6) 47,109 new infections in 2 weeks.
–
197253 (ranked #7) 1,102 new deaths in 2 weeks
–
35.07%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)
No
No
California, USA
11,483,568(ranked #14 in the world; 78,380 new infections in the last 14 days).
4,819
97,515 (ranked #20 in world) 176 new deaths in the last 14 days
14
29.06%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BQ.1BQ.1.1BN.1
No
No
Mexico
7,132,792(ranked #19) 13,859 new infections in 14 days).
–
330,525(ranked #5)81 new deaths in 14 days)
–
5.42%
No
No
South Africa
4,042,221(ranked #37; 5,299 new infections in 14 days).
312
102,464 (ranked #18) 93 new deaths in 14 days)
–
6.65%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
Canada
4,408,276(ranked #34) 31,206 new infections in 14 days).
–
47,781(ranked #25 ) 663 new deaths in the last 14 days
–
11.48%
No
No
Poland
6,353,850 (ranked #21;5,470 new infections in 14 days).
542
118,332 (ranked #15)65 new deaths in the last 14 days
4
16.83%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3
No
No
Russia
21,597,613 (ranked #10), 72,046 new infections in 14 days).
6,785 (ranked #11)
392,060(ranked #4)727 new deaths in 14 days
58
14.81%
No
No
Peru
4,266,251(ranked #36, 107,119 new infections in 14 days).
13,868 (ranked#9)
217,428(ranked #6) 199 new deaths in the last 14 days
14
12.66%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Iran
7,559,737(ranked #18; 526 new infections in last 14 days)
31
144,634(ranked #12) 14 new deaths in the last 14 days
1
8.78%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Spain
13,612,052(ranked #12; 38,331 new infections in 14 days).
2,758
116,081 (ranked #16)440 new deaths in 14 days
30
29.13%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)
No
No
France
37,916,052 (ranked #3; 628,505 new infections in the last 14 days).
69,253 (ranked #2)
159,026 (ranked #10)863 new deaths in 14 days.
76
57.81% a 1.52% increase in 14 days.
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinantBQ.1.1
No
No
Germany
36,530,020(ranked #4; 324,615 new infections in 14 days.)
30,420 (ranked #6)
158,108 (ranked #11)1,486 new deaths in 14 days
166
43.54% 0.38% increase in 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinantBQ.1.1
No
No
South Korea
27,155,813 (ranked #6 693,494 new infections in 14 days).
57,079(ranked #3)
30,568 (ranked #35) 643 new deaths in 14 days
62
52.90%1.35%increase in 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Vietnam
11,516,489 (ranked #13; 5,570new infections in 14 days).
581
43,176(ranked #26)
1
11.63%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Netherlands
8,543,838 (ranked #16; 9,694 new infections in 14 days).
959
22,916 (ranked #41)
3
49.64%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Denmark
3,148,210 (ranked #40) 4,949 new infections in 14 days.
610
7,537(ranked #78 67 new deaths in the last 14 days)
5
53.95%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Taiwan
8,329,000(ranked #17)198,781 new infections in 14 days
15,643 (ranked #7)
14,387 (ranked #58 539 new deaths in the last 14 days)
53
34.86% 0.83% of population has been infected in the last 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Japan
24,911,367(ranked #7)1,307,161 new infections in the last 14 days
118,201(ranked #1)
49,826(ranked #23) 1,768 new deaths in the last 14 days
182
19.83% 1.04% of the population infected in the last 14 days.
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)BA.2*BA.5*
No
No
Argentina
9,727,247 (ranked #15)5,529 new infections in the last 14 days.
–
130,025(ranked #14)
–
21.14%
No
No
Italy
24,327,664 (ranked #8)96,126 new infections in the last 14 days.
–
181,733(ranked #8) 1,152 new deaths in the last 14 days
–
40.36% 0.49% of population infected in last 14 days.
No
No
Chile
4,925,051(ranked #28) 59,393 new infections in14 days..
5,041 (ranked#13)
62,484(ranked #22) 354 new deaths in the last 14 days.
26
25.28% 0.31% of population infected in the last 14 days.
No
No
Colombia
6,318,021(ranked #22) 5,364 new infections in the last 14 days.
3,252
141,811(ranked #13)
16
12.26%
No
No
Australia
10,725,239(ranked #14) 172,561 new infections in 14 days.
14,741 (ranked #8)
16,187(ranked #55) 220 new deaths in 14 days.
16
41.14% 0.66% of population infected in last 14 days.
No
No
Turkey
17,005,537(ranked #11)28,808 new infections in 14 days.
–
101,400(ranked #19) 73 new deaths in 14 days..
–
19.87%
No
No
Indonesia
6,669,821 (ranked #20) 73,009 new infections in last 14 days.
4,977 (ranked #14)
159,884 (ranked #9) 561 new deaths in the last 14 days.
54
23.89%
No
No
Malaysia
4,994,543 (ranked #27) 31,327 new infections in the last 14 days.
2,375
36,695 (ranked #29) 107 new deaths in the last 14 days.
11
15.05%
No
No
Hong Kong
2,128,382(ranked#46) 107,497 new infections in the last 14 days.
10,137 (ranked #10)
10,762 (ranked#64)185 new deaths in the last 14 days.
15
27.98% 1.41% of population infected in the last 14 days.
No
No
China
323,686 (ranked #103)44,255 new infections in 14 days
Single-cell multiomics revealed the dynamics of antigen presentation, immune response and T cell activation in the COVID-19 positive and recovered individuals https://doi.org/10.3389/fimmu.2022.1034159
Novel treatment combining antiviral and neutralizing antibody-based therapies with monitoring of spike-specific antibody and viral load for immunocompromised patients with persistent COVID-19 infection (Experimental Hematology & Oncology) https://ehoonline.biomedcentral.com/articles/10.1186/s40164-022-00307-9
Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies (Acta Pharmacologica Sinica) https://doi.org/10.1038/s41401-022-00998-0
Brain 18F-FDG PET imaging in outpatients with post-COVID-19 conditions: findings and associations with clinical characteristics (European Journal of Nuclear Medicine and Molecular Imaging) https://doi.org/10.1007/s00259-022-06013-2
Successful treatment of prolonged, severe COVID-19 lower respiratory tract disease in a B-cell ALL patient with an extended course of remdesivir and nirmatrelvir/ritonavir (Clinical Infectious Diseases) https://doi.org/10.1093/cid/ciac868
Effectiveness of Monovalent mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States — IVY Network, 18 States, December 26, 2021–August 31, 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7142a3.htm
“Three-dose monovalent mRNA VE estimates against COVID-19–associated hospitalization decreased with time since vaccination. Three-dose VE during the BA.1/BA.2 and BA.4/BA.5 periods was 79% and 60%, respectively, during the initial 120 days after the third dose and decreased to 41% and 29%, respectively, after 120 days from vaccination.”
Saliva antibody-fingerprint of reactivated latent viruses after mild/asymptomatic COVID-19 is unique in patients with myalgic-encephalomyelitis/chronic fatigue syndrome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.949787
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
SARS-CoV-2 infections per day in the United States have increased for the first time in 14 weeks. There is still widespread underreporting by states, a failure to capture positive home tests, and a decreased PCR screening program in most states. Deaths per day in the United States have increased by 34 deaths per day. Many states are not reporting deaths or infections in a timely manner. The number of infections per day has increased by 1,683. The CDC estimates that BA.5 accounted for 39.2% (a 23% drop from 10/21/22), BQ.1 accounted for 16.5% (a 7.1% increase since 10/21/22), BQ.1.1 accounted for 18.8% (a 11.6% increase since 10/21/22), BA.4.6 accounted for 9.5%, BF.7 accounted for 9%, BA.2.75.2 accounted for 1.3%, and BA.4 accounted for 0.2%. In the week ending November 5, 2022 BQ isolates accounted for 35.3% of infections. BQ.1.1 has five spike mutations that are different from BA.5. Four of these mutations allow escape from immunity from monoclonal antibodies, any prior infection (including BA.5), or any vaccine to include a BA.5 vaccine.
CDCCDC
The total percentage of BQ variant infections in the region that includes New York and New Jersey was 28.4% two weeks ago and is now 52.3%. BA.5.2.6 isolates now account for 3.1% of cases. The BA.2.75 lineages account for 4.2%.
CDC
The total percentage of BQ variant infections in the region that includes Pennsylvania, Delaware, Maryland, West Virginia, and Virginia was 17.8% two weeks ago and is now 36.6%. BA.5.2.6 isolates now account for 3.4% of cases. The BA.2.75 lineages account for 3% of cases.
CDC
The total percentage of BQ variant infections in the region that includes California, Nevada, Arizona, and Hawaii was 13.6% two weeks ago and is now 36.9%. BA.5.2.6 isolates now account for 2.4% of cases. The BA.2.75 lineages account for 4.2%.
Data on the rapid spread of a dangerous variant category, the BQ variants, was withheld by the CDC in their weekly reports until three weeks ago. The data on BQ.1 and BQ.1.1, the last being a variant with five significant spike protein mutations leading to escape from immunity from prior infections or vaccination. In addition, our monoclonal antibody therapies do not work for these isolates. Infections and hospitalizations in New York are rapidly increasing, secondary to BQ variants. BQ variants have been found in all 10 regions in the United States. Since New York has been a harbinger of things to come throughout the pandemic, we expect the pattern of increased infections, hospitalizations and deaths to continue in many states. These emerging BQ variants are descendants of BA.5. It’s troubling that, despite the availability of a BA.5 bivalent SARS-CoV-2 vaccine, few people are getting vaccinated. As of November 2, 2022, the CDC reports that only 26,378,963 people have received the bivalent vaccine. The Pfizer Omicron BA.5 mRNA booster was administered to 16,748,737 people and the Moderna Omicron BA.5 mRNA booster was administered to 9,630,226 people. In total, 26.3 million people (5 years and up) have received the bivalent vaccine. That’s only 11.6% of people who received the primary series and 7.9% of the overall population.
Children under the age of 5 have not been approved to receive either Omicron BA.5 mRNA boosters. Sadly, in children between 0 and 5 years of age only 1.47 million have received at least one dose of any SARS-CoV-2 mRNA vaccine. In the United States, at least 1,332 children have died of COVID-19, and another 74 have died of multisystem inflammatory syndrome (MIS-C). Worldwide, according to UNICEF, over 16,100 children and young adults aged 0-20 have died of COVID-19.
The October 28 UK Health Security Agency Technical Briefing identifies lineages BQ.1, BQ.1.1, XBB, and BF.7 as isolates of concern. Although BA.5 remains the dominant lineage in the UK, the authors explain, “In the most recent week, logistic growth of variants with 1, 2 or 3 convergent and antigenically significant RBD mutations was respectively 23%, 47%, and 66% per week. The category with 3 RBD mutations consisted largely of BQ.1.1 (59%) with the remainder consisting primarily of a mixture of BA.2.75 sub-lineages (29%).”
Variant
Sublineage of
Spike Mutations
Global Sequences
UK Sequences
BF.7
BA.5.2.1
R346T
11,922
2,644
BQ.1
BA.5
L452RN460KK444T
2,490
3,207
BQ.1.1
BA.5
N460KK444TR346T
2,304(35 countries)
1,272
BS.1
BA.2.3.2
R346TL452RN460KG476S
79
2
Data from UK Health Security Agency
In Monterey County, as of 11/5/22, 2.6% of 0-4 year-olds and 40.1% of 5-11 year-olds have received the first two doses of vaccine, while 73.4% of 12-17 year-olds have received two doses. Only 54.5% of Monterey County residents have received a third dose of the vaccine. The Monterey County Health Department does not publish data on how many residents have received the new BA.5 bivalent booster vaccine. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. All Monterey County residents should get up to date on COVID-19 vaccinations, including the bivalent BA.5 booster, as soon as possible.
Monterey County Health Department
On 11/04/22, the United States had 21,312 documented new infections. There were also 148 deaths. Thirty-five states did not report their infections, and 37 states didn’t report their deaths. In the United States the number of hospitalized patients has increased slightly (+2% compared to the previous 14 days) in many areas and was 27,395 on November 5. On 11/05/22 there were 3,146 patients who were seriously or critically ill; that number was 2,707 two weeks ago. The number of critically ill patients has increased by 439 in the last 14 days, while at least 5,432 new deaths occurred. The number of critically ill patients has decreased for the sixth time in thirty 14-day periods. Patients are still dying each day (average 388/day). Two new Omicron variants BQ.1 and BQ.1.1 are causing increased numbers of infections and hospitalizations in New York. BA.4, BA.4.6, BA.5, and BF.7 variants are still causing infections. In Singapore a different Omicron BA.2 variant, XBB, has caused rapidly increasing infections and now has been named a designated variant along with BQ.1 in the October 28 UK Health Security Agency Technical Briefing. Past infections with a BA.1, BA.2 or BA.5 variants will not prevent infections with any of the newer variants.
As of 11/04/22, we have had 1,098,038 deaths and 99,602,478 SARS-CoV-2 infections in the United States. We have had 546,941 new infections in the last 14 days. We are adding an average of 273,348 new infections every seven days. For the pandemic in the United States we are averaging one death for every 90.71 infections or over 11,024 deaths for each one million infections. As of 11/04/22, thirty-eight states have had greater than 500,000 total infections, and 38 states have had greater than 5,000 total deaths. Forty-six states have had greater than 2,000 deaths, and 43 states have greater than 2,000 deaths per million population. Seven states have over 4,000 deaths per million population: Mississippi (4,365), Arizona (4,338), Alabama (4,193), West Virginia (4,202), New Mexico (4,132), Tennessee (4,118), and Arkansas (4,148). . Eighteen states (Alabama, Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Eight states have had greater than 40,000 deaths: Florida (82,357 deaths), Texas (91,737 deaths), New York (73,549 deaths), Pennsylvania (47,840 deaths), Georgia (40,696 deaths), Ohio (40,249 deaths) , Illinois (40,058 deaths), and California (96,984 deaths, 20th most deaths in the world).
On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. Since 11/20/20 (23 months), there were 830,937 new deaths from SARS-CoV-2. For nineteen of those months, vaccines have been available to all adults. During these nineteen months, 525,939 people have died of SARS-CoV-2 infections. Clearly, a vaccine-only approach is not working anywhere, especially not in the United States. In addition to getting more people vaccinated, most of the hospitalizations and deaths could have been prevented by proper masking (N95 or better), social distancing, and treatment with oral antiviral agents like Paxlovid. We recommend all of these precautions and treatments to every patient in our clinic, and we have only lost one patient to COVID in 2.5 years.
As of 11/04/22, California was ranked 33rd in the USA in infection percentage at 28.73%. In California, 24.76% of the people were infected in the last 20 months. As of 11/06/22, 24 states have had greater than 30% of their population infected. Fifty states have greater than 20% of their population infected.
Worldwide, average deaths per day are 1,637 for the last 14 days, which is a 68 deaths-per-day increase over the previous 14 days. The United States accounts for 23.70% (388 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 346,369. The United States accounts for 11.28% of those infections (or 39,067 infections per day).
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Merck has developed the oral drug Molnupiravir, which induces RNA mutagenesis by viral RNA-dependent RNA polymerase of SARS-CoV-2 and other viruses. According to Kabinger et al, “Viral RNA-dependent RNA polymerase uses the active form of Molnupiravir, β-D-N4-hydroxycytidine triphosphate, as a substrate instead of cytidine triphosphate or uridine triphosphate. When the RNA-dependent RNA polymerase uses the resulting RNA as a template, β-D-N4-hydroxycytidine triphosphate directs incorporation of either guanine or adenine, leading to mutated (viral) RNA products. Analysis of RNA-dependent RNA polymerase–RNA complexes that contain mutagenesis products has demonstrated that β-D-N4-hydroxycytidine (the active form ofMolnupiravir) can form stable base pairs with either guanine or adenine in RNA-dependent RNA polymerase explaining how the polymerase escapes proofreading and synthesizes mutated RNA” (quotation modified for clarity). The results of the phase 3 trial of Molnupiravir were published in the NEJM article “Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients” by Angélica Jayk Bernal, M.D. et al. (December 16, 2021 DOI: 10.1056/NEJMoa2116044). In this phase 3 study in the Molnupiravir group, 28 patients were hospitalized and one death occurred. In the placebo group, 53 patients were hospitalized and 9 died. Overall, 47% of hospitalizations and deaths were prevented by Molnupiravir. If you do a post hoc analysis and just look at deaths,Molnupiravir would prevent 89% of deaths. An Emergency Use Authorization by the FDA for Molnupiravir was approved on 12/24/21.The dose of Molnupiravir approved is four 200 mg capsules orally twice a day for five days. Diarrhea is reportedly a side effect in two percent of patients. I treated my first patient with Molnupiravir on 1/28/22. Currently more Molnupiravir is available weekly in the United States than PAXLOVID™ (see chart below; data from PHE.gov). Locally Molnupiravir is still available at CVS in Monterey (Fremont Blvd.; phone number: 831-375-5135) and CVS in Salinas (East Alisal Street; phone number 831-424-0026).
28, p740–746 (2021)with four 200 mg capsules orally twice a day for five dayfour 200 mg capsules orally twice a day for five daysIntravenous Drug Treatment for non-hospitalized SARS-CoV-2 Infected Patient
FDA-Approved Intravenous Monoclonal Antibody Treatment for Non-Hospitalized SARS-CoV-2 Patients
Bebtelovimab is a monoclonal antibody treatment for mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death, and for whom alternative COVID-19 treatment options approved or authorized by FDA are not accessible or clinically appropriate. The authorized dose of bebtelovimab is 175 mg, given as an intravenous injection over at least 30 seconds. The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for this drug on 2/11/22. Bebtelovimab is a human antibody that demonstrates neutralization against the Omicron variants and is available in every state and many hospitals and some clinics. If you are planning on using a monoclonal antibody to treat a SARS-CoV-2 infection, currently only bebtelovimab has activity against all Omicron variants, including BA.4.6. Researchers at Columbia University recently reported that “The loss of activity of tixagevimab and cilgavimab [components of Evusheld] against BA.4.6 leaves us with bebtelovimab as the only therapeutic mAb that has retained potent activity against all circulating forms of SARS-CoV-2.” For this reason, we no longer recommend Evusheld for immunocompromised patients with Omicron infections.
An examination of the three variants that Wang et al identified as capable of immune escape in patients who receive the two monoclonal antibodies that are contained in Evusheld reveals that all three variants have a mutation in the spike protein at position 346. The changes substitute an uncharged amino acid— threonine (T), serine (S), or isoleucine (I)—for a positively-charged amino acid, arginine. This just goes to show that a single point mutation in the spike protein can render a monoclonal antibody treatment ineffective. Policy makers should keep in mind that the only way to prevent new drug-resistant variants like BA.4.6 from emerging is to prevent transmission of SARS-CoV-2 in the first place, using non-pharmaceutical interventions. The lack of use of N95 masks, with impending winter and influenza outbreaks, on top of COVID-19, is not wise public health and infectious disease policy. If we don’t make effective use of the non-pharmaceutical interventions available to us (masks, ventilation, social distancing), then the pharmaceutical interventions we have will all eventually be useless.
Two virologists collaborated on Twitter to create the figure below, which Professor Johnson titled “Convergent Evolution on Steroids.” It shows the key mutations present in many of the currently-circulating Omicron subvariants and demonstrates that mutation at site 346 is becoming more and more common. This means that even if prevalence of BA.4.6 wanes, we are still likely to have drug resistance issues with other newer variants.
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
Location
Total Infections as of 11/04/22
New Infections on 11/04/22
Total Deaths
New Deaths on 11/04/22
% of Pop.Infected
SARS-CoV-2 Isolates Currently Known in Location
National/ State Mask Mandate
Currently in Lockdown
World
637,281,842(4,849,164 new infections in 14 days).
273,333
6,604,448(22,918 new deaths in last 14 days)
1,091
8.17%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1 (USA)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)BF.7BJ.1XBBBQ.1BQ.1.1BS.1
No
No
USA
99,602,478(ranked #1) 546,941 new infections in the last 14 daysor 39,067/day.
19,652(ranked #6) 35 states and D,C. failed to report infections on 11/04/22.
1,098,038(ranked #1) 5,432 new deaths reported in the last 14 days or 388/day.
148 37 states and D.C. failed to report deaths on 11/04/22.
29.74%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BA.4.6 (USA 7/22)
No
No
Brazil
34,890,243(ranked #5) 62,069 new infections in the last 14 days.
2,738
688,384(ranked #2; 803 new deaths in 14 days)
68
16.20%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
India
44,659,447(ranked #2); 18,699 new infections in 2 weeks.
1,082
530,486(ranked #3) 1,529 new deaths in 2 weeks.
7
3.17%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India)
No
No
United Kingdom
23,930,041(ranked #7) 74,519 new infections in 2 weeks.
–
194,704 (ranked #7) 2,022 new deaths in 2 weeks
–
34.93%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)
No
No
California, USA
11,353,896(ranked #13 in the world; 21,351 new infections in the last 14 days).
1,434
96,984 (ranked #20 in world) 303 new deaths in the last 14 days
7
28.73%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)
No
No
Mexico
7,113,132(ranked #19) 7,114 new infections in 14 days).
628
330,415(ranked #5)94 new deaths in 14 days)
5
5.40%
No
No
South Africa
4,029,737(ranked #37; 4,362 new infections in 14 days).
241
102,363 (ranked #18) 106 new deaths in 14 days)
52
6.63%
B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)
No
No
Canada
4,336,860(ranked #33) 22,142 new infections in 14 days).
–
46,389(ranked #25 ) 364 new deaths in the last 14 days
–
11.29%
No
No
Poland
6,333,591 (ranked #21;9,506 new infections in 14 days).
693
118,157 (ranked #15)142 new deaths in the last 14 days
14
16.80%
B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3
No
No
Russia
21,453667(ranked #10), 98,753 new infections in 14 days).
6,149 (ranked #9)
390,459(ranked #4)1,100 new deaths in 14 days
71
14.71%
No
No
Peru
4,159,132(ranked #36, 7,113new infections in 14 days).
598
216,972(ranked #6) 95new deaths in the last 14 days
5
12.34%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Iran
7,558,002(ranked #17; 2,308 new infections in last 14 days)
40
144,587(ranked #12) 47 new deaths in the last 14 days
4
8.78%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)
No
No
Spain
13,529,643(ranked #12; 41,628 new infections in 14 days).
2,551
115,239 (ranked #16)381 new deaths in 14 days
23
28.95%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)
No
No
France
36,920,064 (ranked #3; 395,459 new infections in the last 14 days).
29,438 (ranked #4)
157,277 (ranked #10)940 new deaths in 14 days.
78
56.29% a 0.60% increase in 14 days.
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant
No
No
Germany
35,823,771(ranked #4; 651,078 new infections in 14 days.)
38,859 (ranked #2)
154,535 (ranked #11)2,053 new deaths in 14 days
207
42.70% 0.77% increase in 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
South Korea
25,760,701 (ranked #6 516,446 new infections in 14 days).
43,424(ranked #1)
29,315 (ranked #36) 363 new deaths in 14 days
35
49.18%1.00%increase in 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Vietnam
11,505,249 (ranked #13; 8,895 new infections in 14 days).
339
43,165(ranked #26)
–
11.62%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Netherlands
8,521,729 (ranked #16; 27,024 new infections in 14 days).
1,225
22,845 (ranked #41)
3
49.51%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Denmark
3,138,750 (ranked #40) 7,601 new infections in 14 days.
355
7,387 (ranked #78 139 new deaths in the last 14 days)
12
53.79%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant
No
No
Taiwan
7,837,658(ranked #17)458,453 new infections in 14 days
27,594 (ranked #5)
13,084 (ranked #59 878 new deaths in the last 14 days)
74
32.80% 1.91% of population has been infected in the last 14 days
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)
No
No
Japan
22,534,377(ranked #9)608,146 new infections in the last 14 days
34,064(ranked #5)
46,898(ranked #24) 757 new deaths in the last 14 days
59
17.94%
B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)BA.2*BA.5*
No
No
Argentina
9,718,875 (ranked #15)
–
129,991(ranked #14)
–
21.12%
No
No
Italy
23,642,011 (ranked #8)
–
179,436(ranked #8)
39,23%
No
No
Chile
4,777,208(ranked #28)
7,570
61,737(ranked #22)
12
24.81%
No
No
Colombia
6,310,332(ranked #14)
–
141,850(ranked #13)
–
12.25%
No
No
Australia
9,718,875(ranked #14)
15,618 (ranked #7)
15,776(ranked #55)
59
39.95%
No
No
Turkey
16,919,638(ranked #11)
–
101,203(ranked #19)
–
19.77%
No
No
Indonesia
6,512,913 (ranked #20)
5,303 (ranked #11)
158,768 (ranked #9)
31
23,23%
No
No
Malaysia
4,918,917 (ranked #29)
4,360 (ranked #13)
36,481 (ranked #29)
1
14.75%
No
No
What Our Team Is Reading This Week
Successful treatment of prolonged, severe COVID-19 lower respiratory tract disease in a B-cell ALL patient with an extended course of remdesivir and nirmatrelvir/ritonavir (Clinical Infectious Diseases) https://doi.org/10.1093/cid/ciac868
Effectiveness of Monovalent mRNA Vaccines Against COVID-19–Associated Hospitalization Among Immunocompetent Adults During BA.1/BA.2 and BA.4/BA.5 Predominant Periods of SARS-CoV-2 Omicron Variant in the United States — IVY Network, 18 States, December 26, 2021–August 31, 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7142a3.htm
“Three-dose monovalent mRNA VE estimates against COVID-19–associated hospitalization decreased with time since vaccination. Three-dose VE during the BA.1/BA.2 and BA.4/BA.5 periods was 79% and 60%, respectively, during the initial 120 days after the third dose and decreased to 41% and 29%, respectively, after 120 days from vaccination.”
Saliva antibody-fingerprint of reactivated latent viruses after mild/asymptomatic COVID-19 is unique in patients with myalgic-encephalomyelitis/chronic fatigue syndrome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.949787
Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: an observational study (The Lancet) https://doi.org/10.1016/S0140-6736(22)01586-0
Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients (Ear, Nose, and Throat Journal) https://doi.org/10.1177/01455613221123737
Note: This is a frightening paper and if the conclusions are accurate humans in general are in trouble. From other papers the facts that HERV-M and EBV are activated by SARS-CoV-2 infection does not bode well for humans moving forward.
SARS-CoV-2 Spike protein promotes vWF secretion and thrombosis via endothelial cytoskeleton-associated protein 4 (CKAP4) (Signal Transduction and Targeted Therapy) https://www.nature.com/articles/s41392-022-01183-9
VACCINE INFORMATION FACT SHEET FOR RECIPIENTS AND CAREGIVERS ABOUT COMIRNATY (COVID-19 VACCINE, mRNA), THE PFIZER-BIONTECH COVID-19 VACCINE, AND THE PFIZER-BIONTECH COVID-19 VACCINE BIVALENT (ORIGINAL AND OMICRON BA.4/BA.5) TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19) FOR USE IN INDIVIDUALS 12 YEARS OF AGE AND OLDER https://labeling.pfizer.com/ShowLabeling.aspx?id=14472
SARS-CoV-2 variants of concern: spike protein mutational analysis and epitope for broad neutralization (Nature Communications) https://doi.org/10.1038/s41467-022-32262-8
Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients (The Lancet Psychiatry) https://doi.org/10.1016/S2215-0366(22)00260-7
An Antibody from Single Human VH-rearranging Mouse Neutralizes All SARS-CoV-2 Variants Through BA.5 by Inhibiting Membrane Fusion (Science Immunology) https://doi.org/10.1126/sciimmunol.add5446
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic (Preprint) https://doi.org/10.1101/2022.08.03.22278363
SARS-CoV-2 Brain Regional Detection, Histopathology, Gene Expression, and Immunomodulatory Changes in Decedents with COVID-19 (Journal of Neuropathology and Experimental Neurology) https://doi.org/10.1093/jnen/nlac056
Notes from the Field: Increase in Pediatric Intracranial Infections During the COVID-19 Pandemic — Eight Pediatric Hospitals, United States, March 2020–March 2022 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7131a4



















You must be logged in to post a comment.