
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.

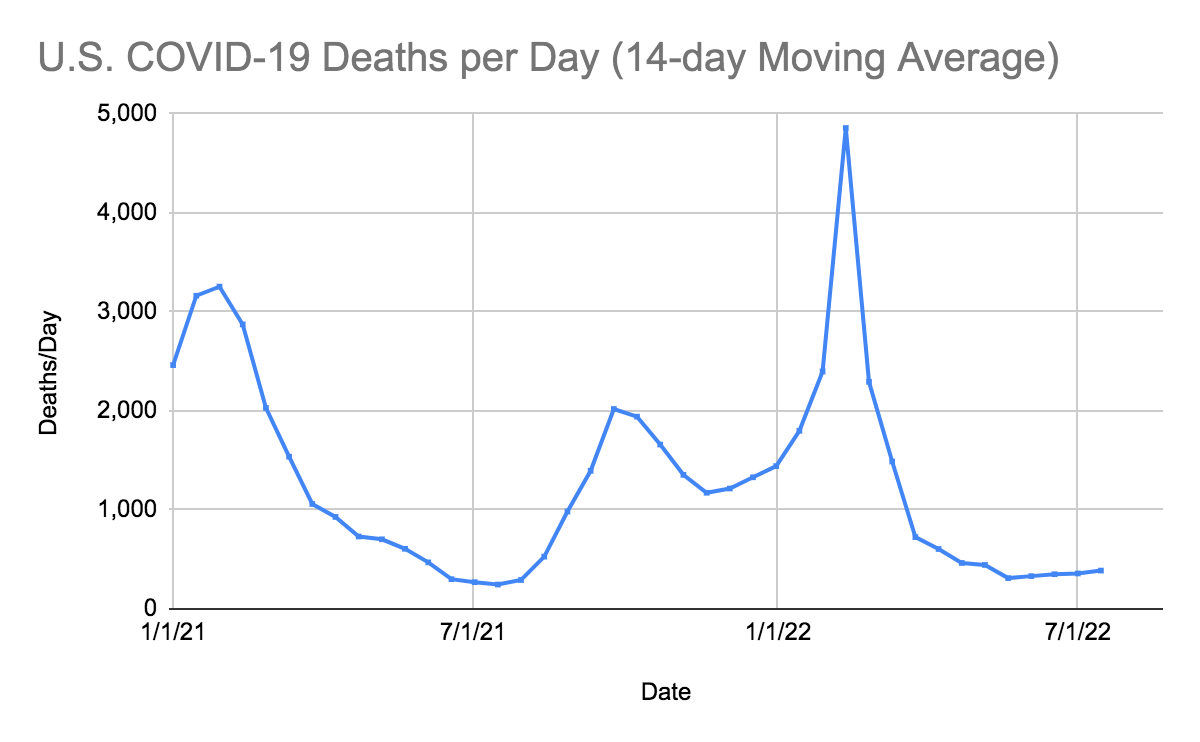
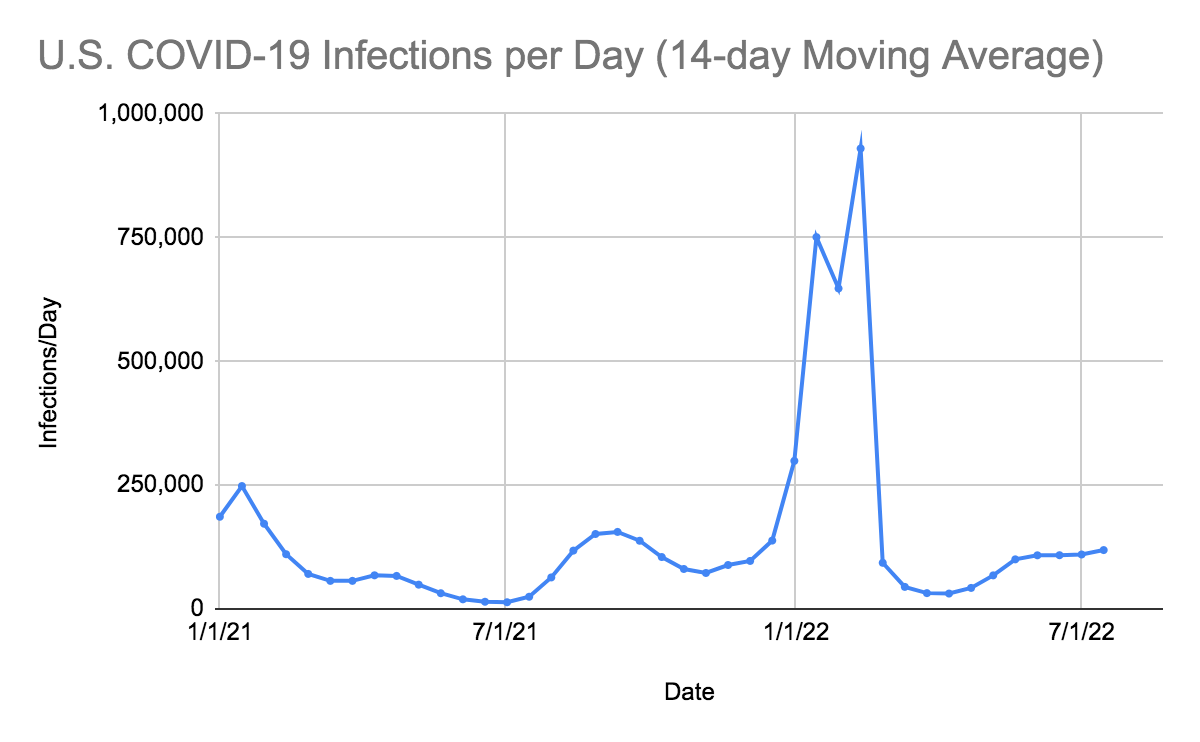
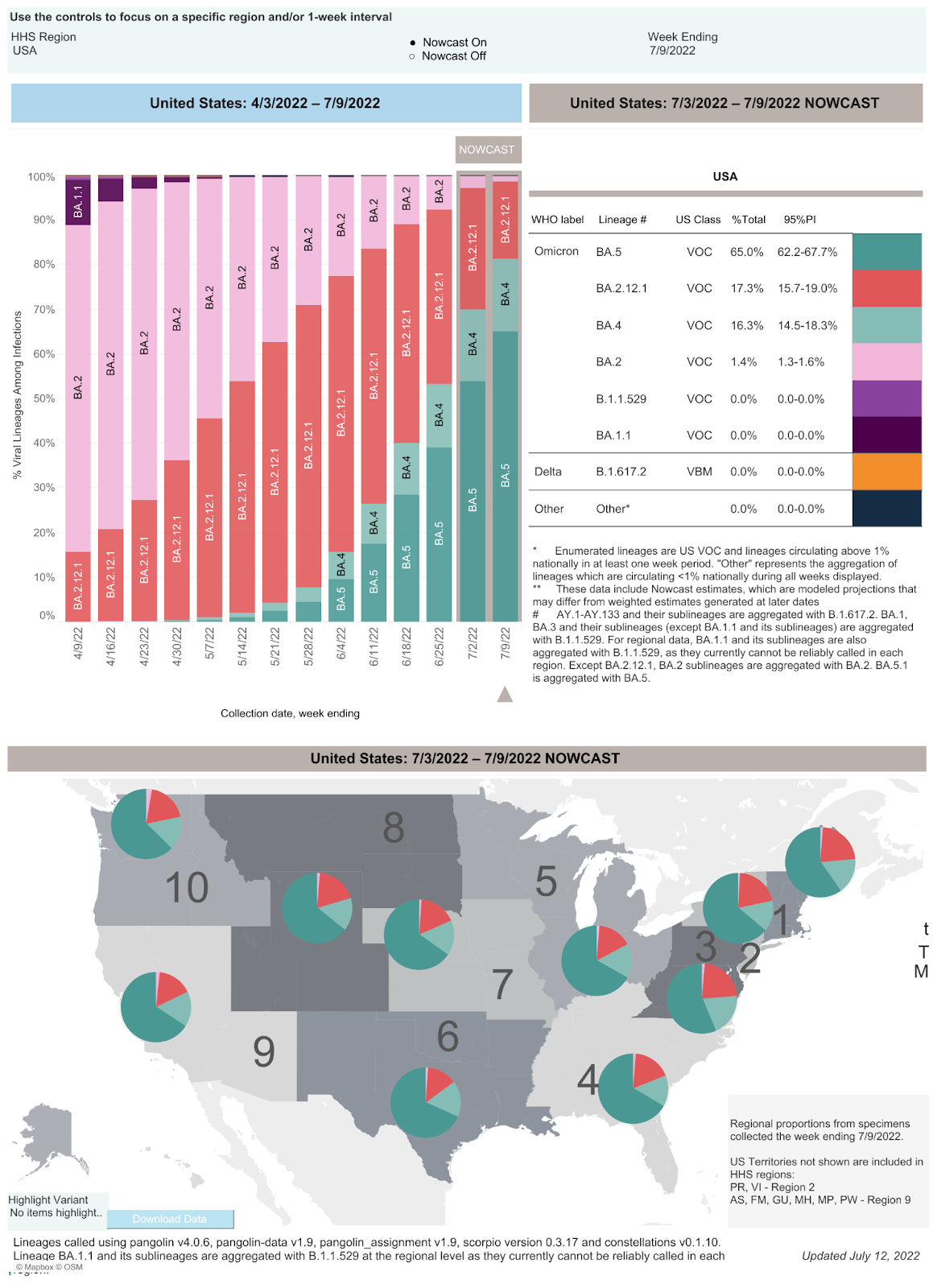
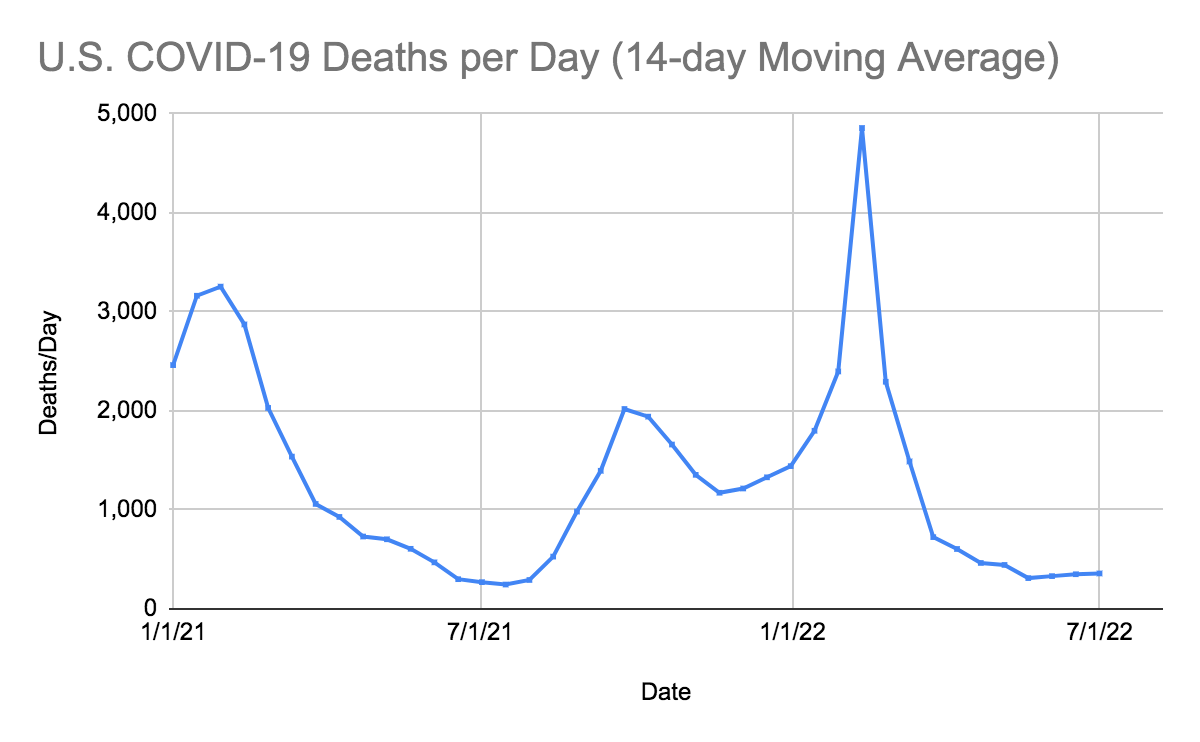
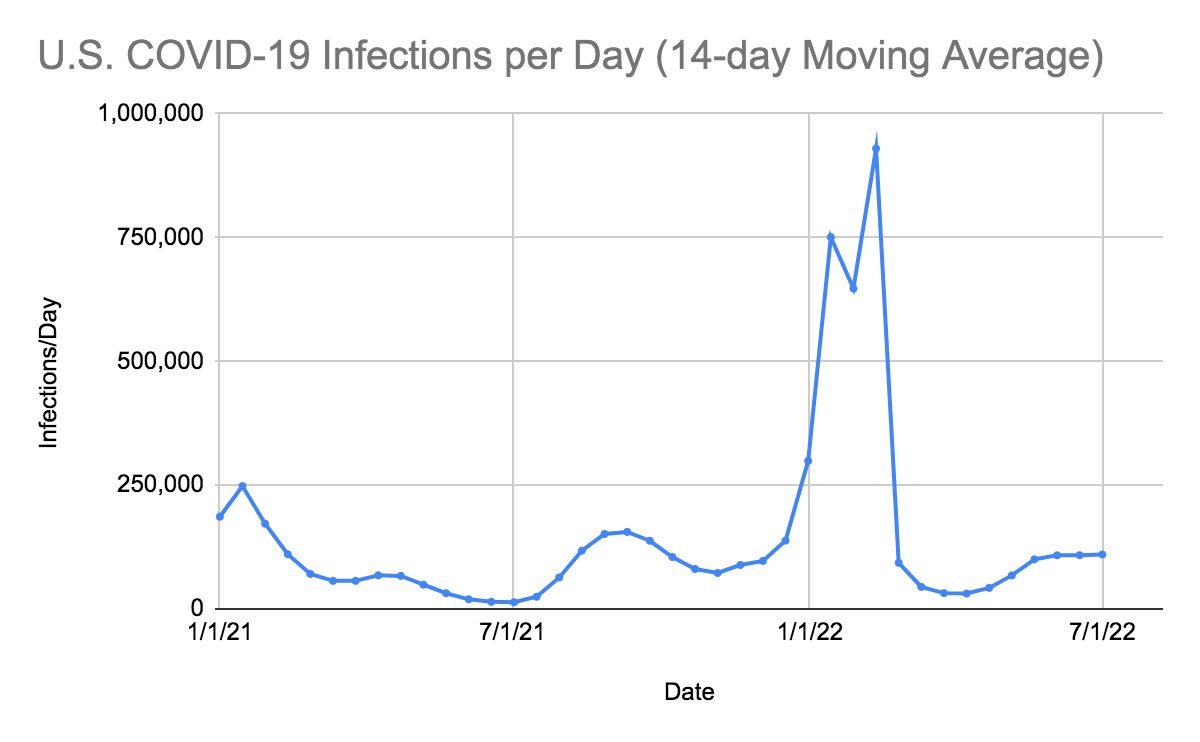
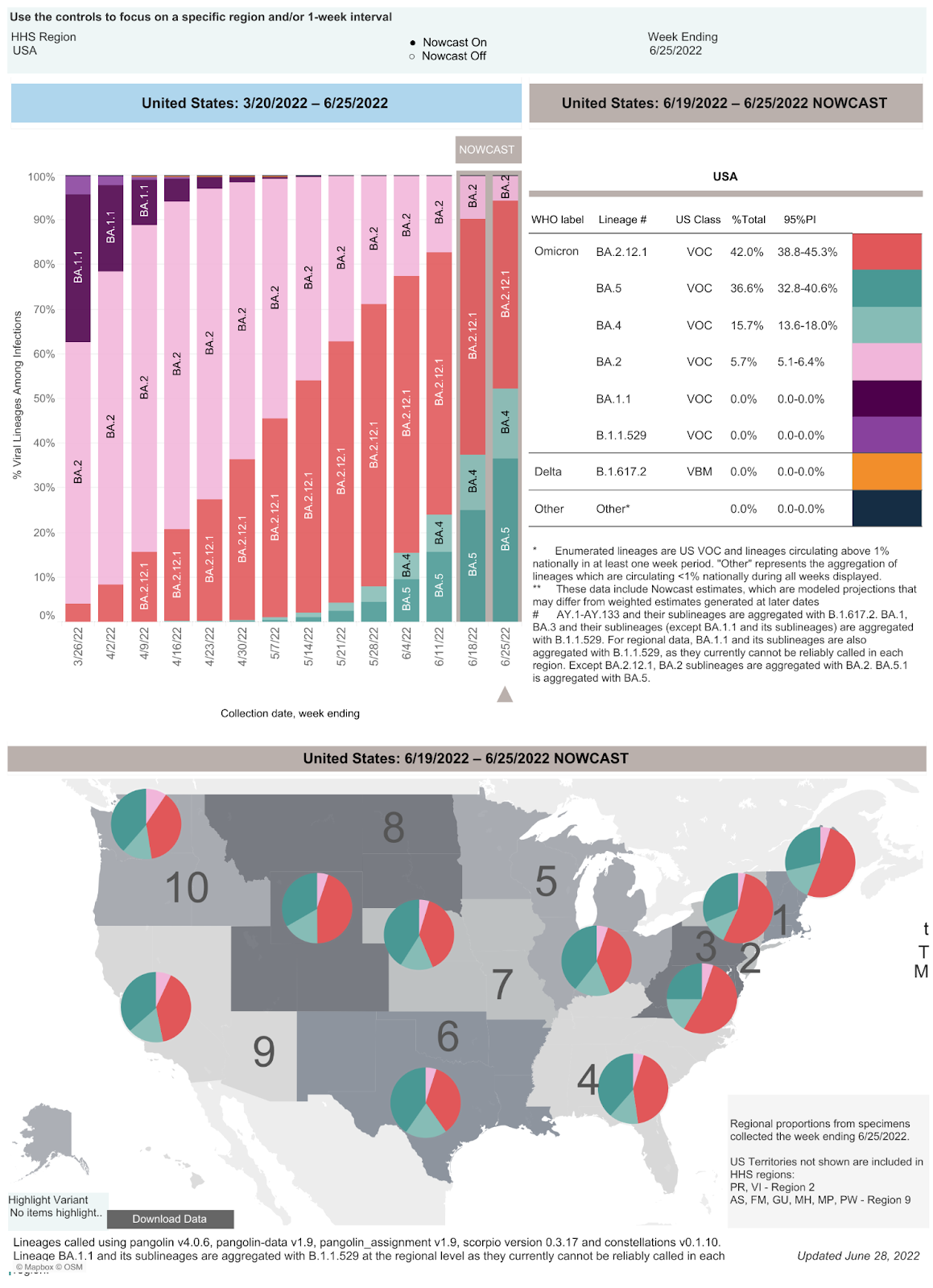
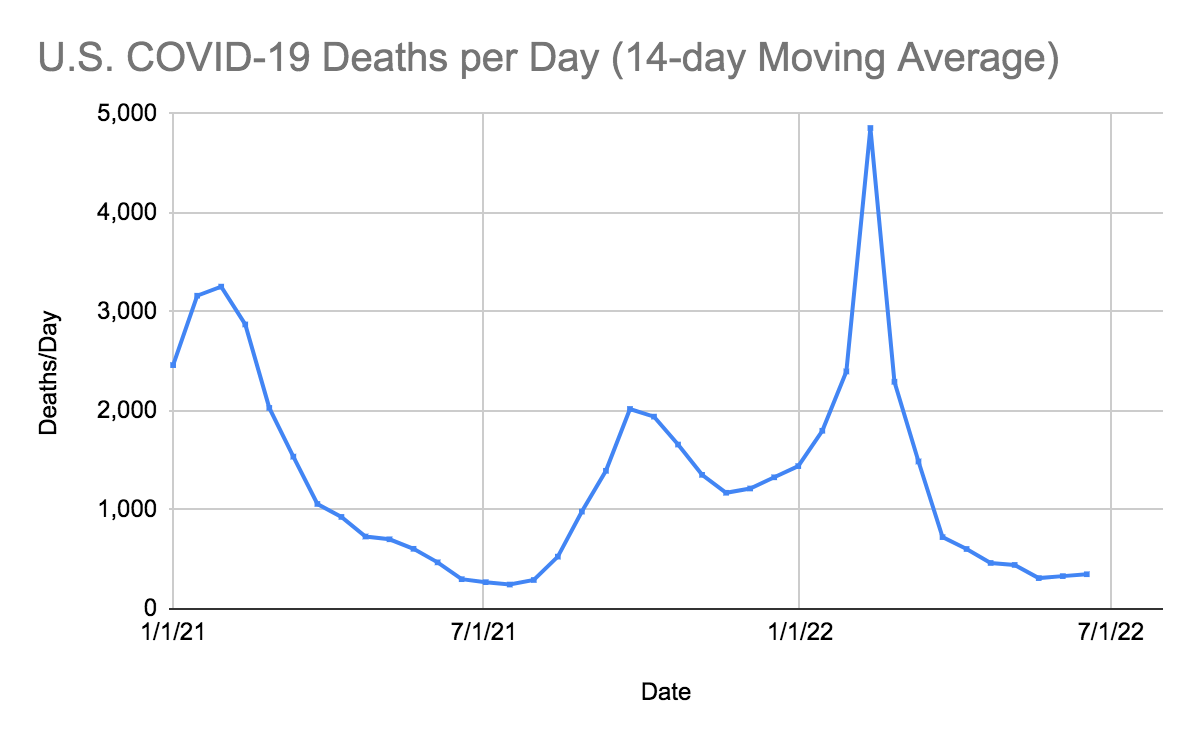
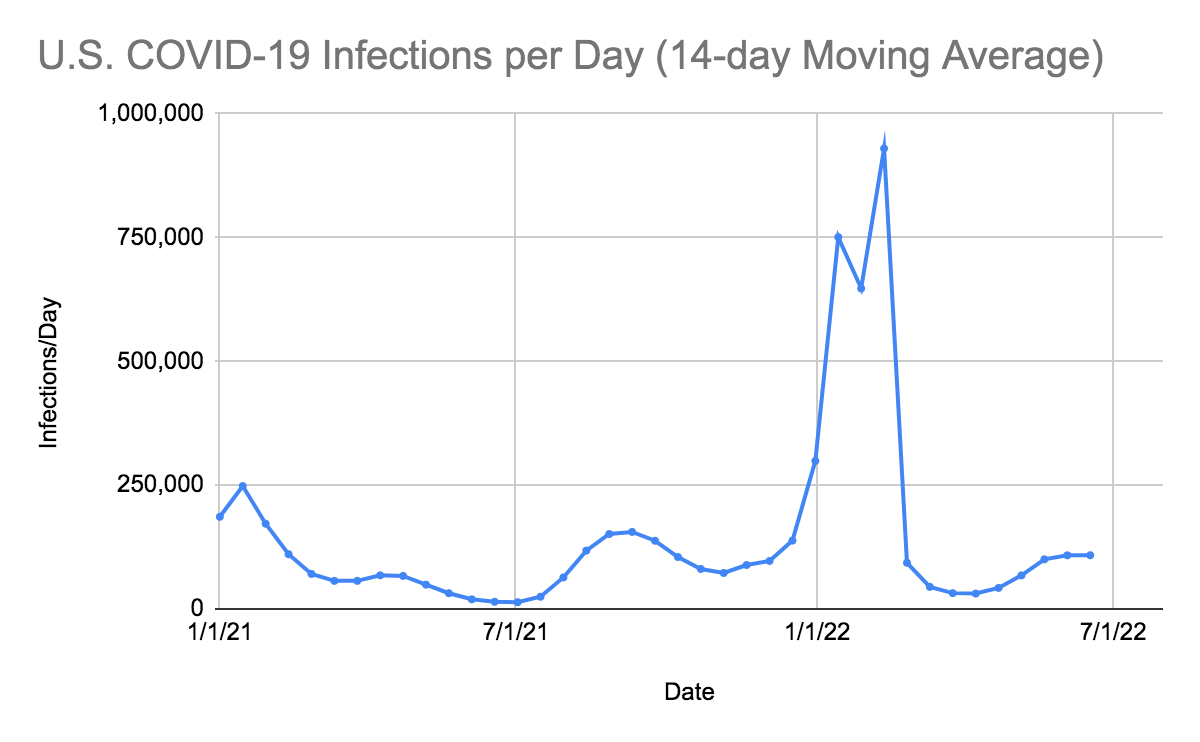
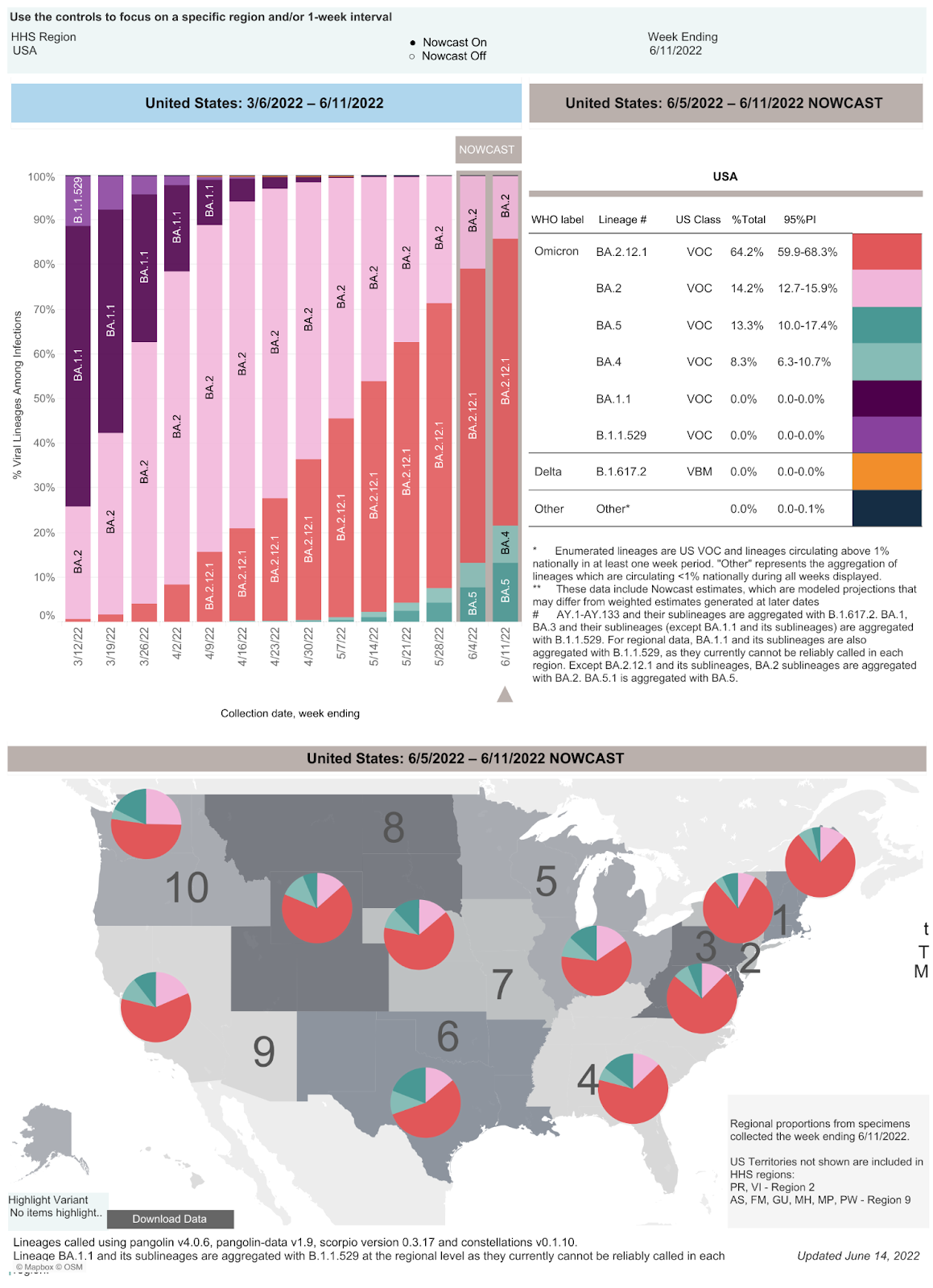
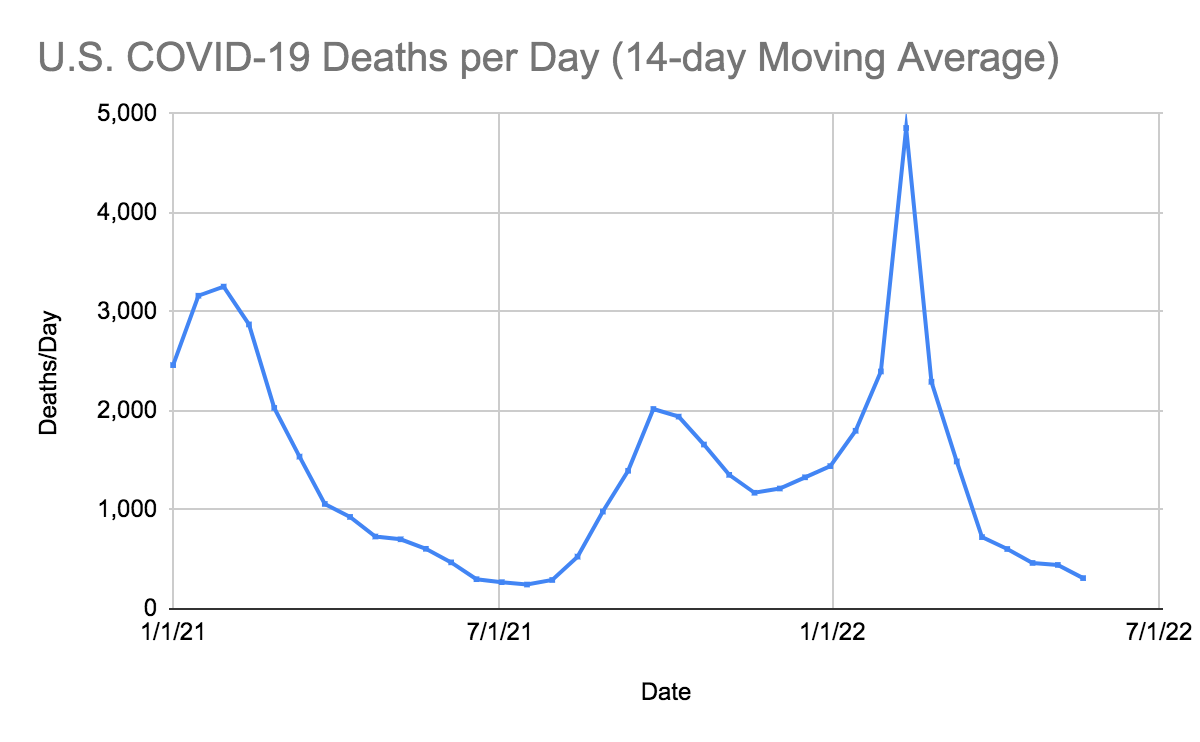
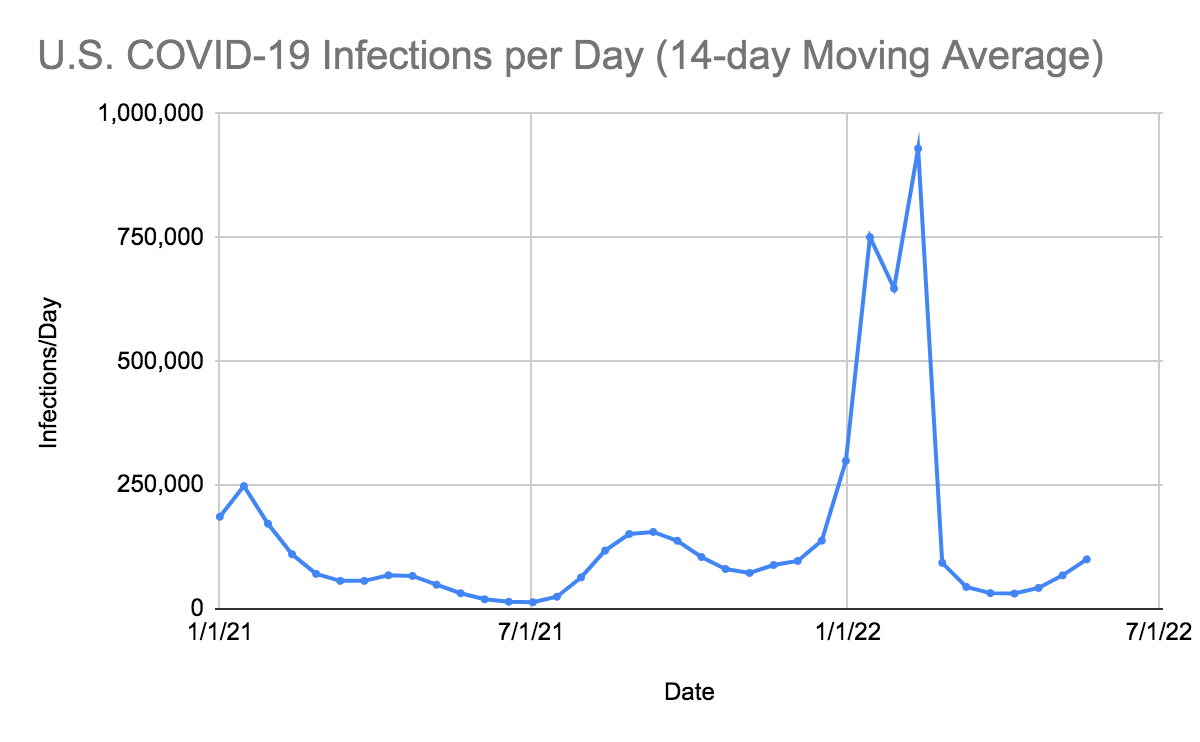
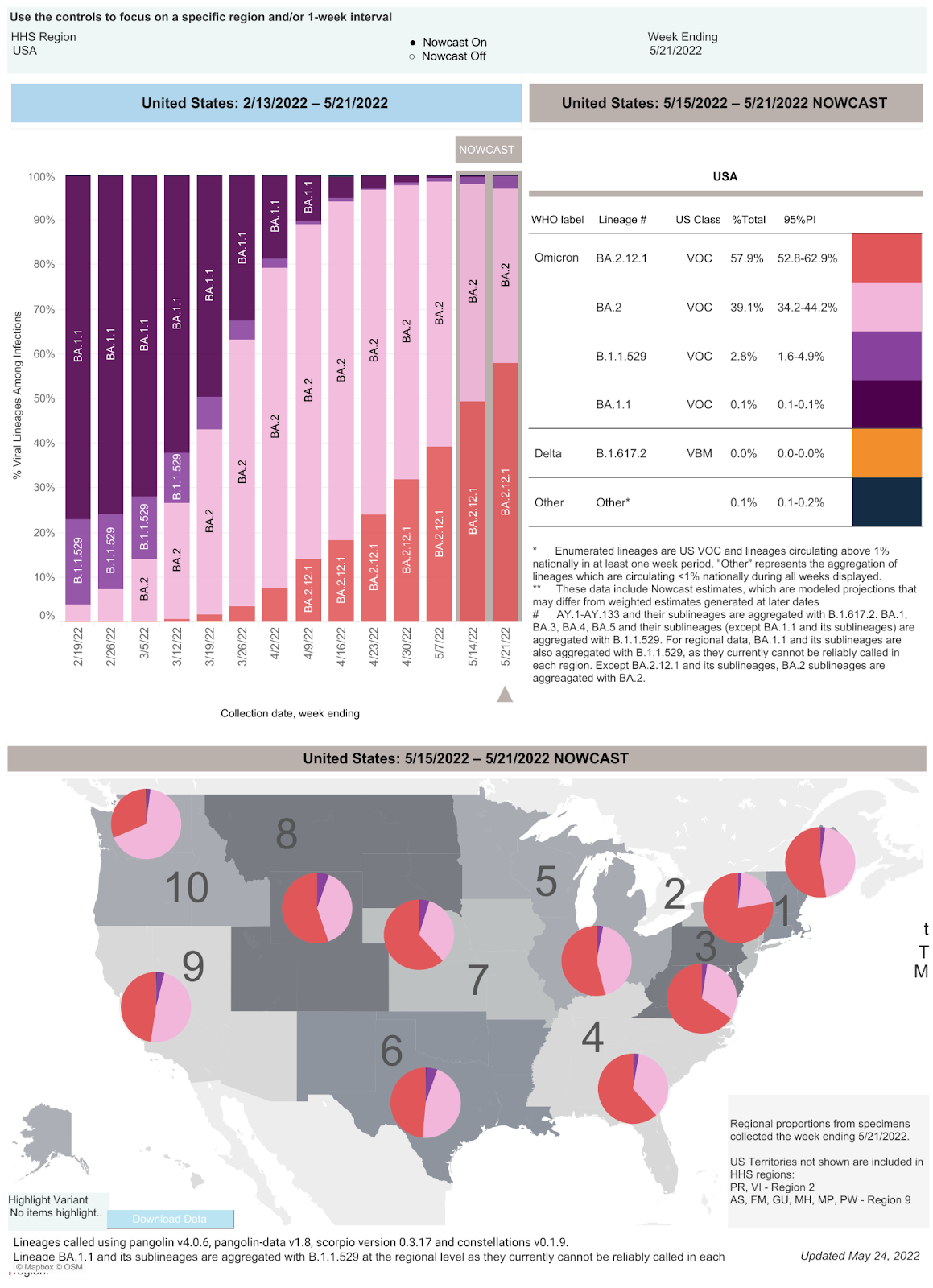
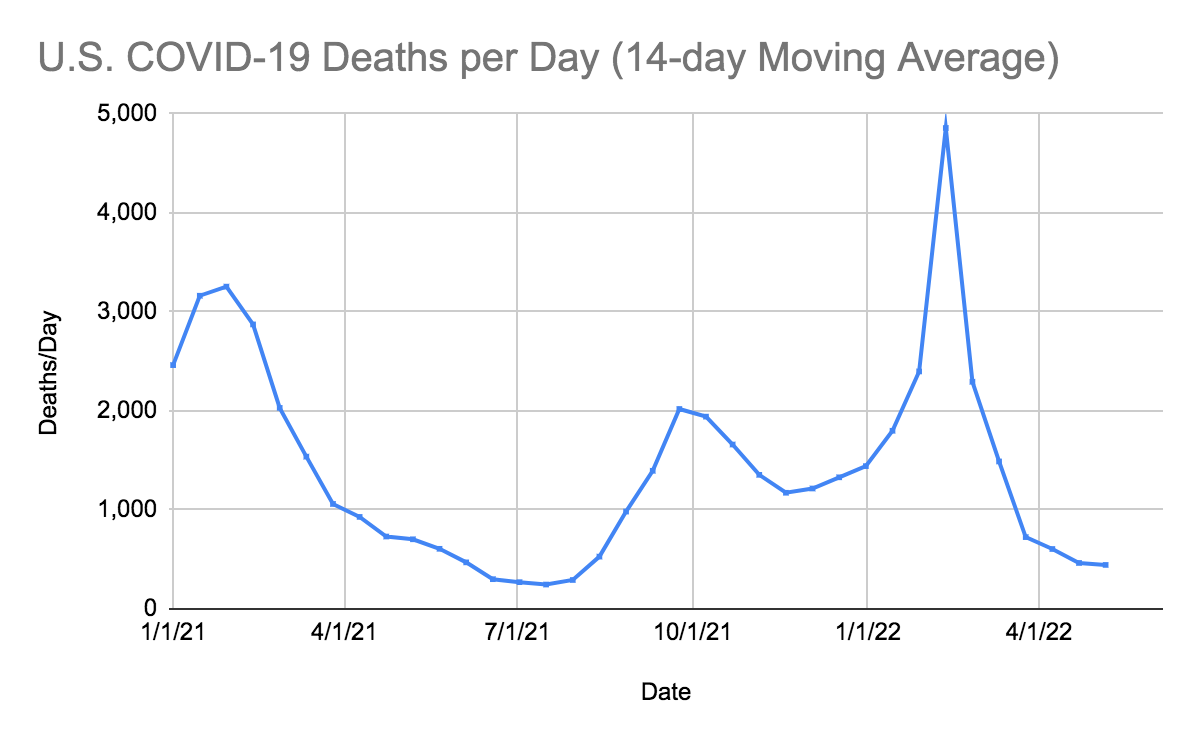
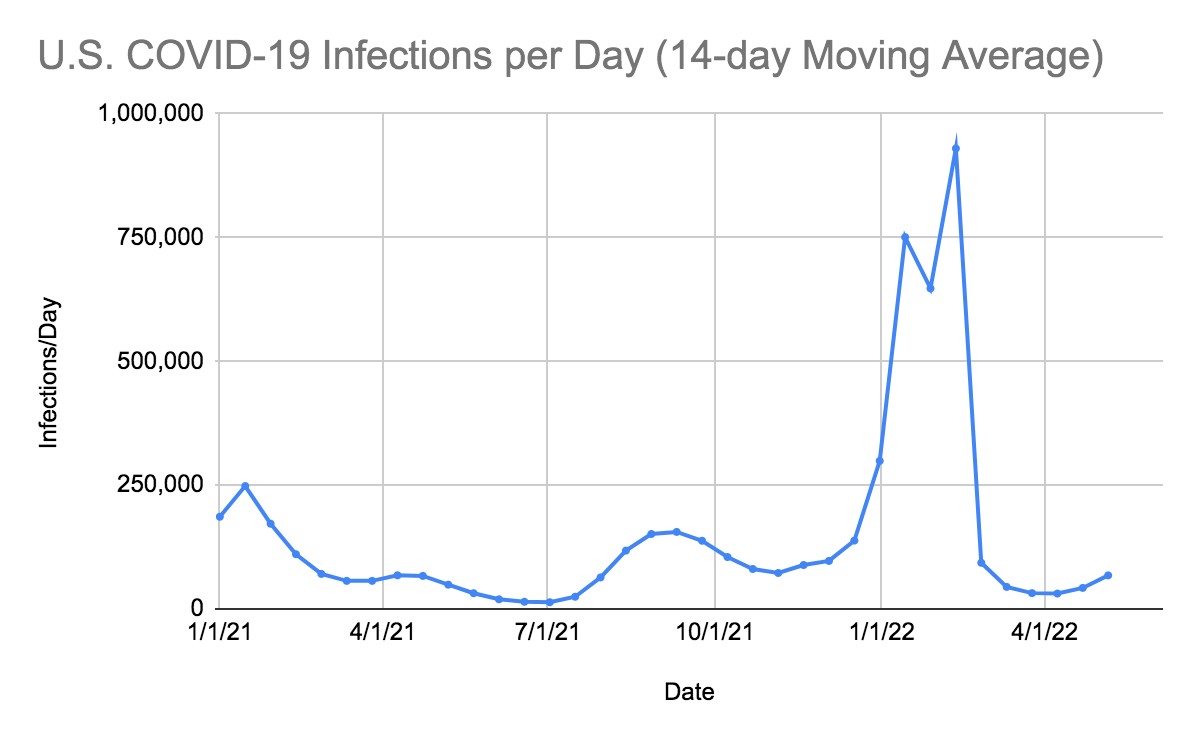
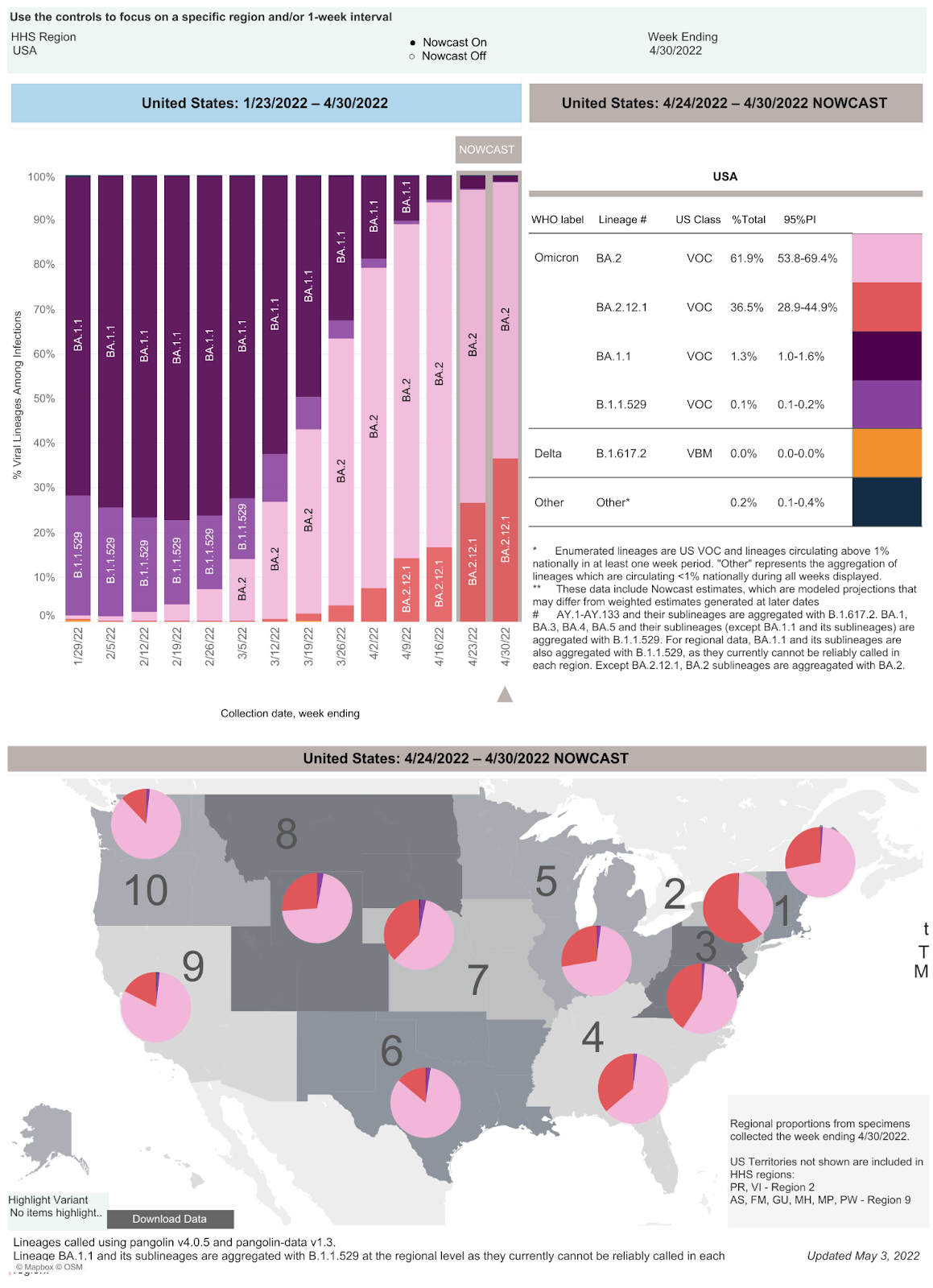
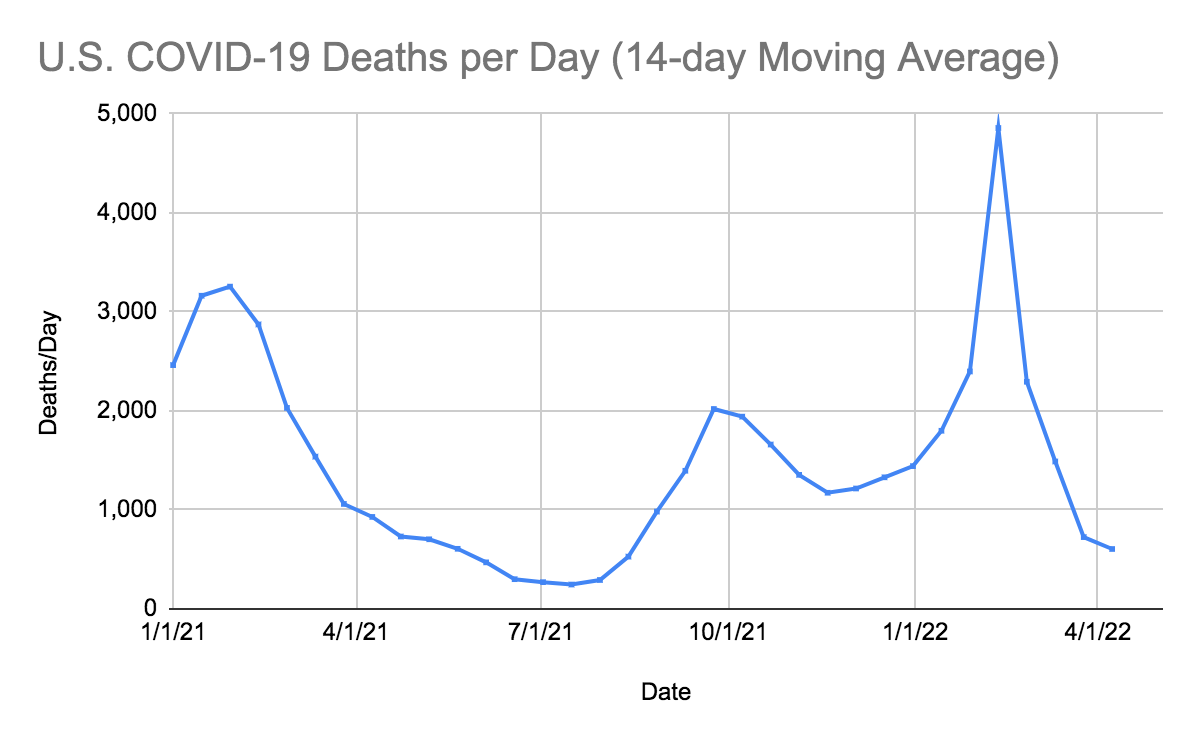
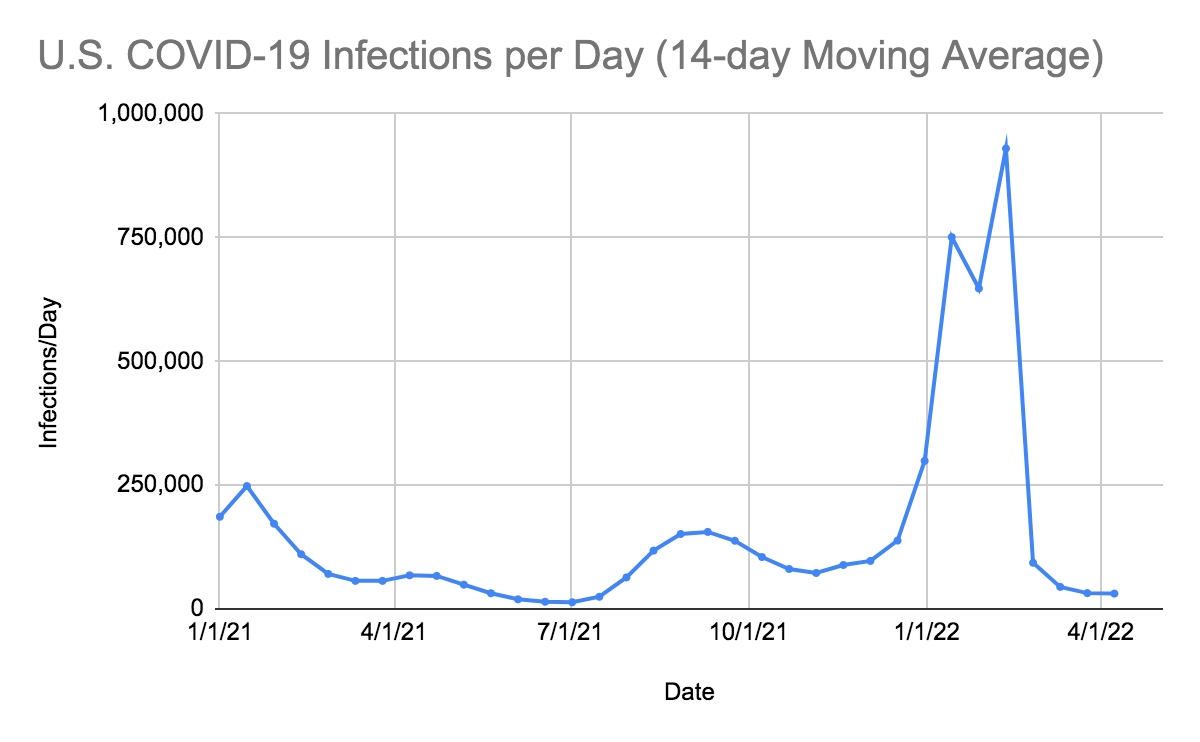
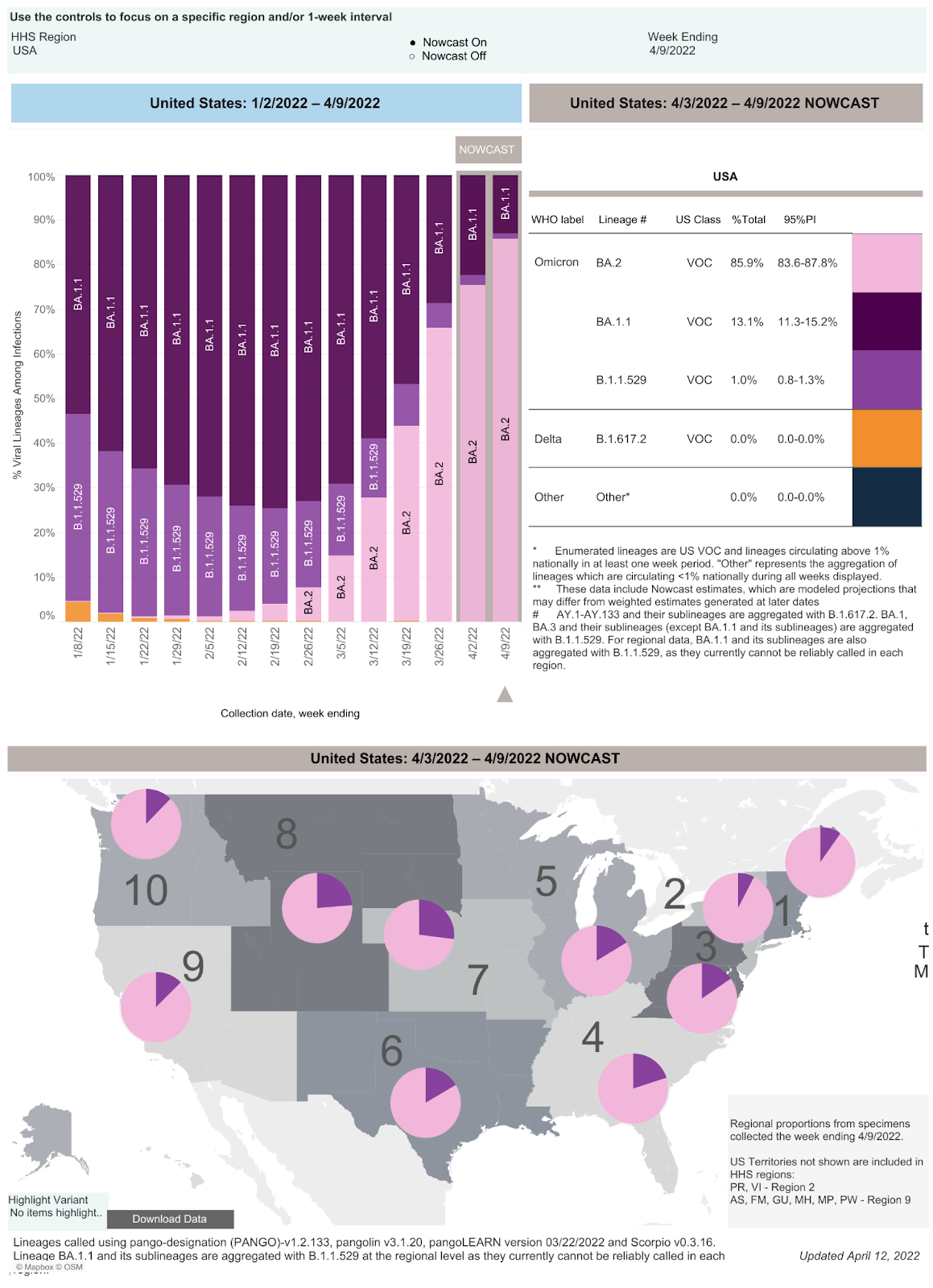
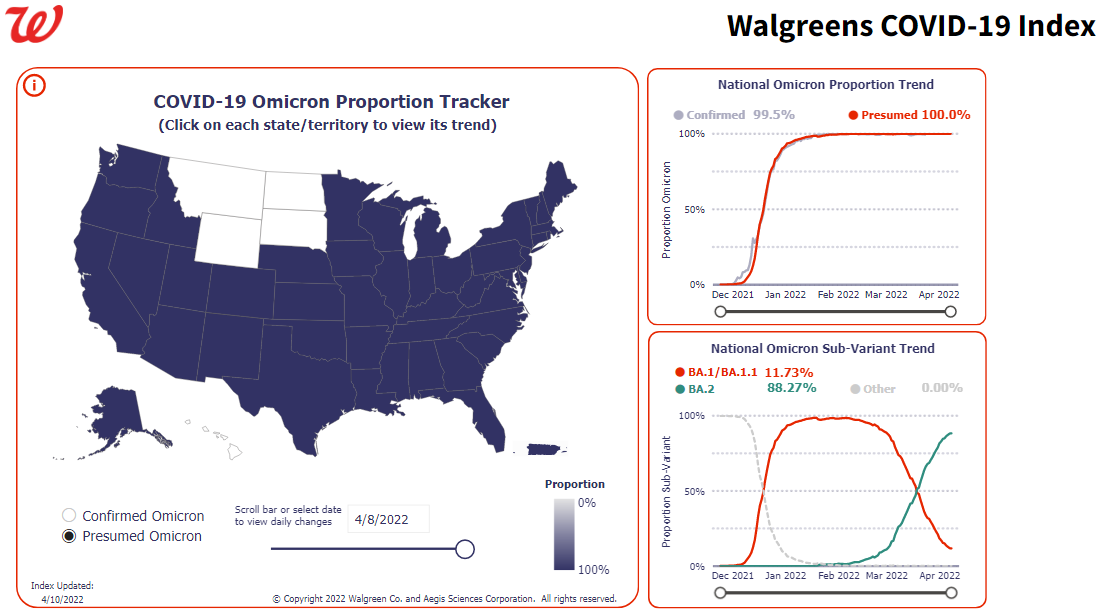
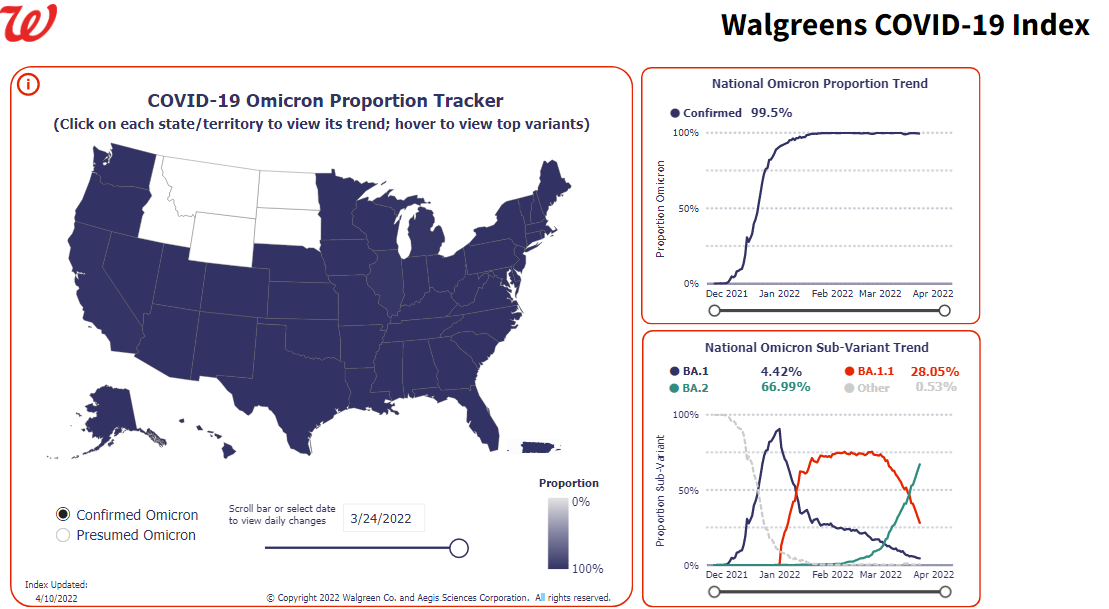
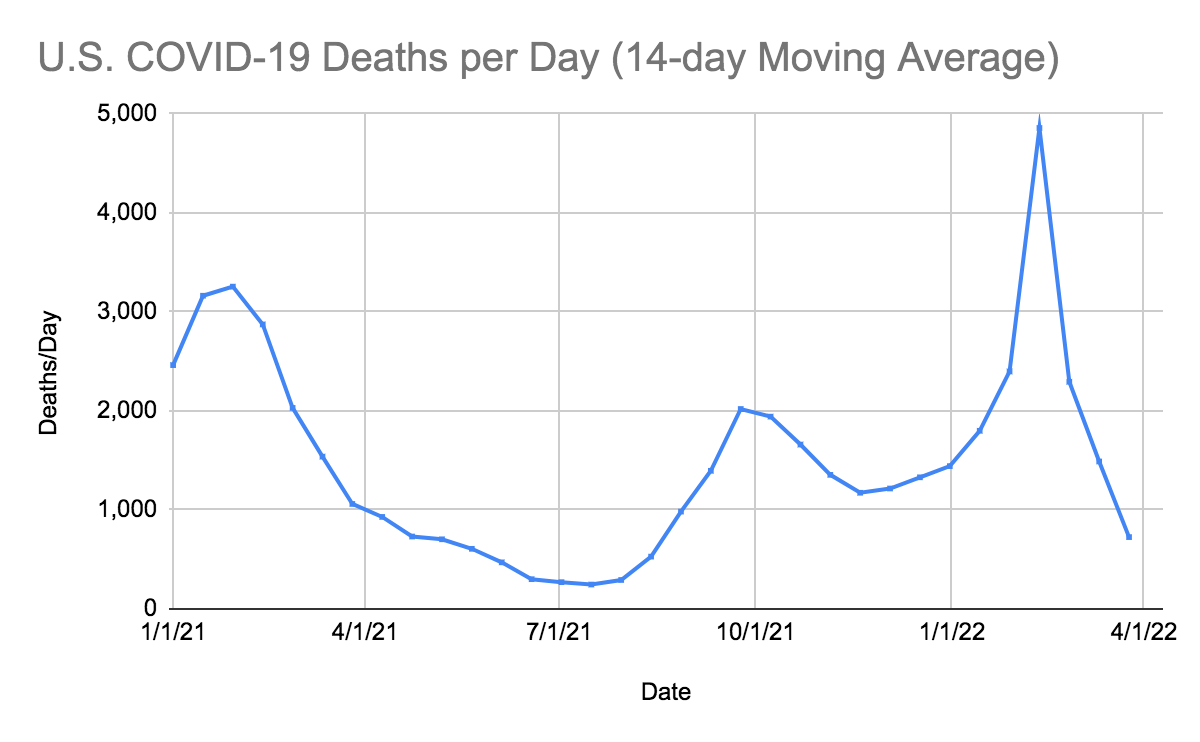
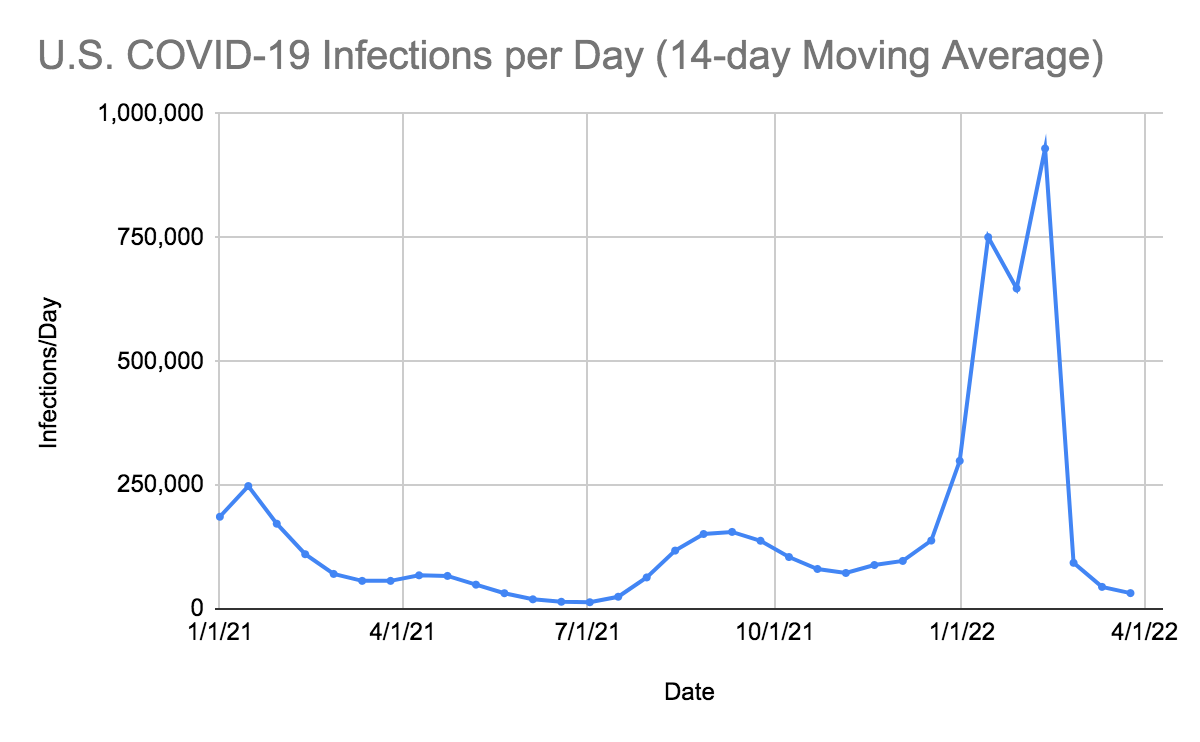
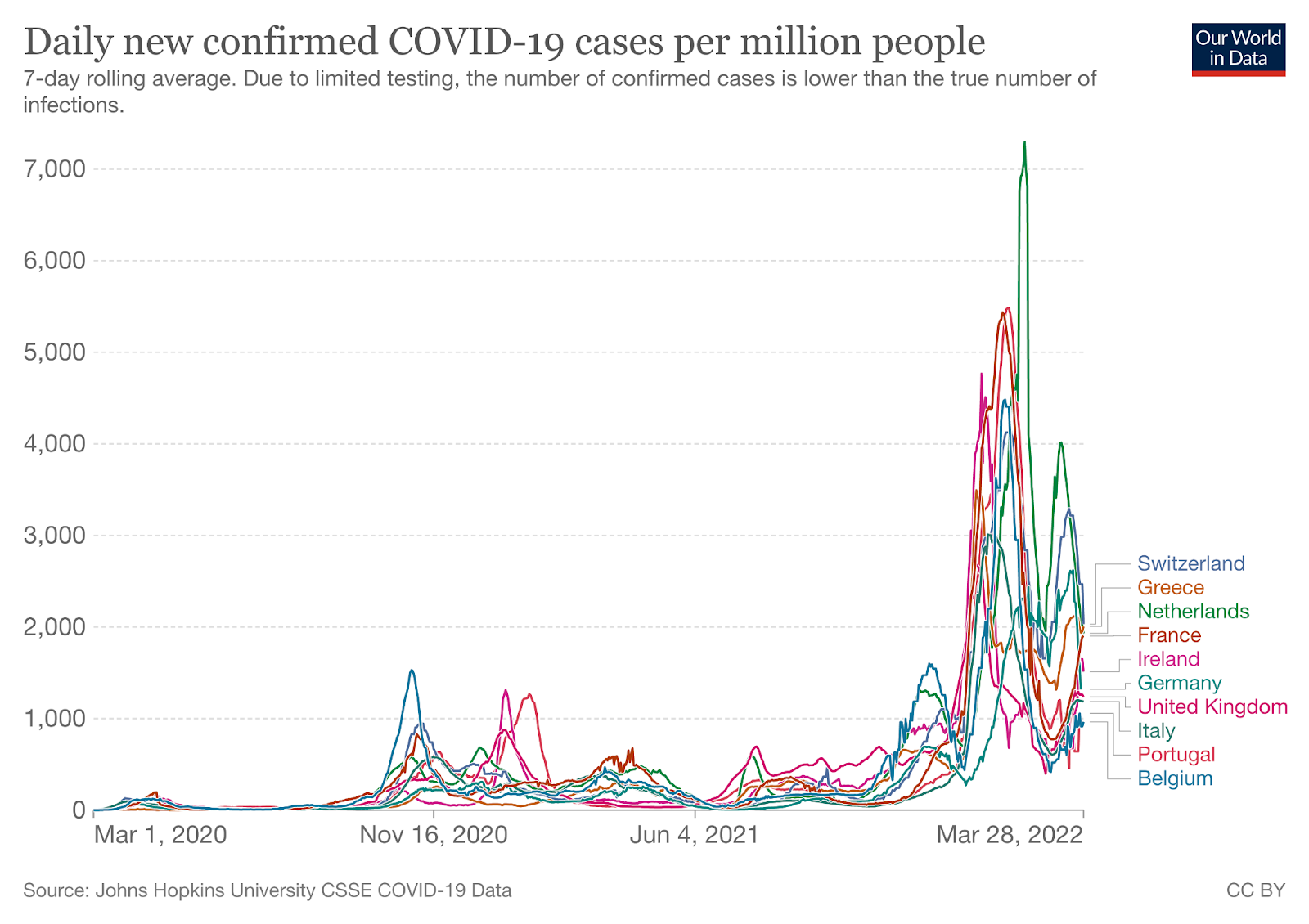
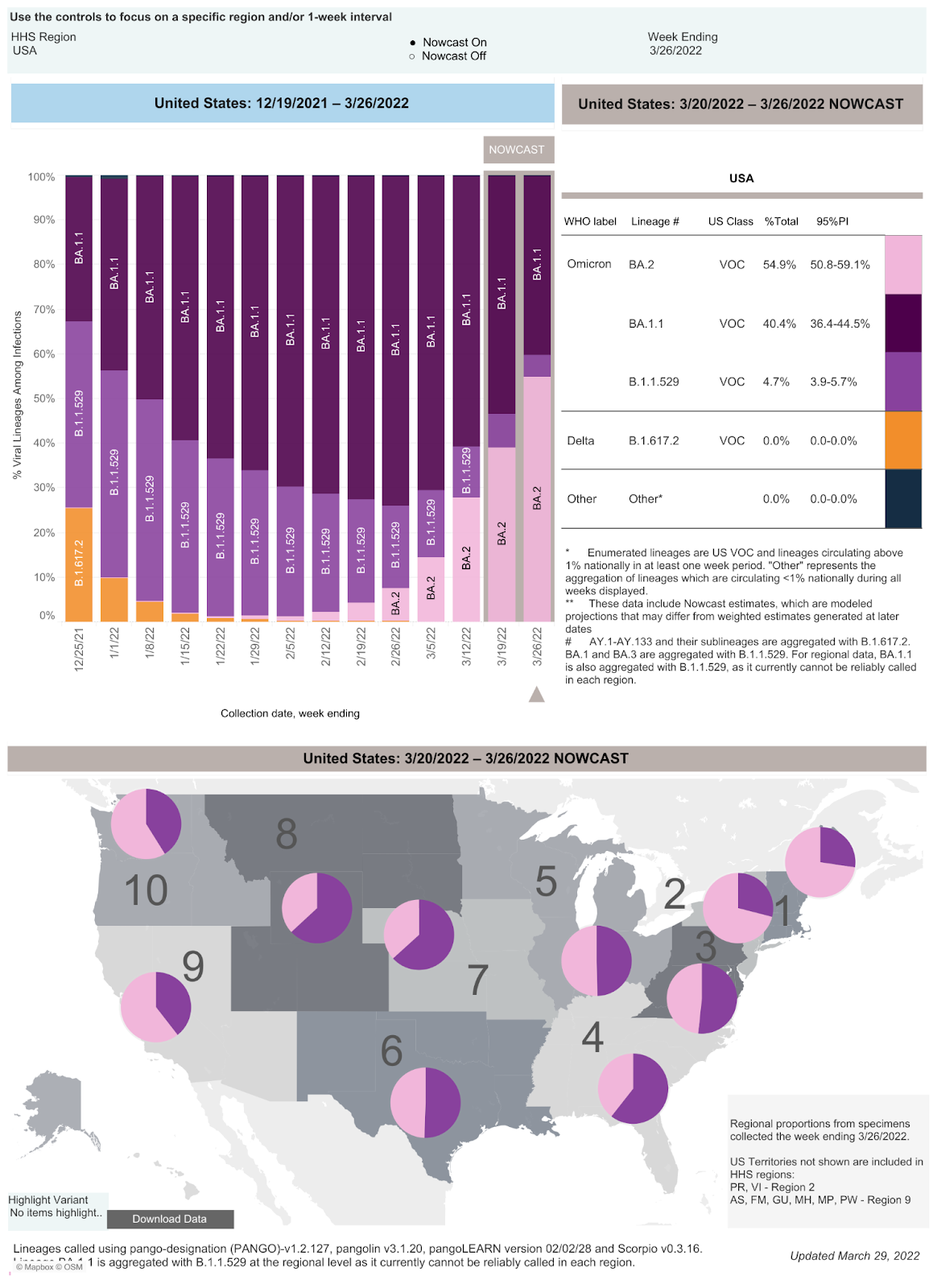
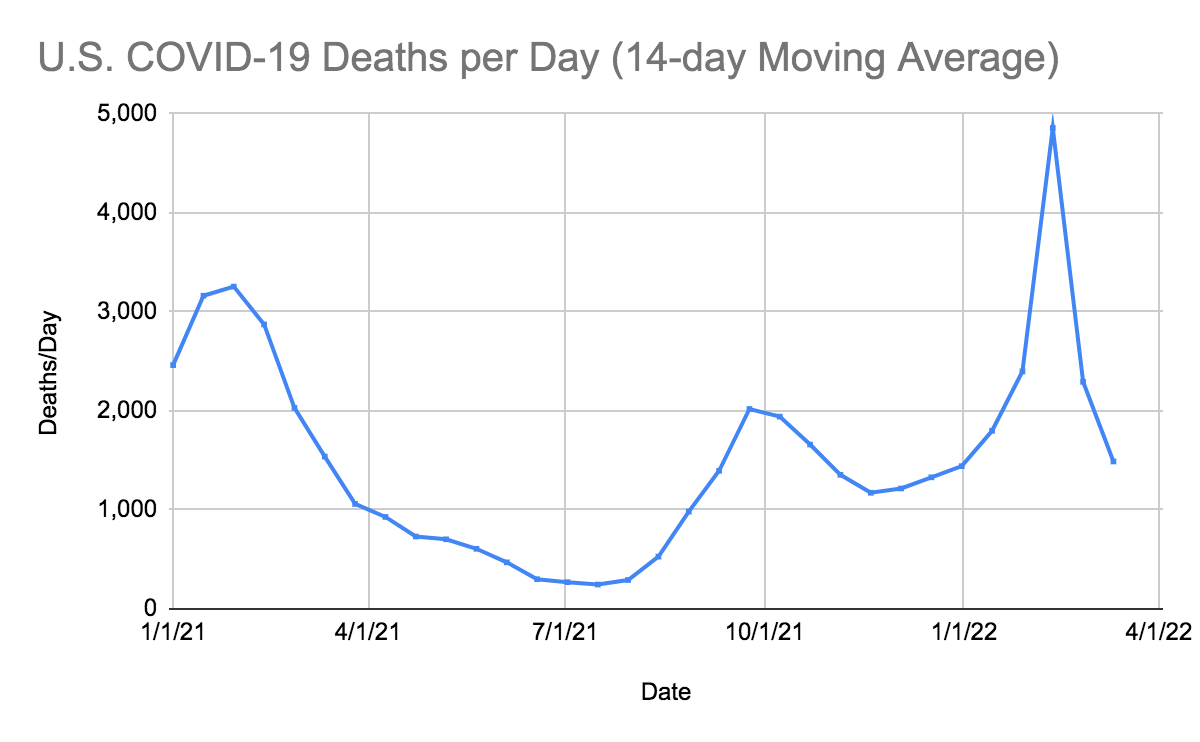
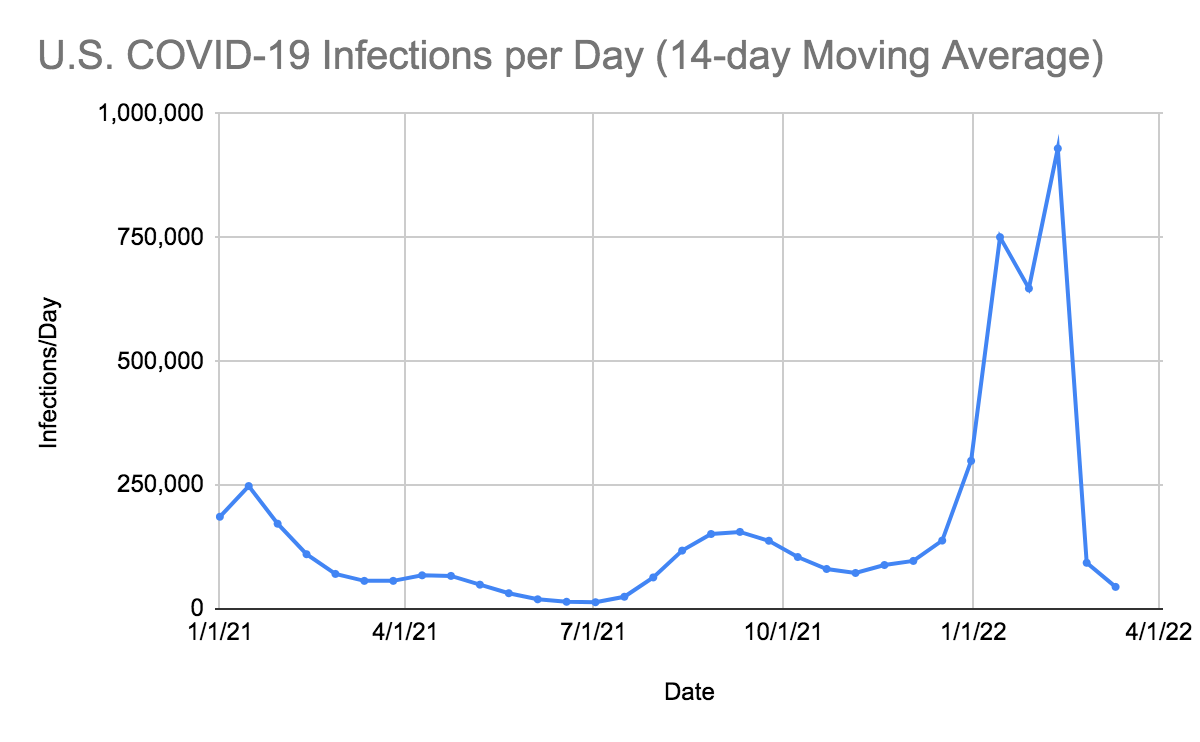
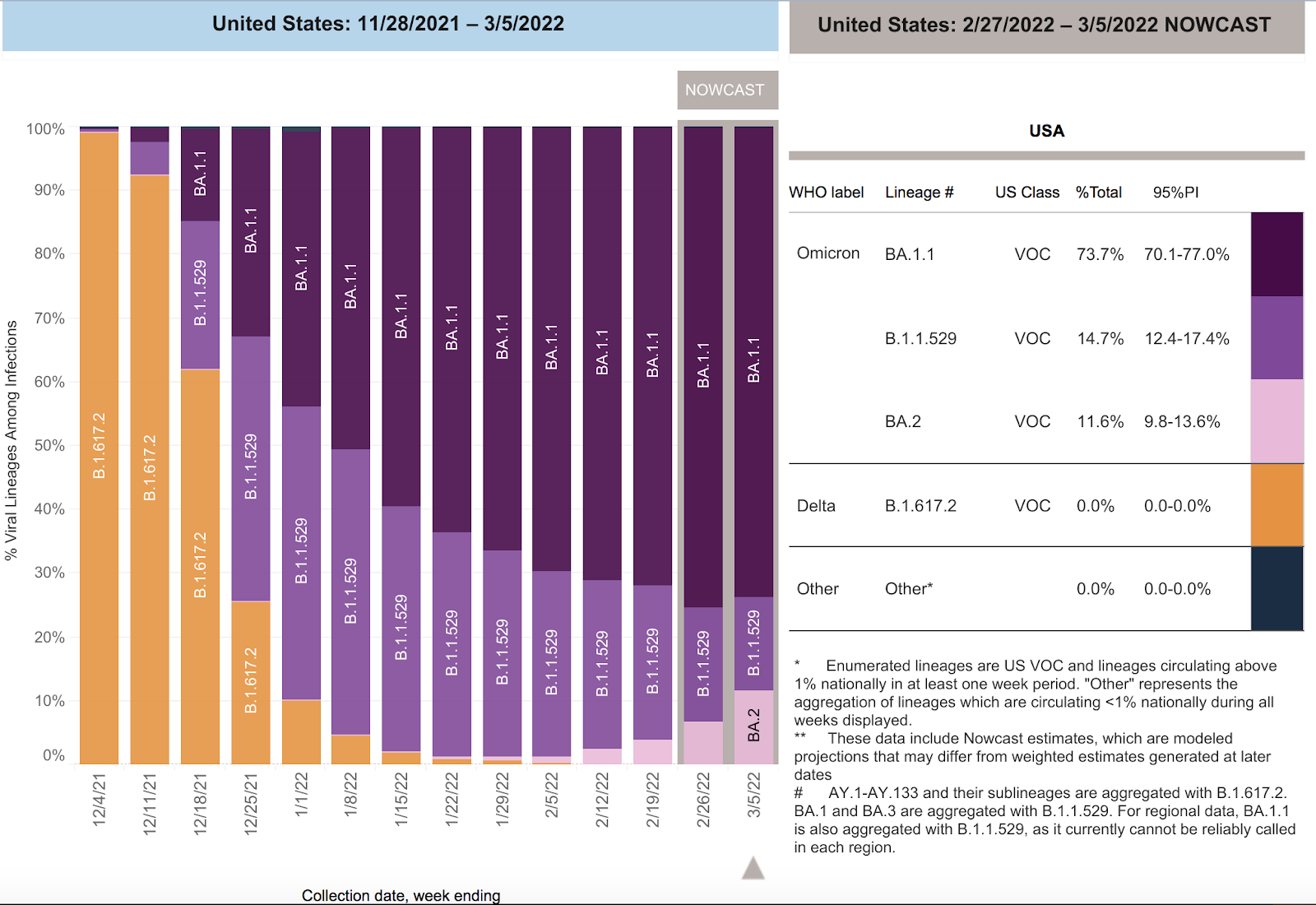
SARS-CoV-2 infections per day have been increasing in the United States for 14 consecutive weeks despite underreporting by states and the failure to capture positive home tests and a decreased screening program in most states. Deaths per day had been decelerating at a rapid rate in the United States but are now increased by 29 more deaths per day. The number of infections have increased as the Omicron BA.2.12.1, BA.2, BA.4, and BA.5 variants of SARS CoV-2 have spread across the nation. The CDC estimates that BA.2.12.1 accounted for 17.3% of isolates, BA.2 accounted for 1.4%, BA.5 accounted for 65.0%, BA.4 accounted for 16.3%, and B.1.1.529 accounted for 0% in the week ending June 25.
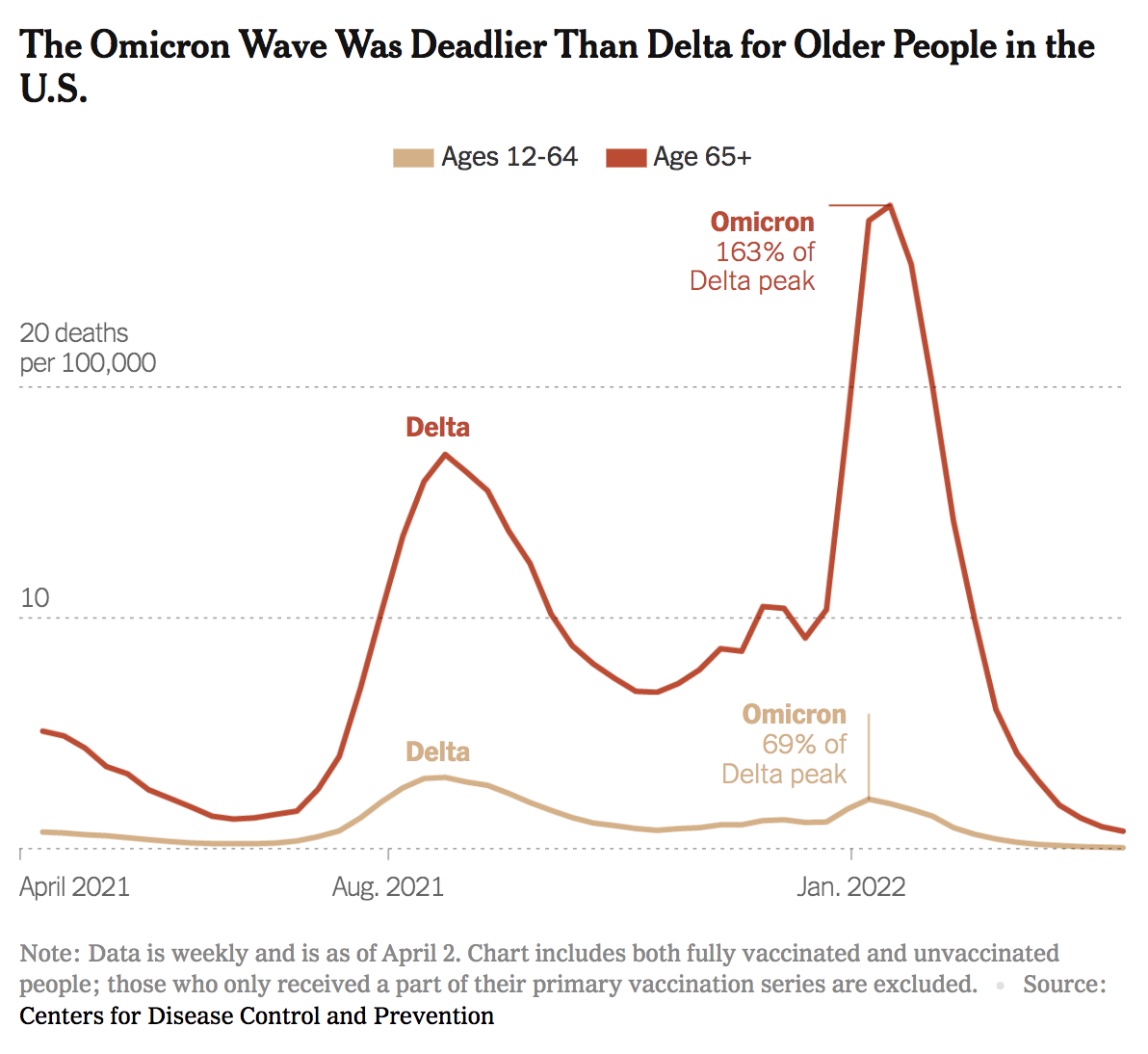
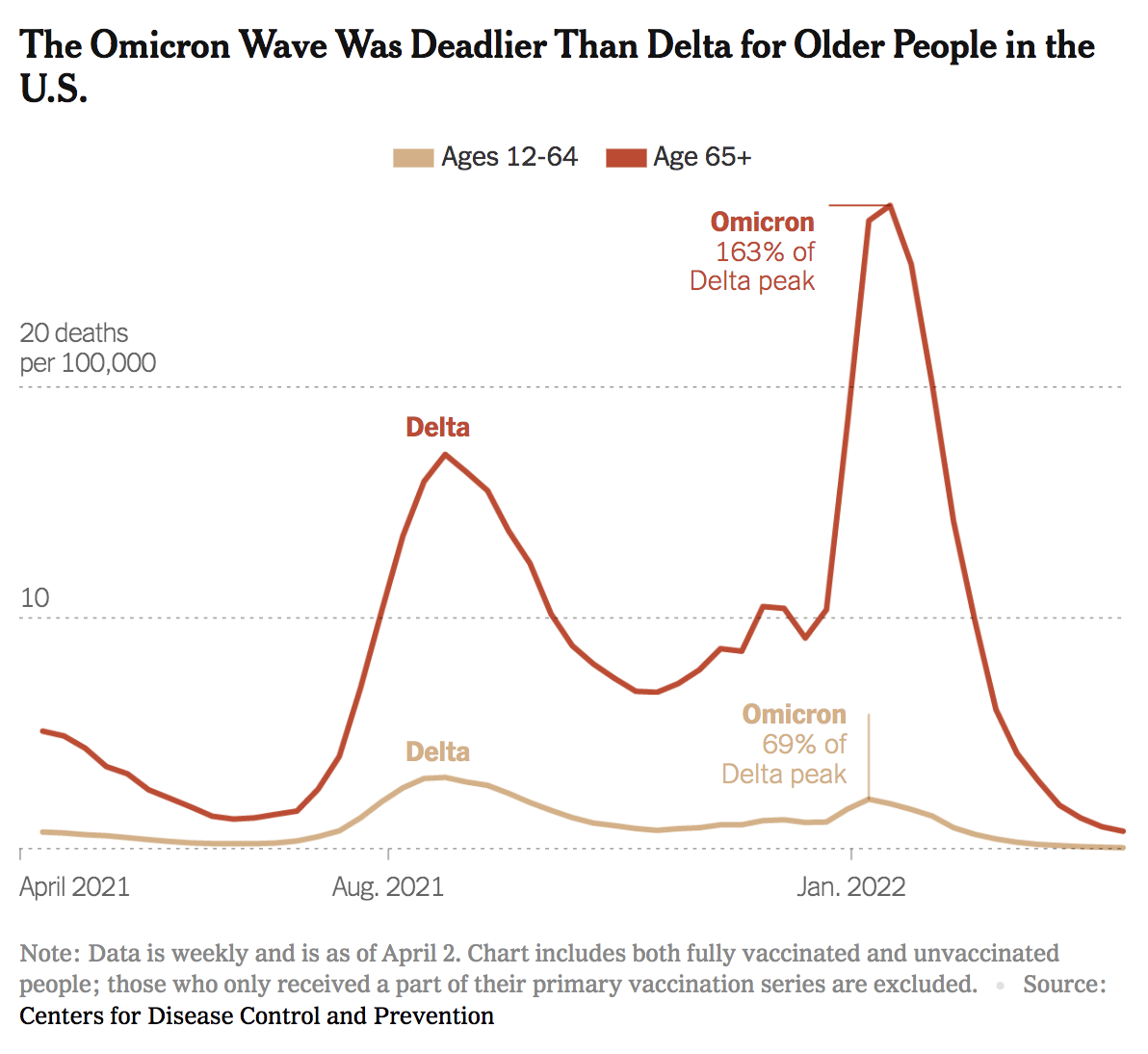
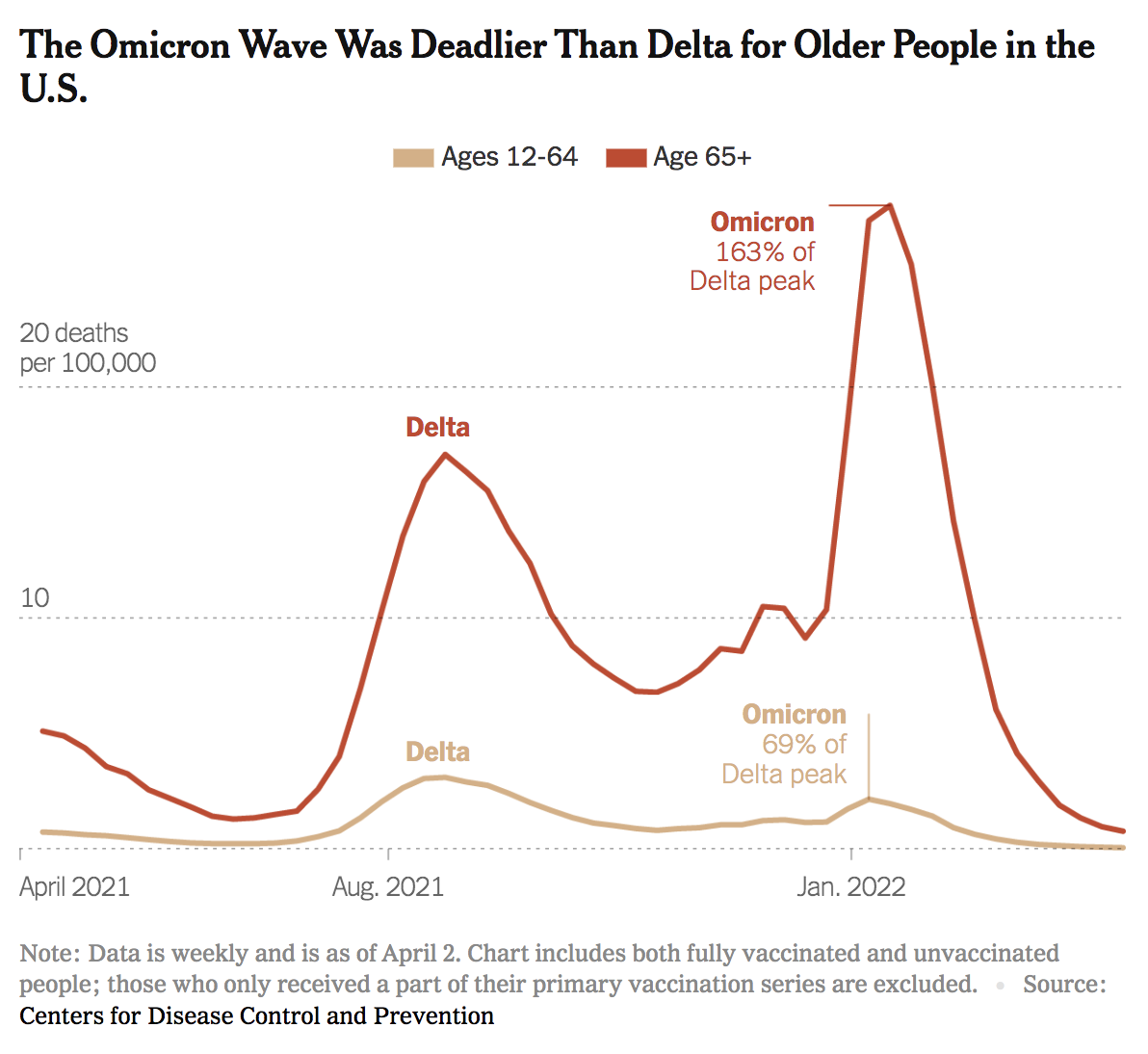
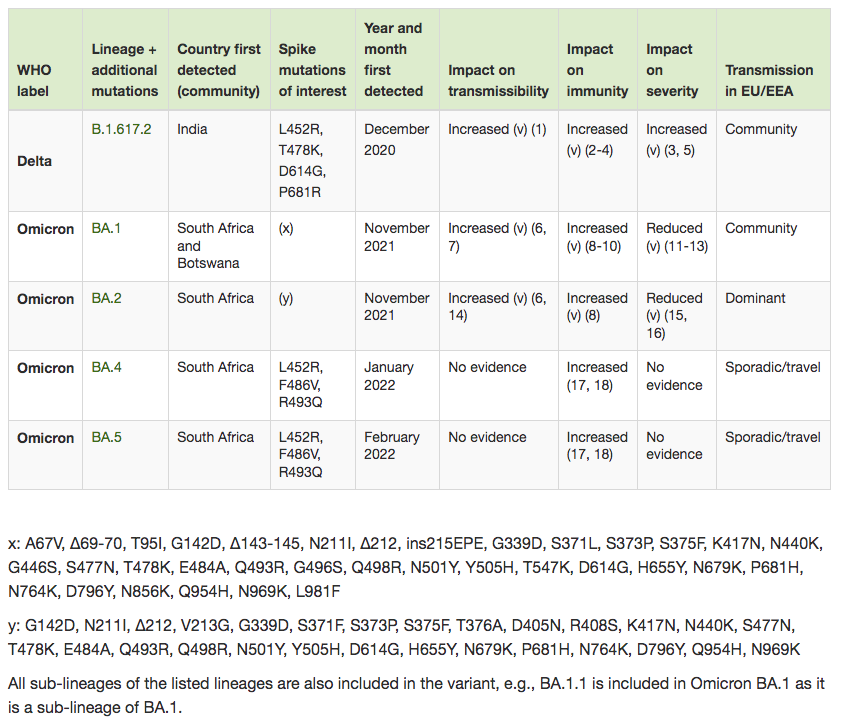
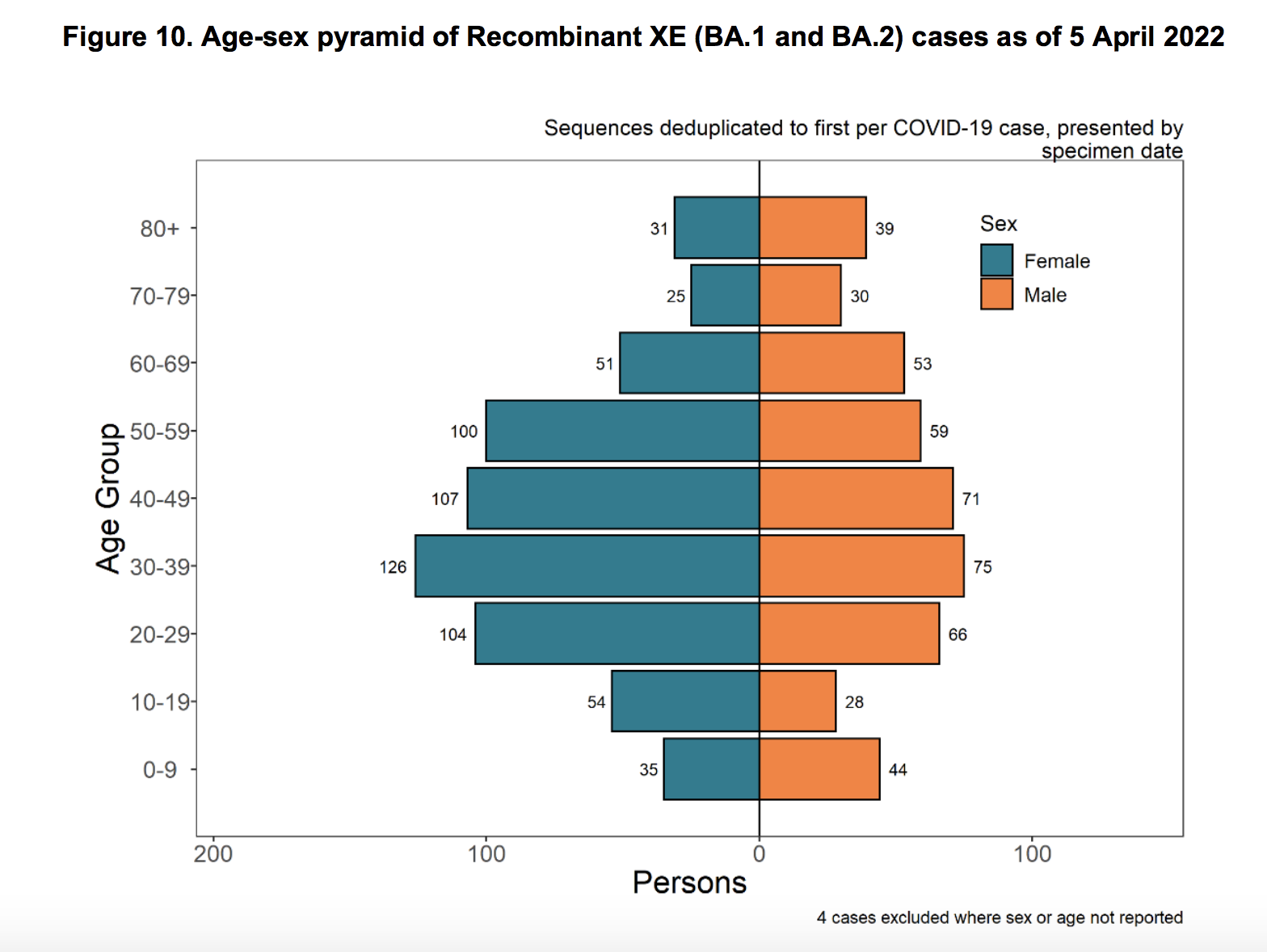
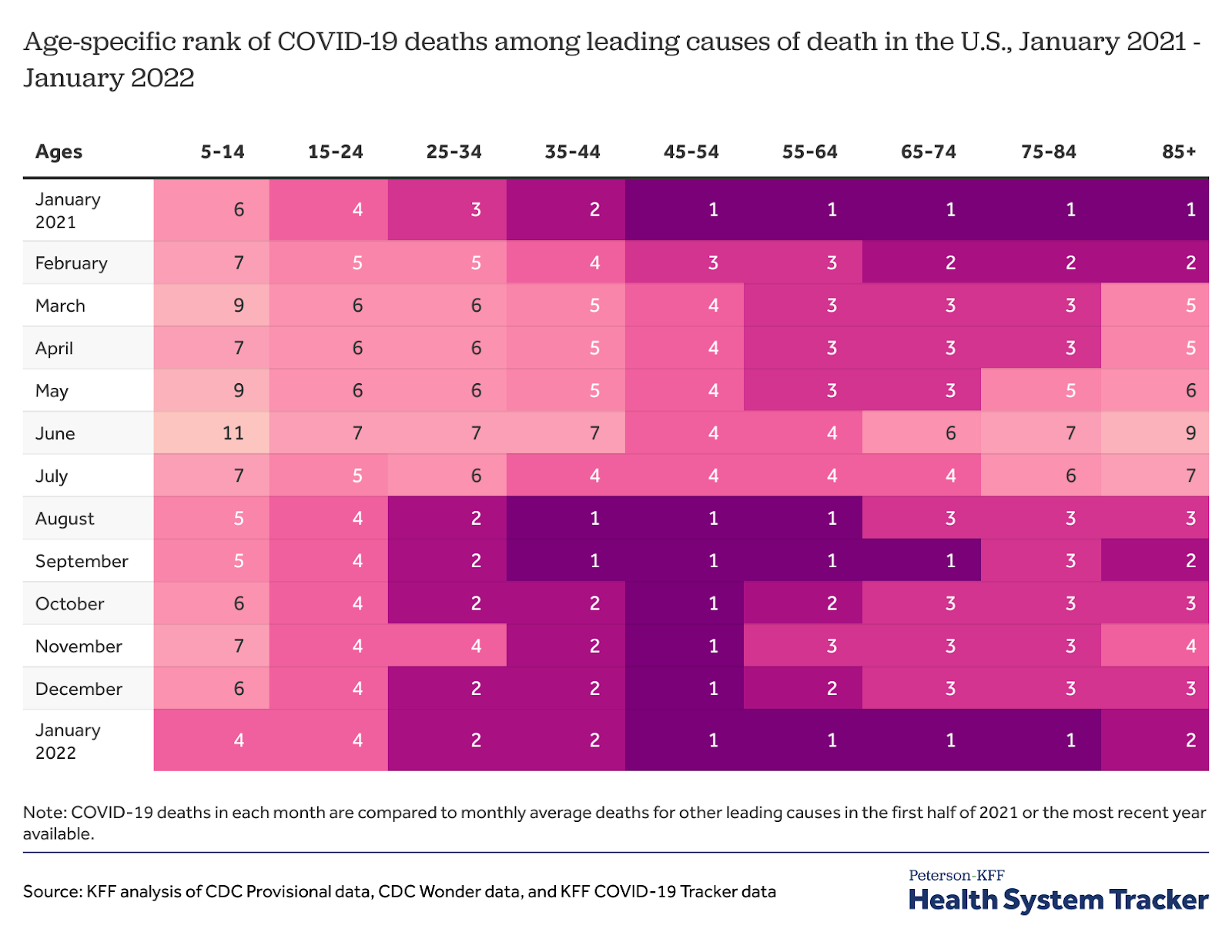
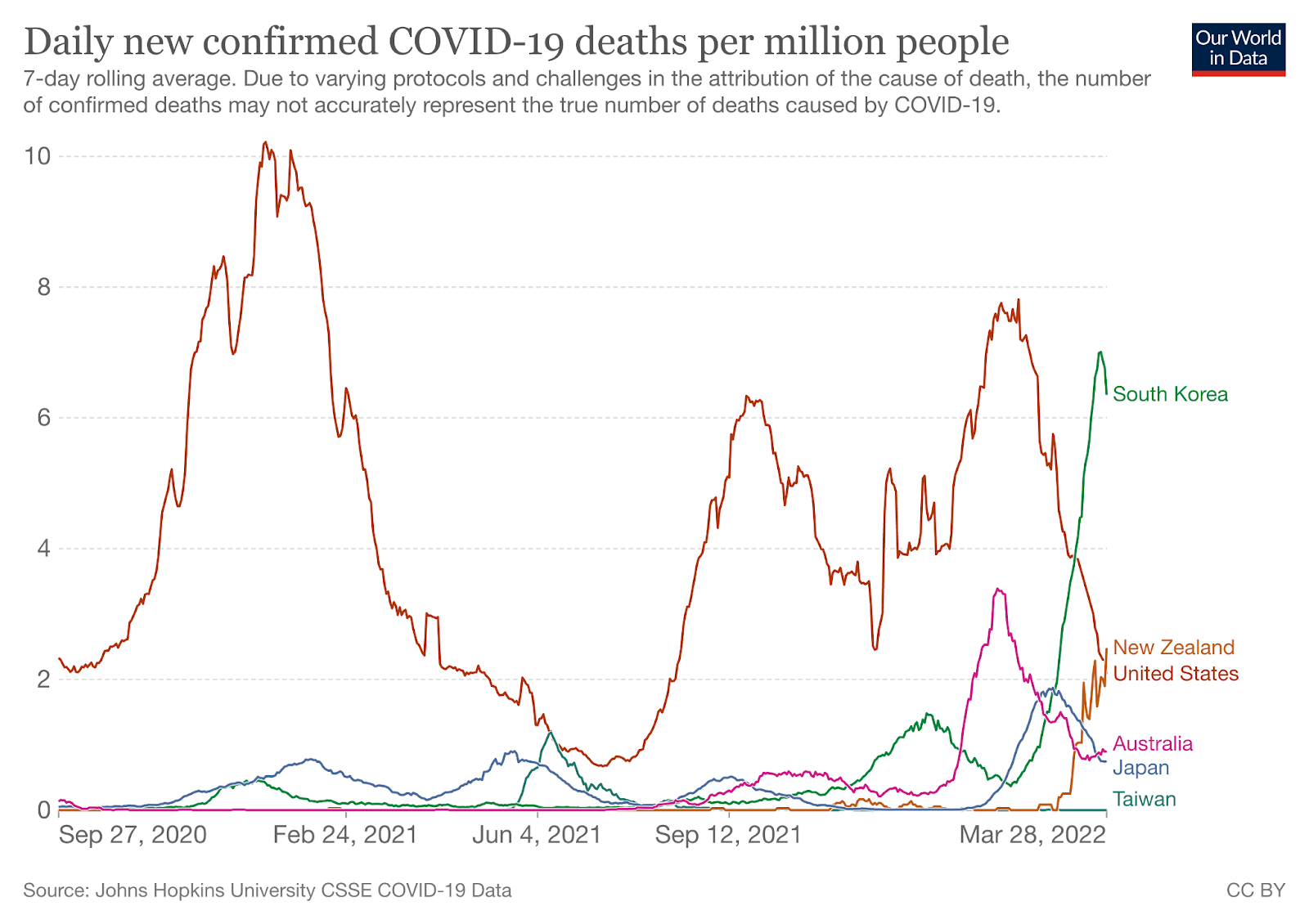
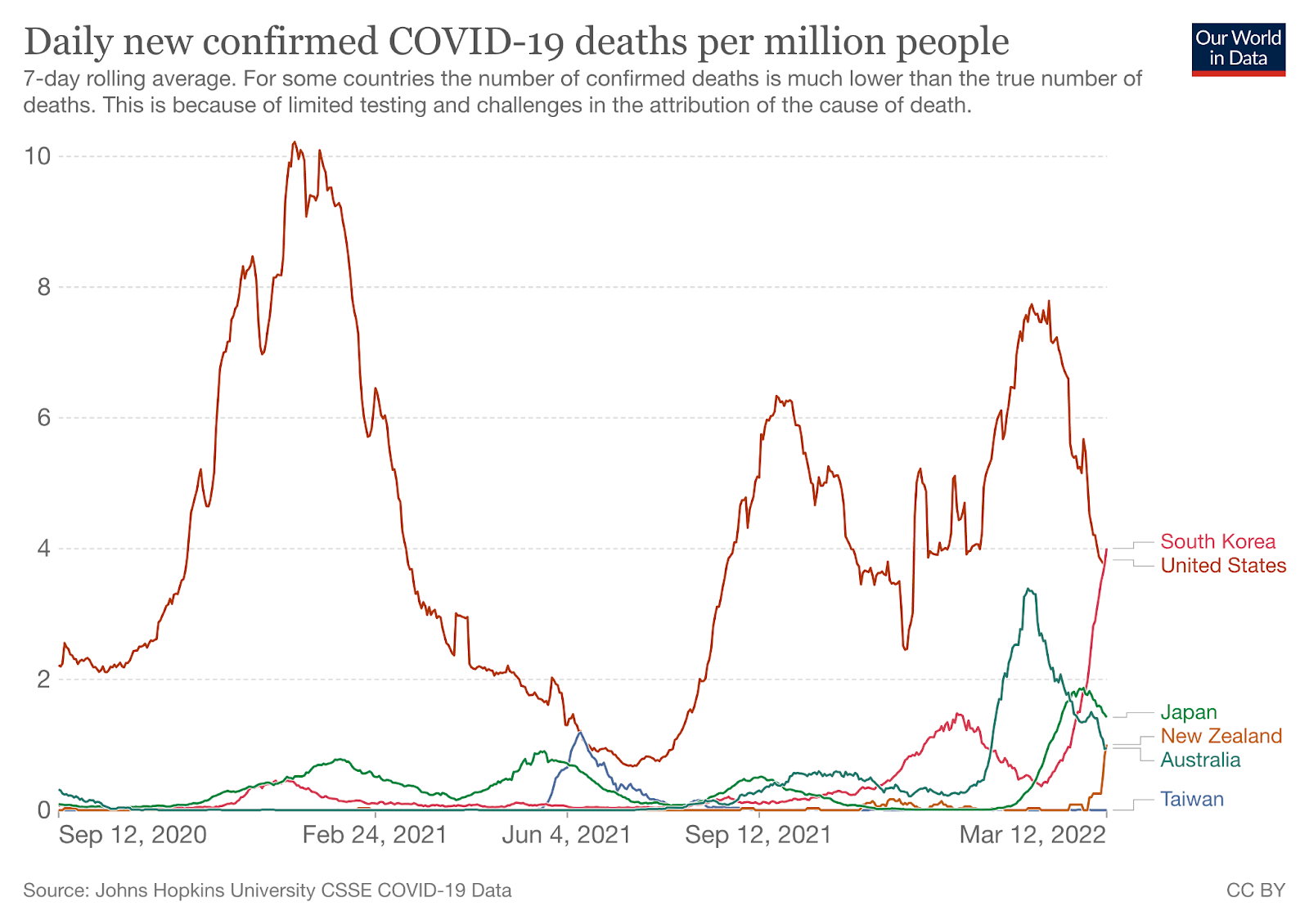
We frequently hear messaging from health officials and politicians that Omicron is “mild,” especially compared to the Delta variant, and as a result, many of our patients believe that they no longer need to wear their masks. This is a dangerous misconception. SARS-CoV-2 still remains a highly transmissible, airborne virus. The following graph, based on CDC data from April 2, 2022, shows that Omicron deaths in people over 65 are much higher than Delta deaths in the same age group. In fact, the peak of Omicron deaths in people over 65 years of age is 163% higher than the Delta peak. The death rate from Omicron is only lower than Delta in the populations between 12 and 64 years of age. Until we have more data on these newer mutants of SARS-CoV-2, we will not know the lethality of each variant. It may take months to measure objective differences in the death rates of new circulating variants. We recommend that all of our patients and family members continue to wear N95 masks in all enclosed spaces.
In patients treated with Paxlovid for five days who have persistent symptoms and continued positivity, we feel that clinicians should consider giving a second course of Paxlovid for five days. Boucau et al have demonstrated that in a study of seven patients with recurrent symptoms, “High viral loads (median 6.1 log10 copies/mL) were detected after rebound for a median of 17 days after initial diagnosis. Three had culturable virus for up to 16 days after initial diagnosis.” This was not due to resistance-associated mutations of the virus, suggesting that the course of therapy may be inadequate in this group of persistently infected patients.
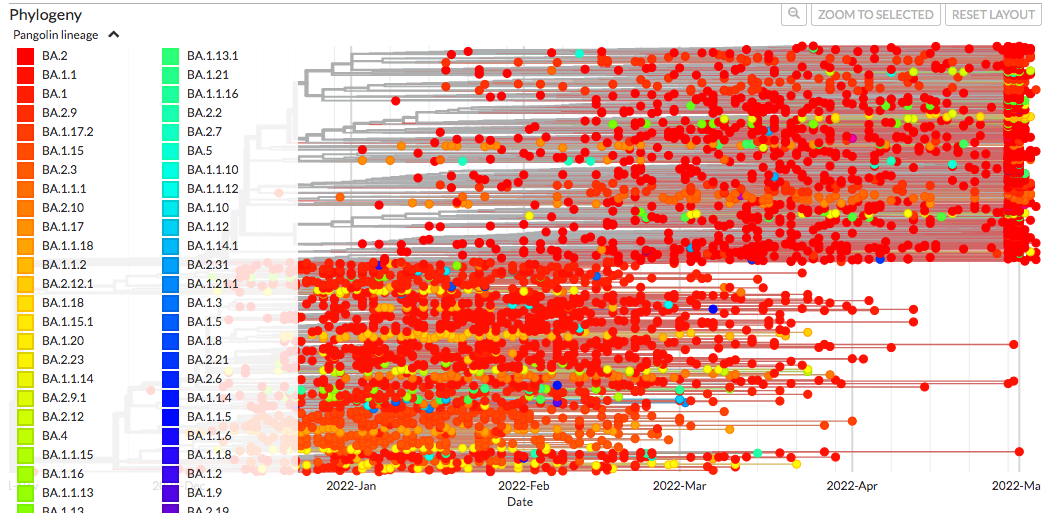
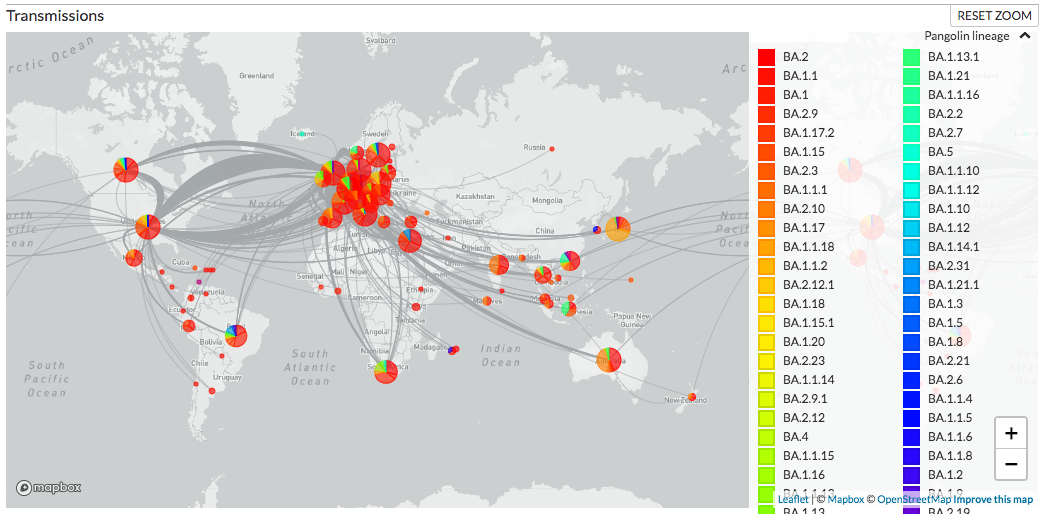
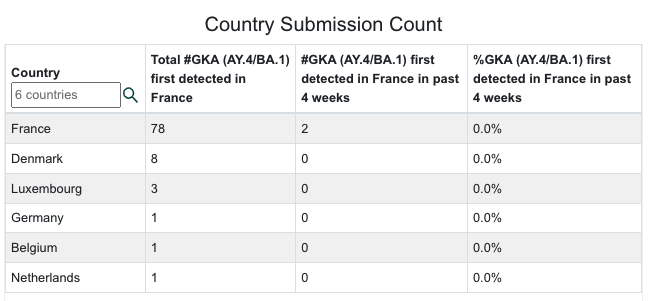
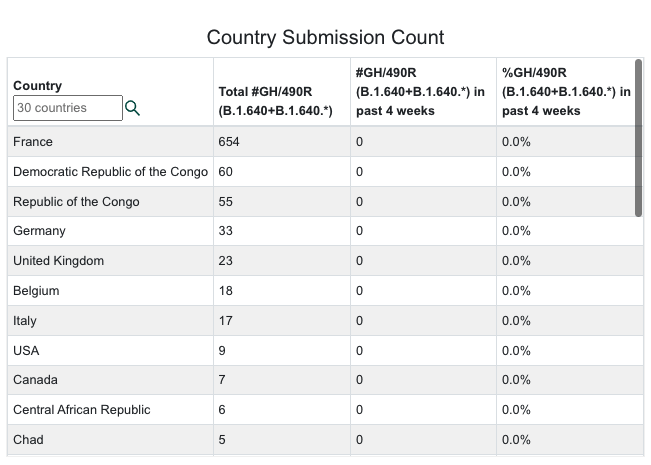
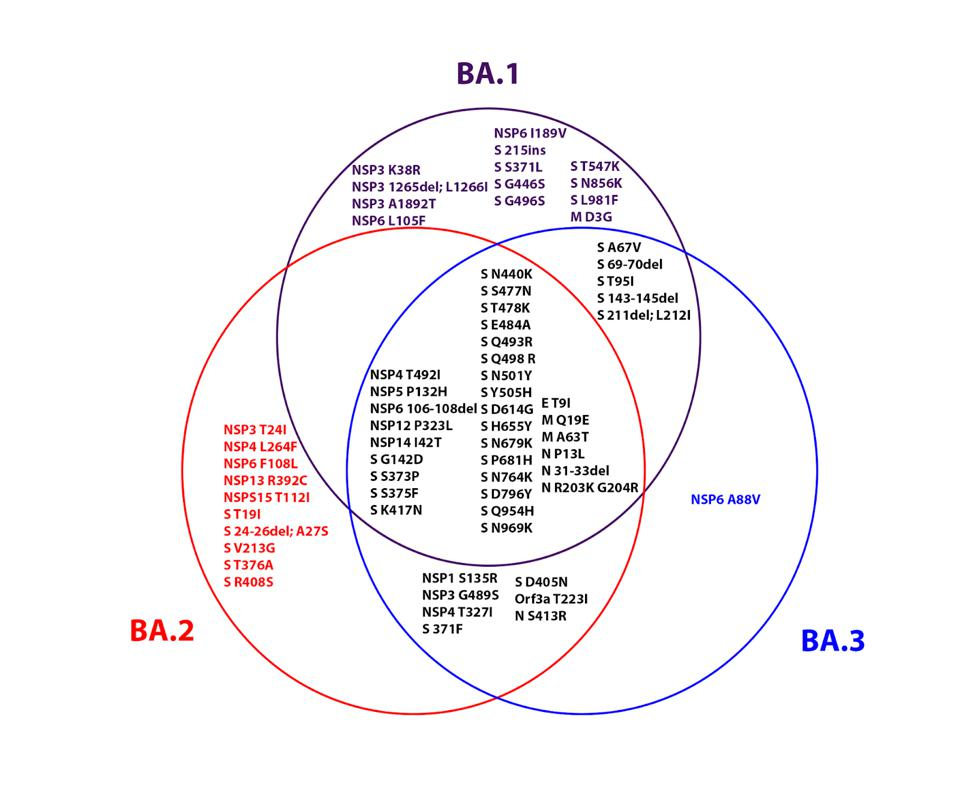
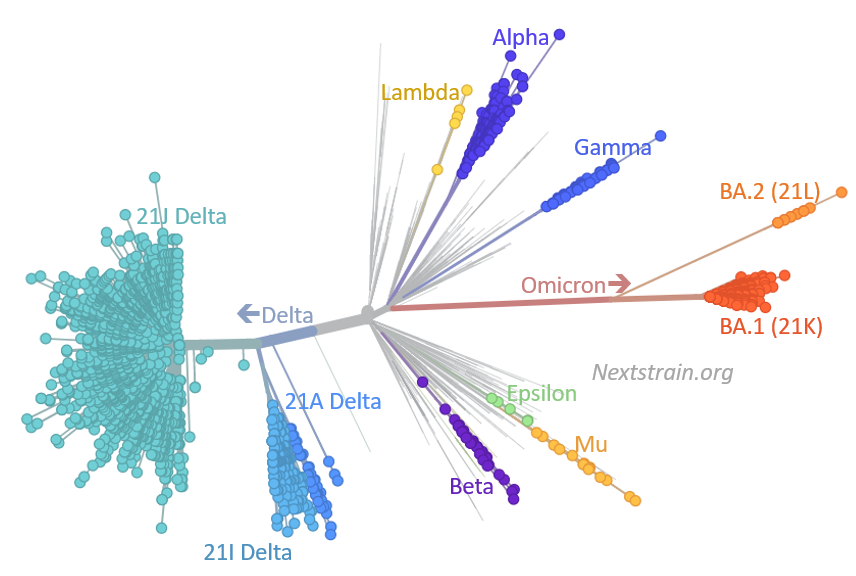
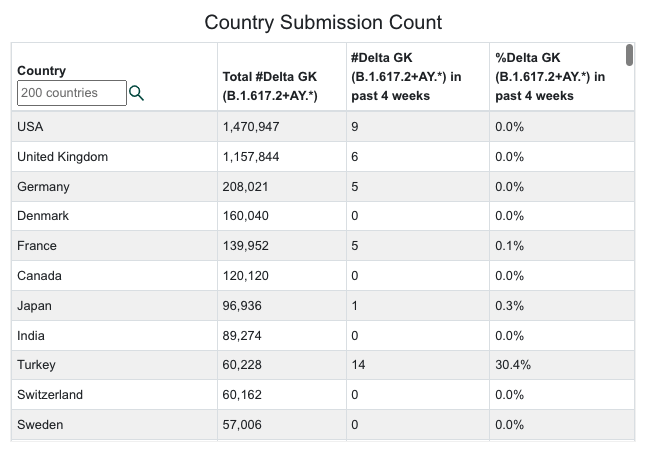
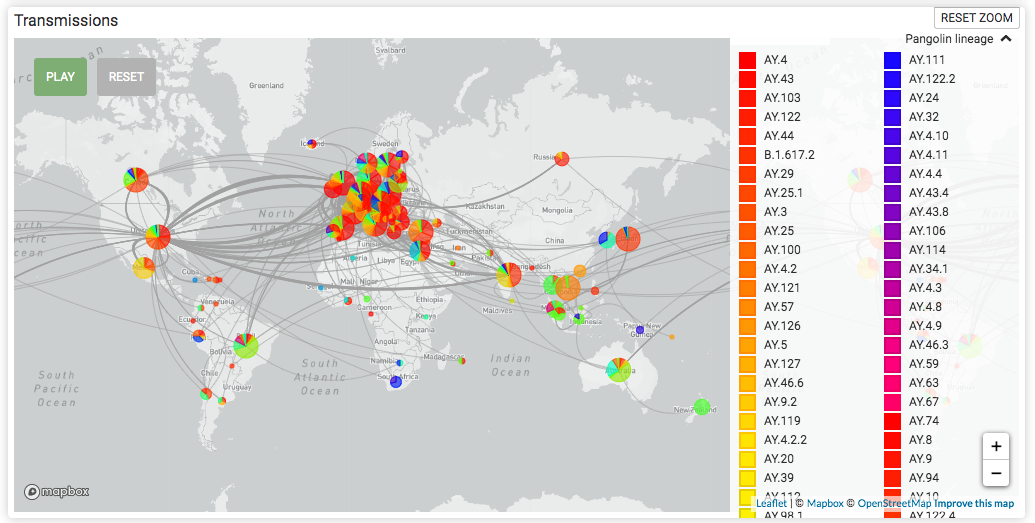
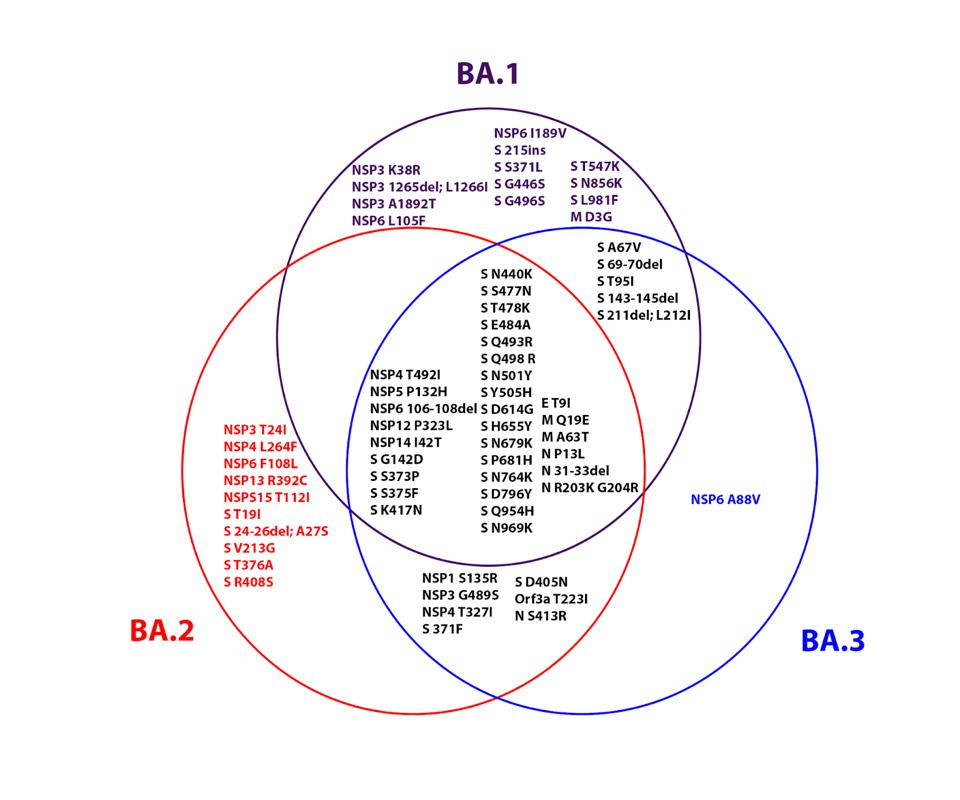
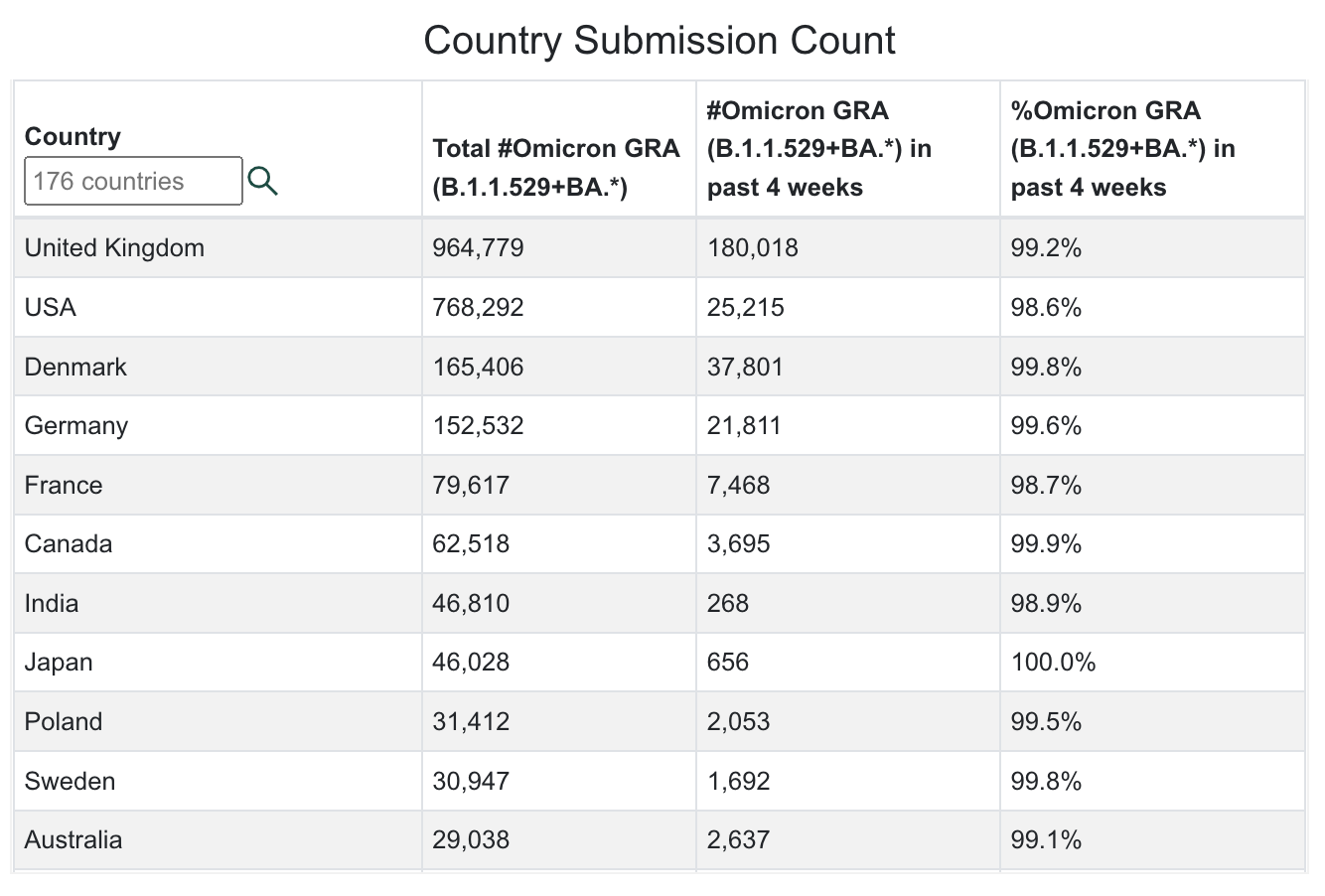
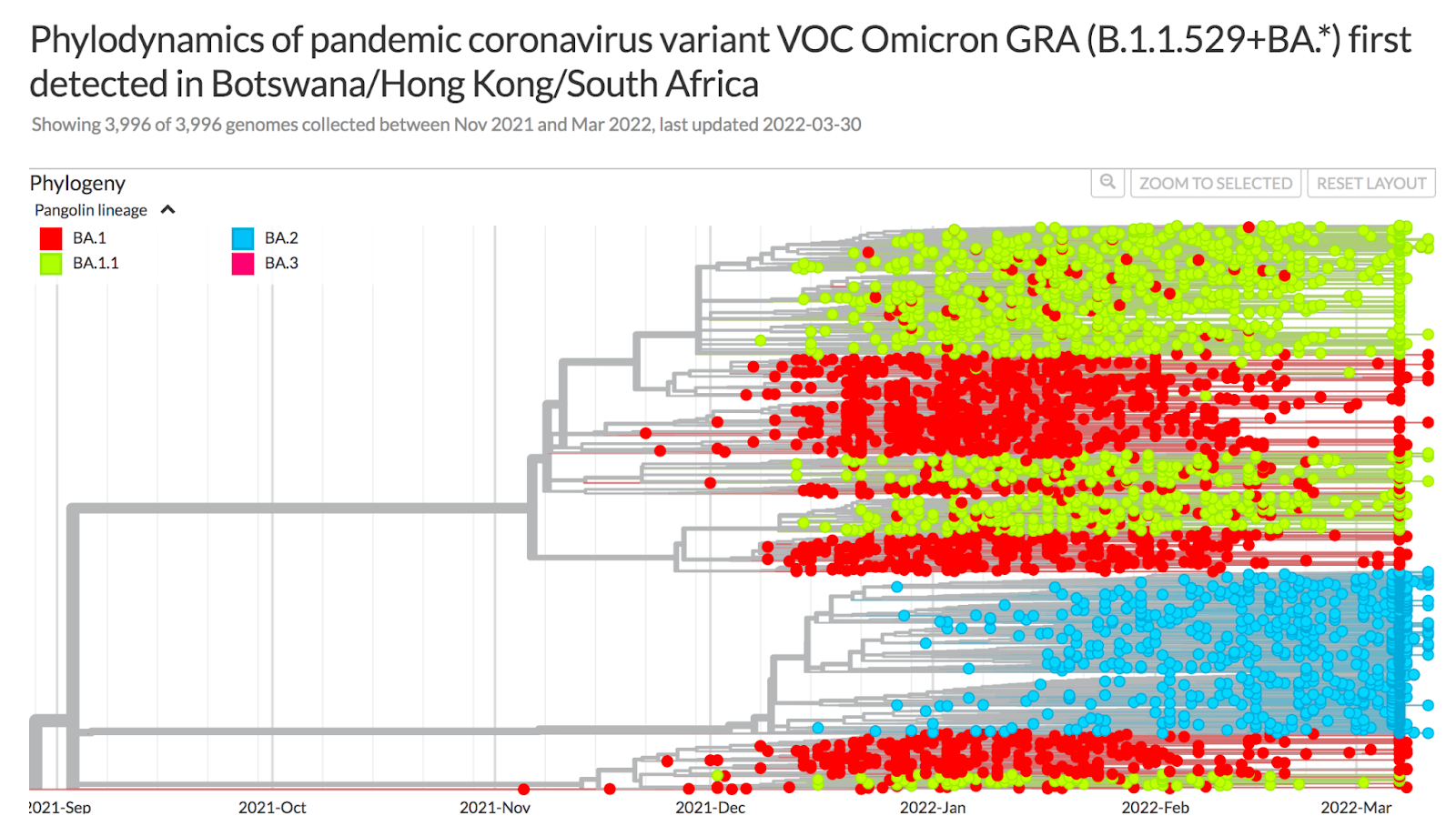
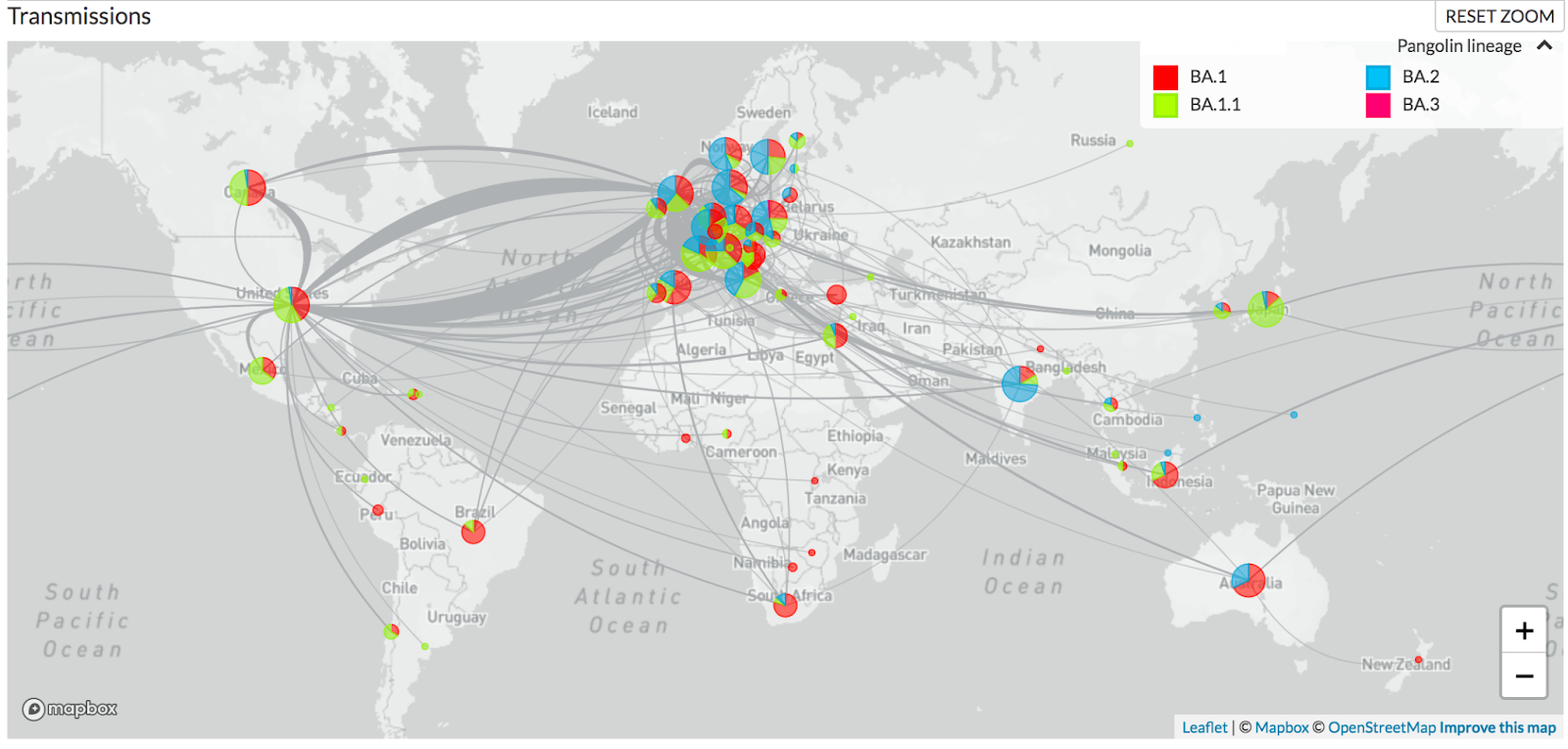
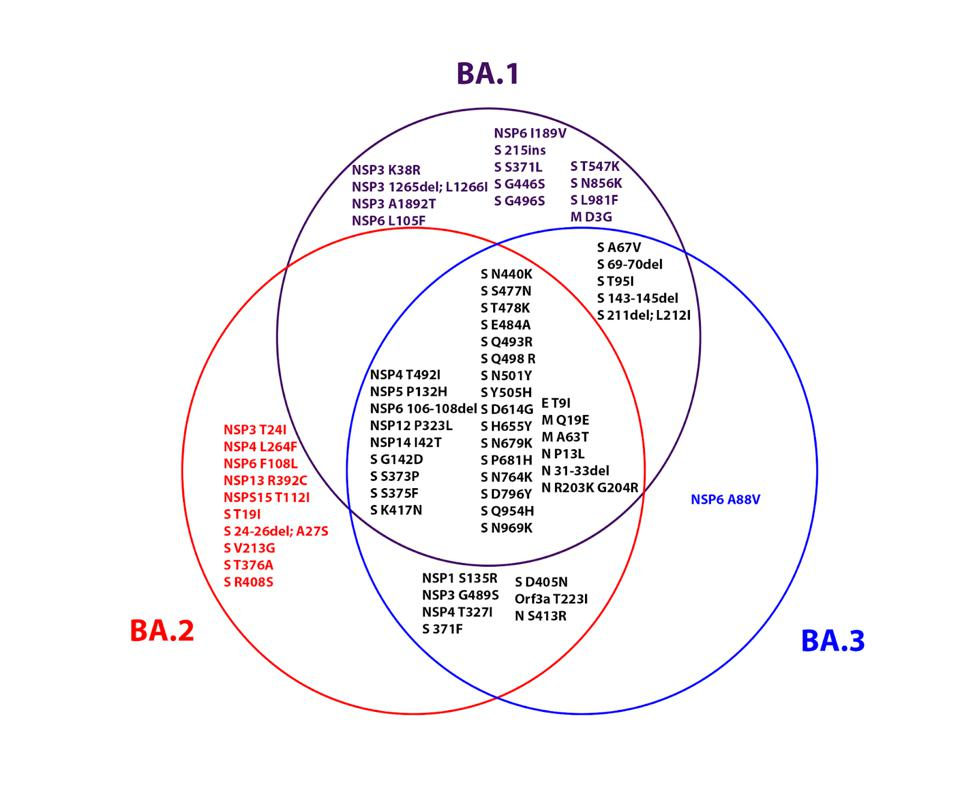
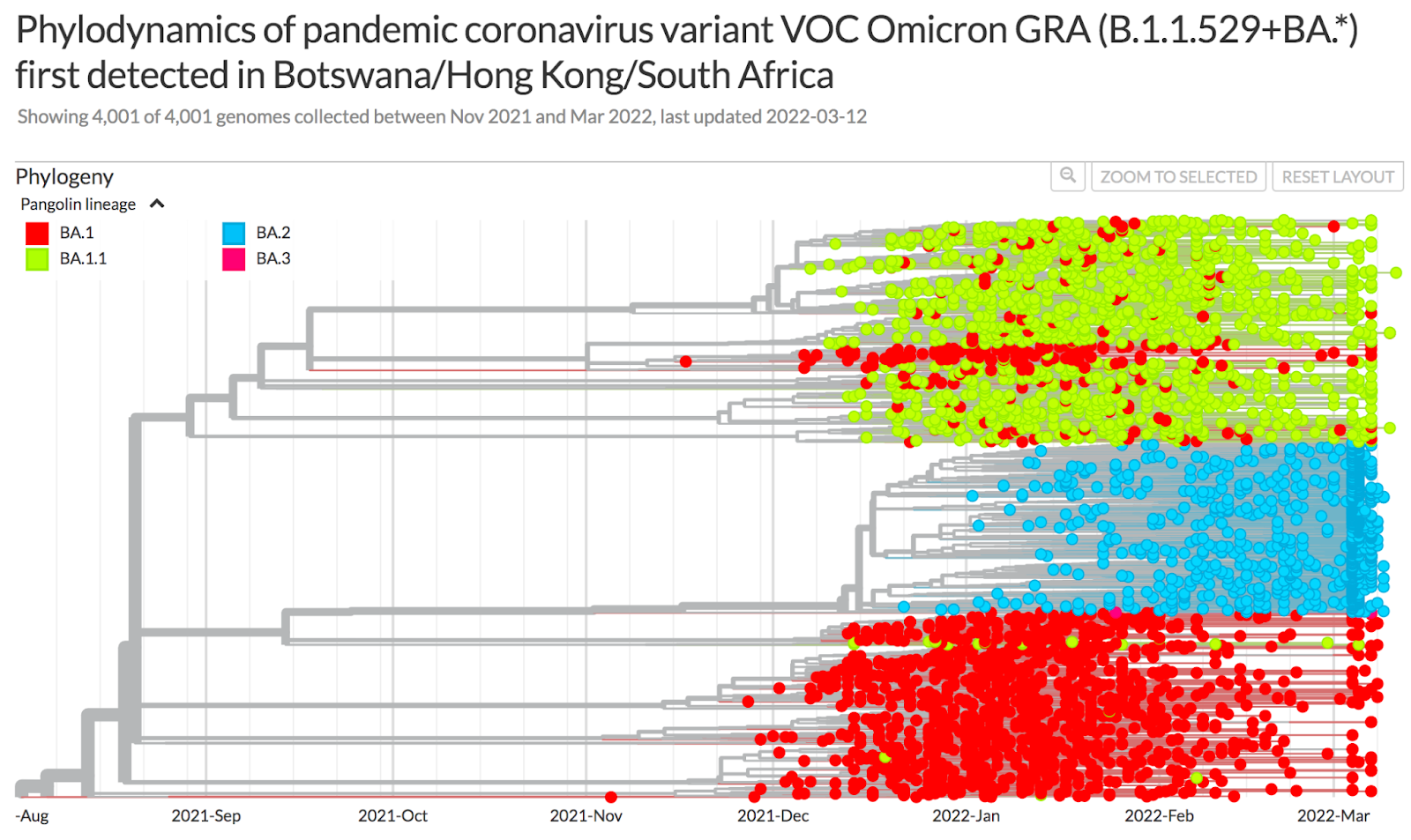
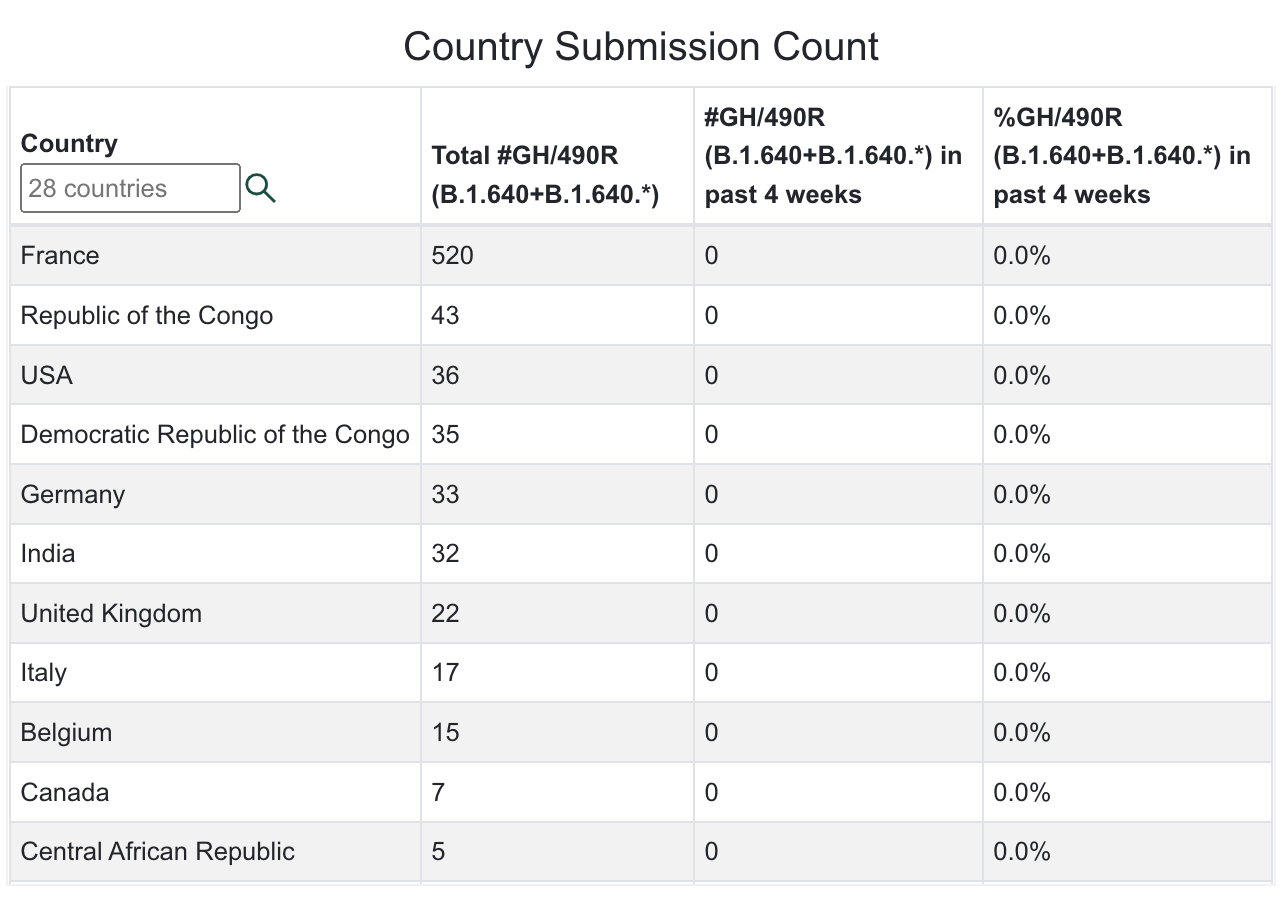
The Omicron variant has continued to mutate just like Delta. There are now 211 Omicron sub-variants (an increase of 12 in the last two weeks) that have been assigned Pango lineages, including 112 sub-lineages of BA.2 (an increase of 8 in two weeks), one sub-lineage of BA.3, 11 sub-lineages of BA.4 (an increase of 2 in two weeks), and 17 sub-lineages of BA.5 (an increase of 2 in two weeks). The BF lineage (new four weeks ago), with BF.1 first detected in England, Denmark, Spain and Scotland still has 6 sublineages. The BE lineage (also new four weeks ago), with BE.1 first detected in South Africa, Austria and England, now has 4 sublineages (one new in the past two weeks). There are also new lineages from four weeks ago: BC.1 (Japan), BC.2 (Peru),BD.1 (UK), BG.1 (Peru), BG.2 (US, Denmark, Canada), BG.3 (Peru), BG.4 (Israel).
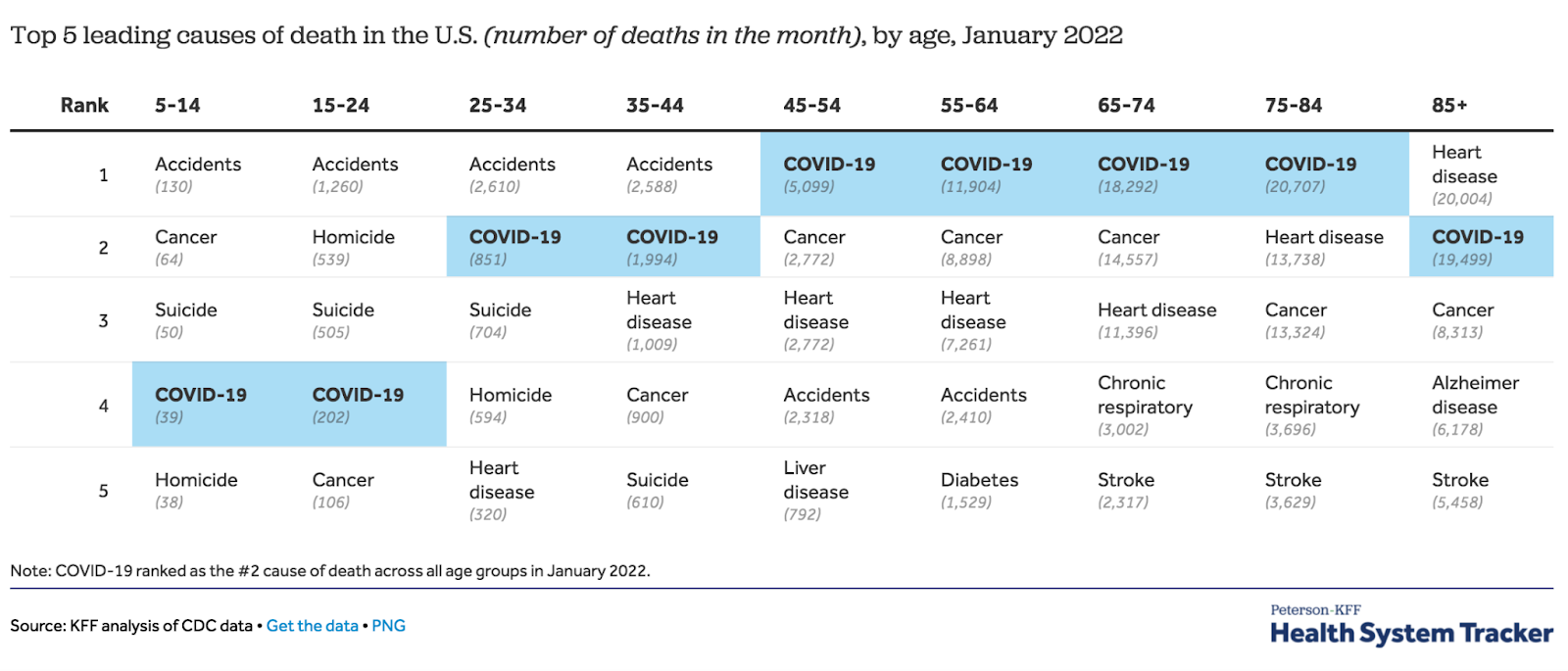
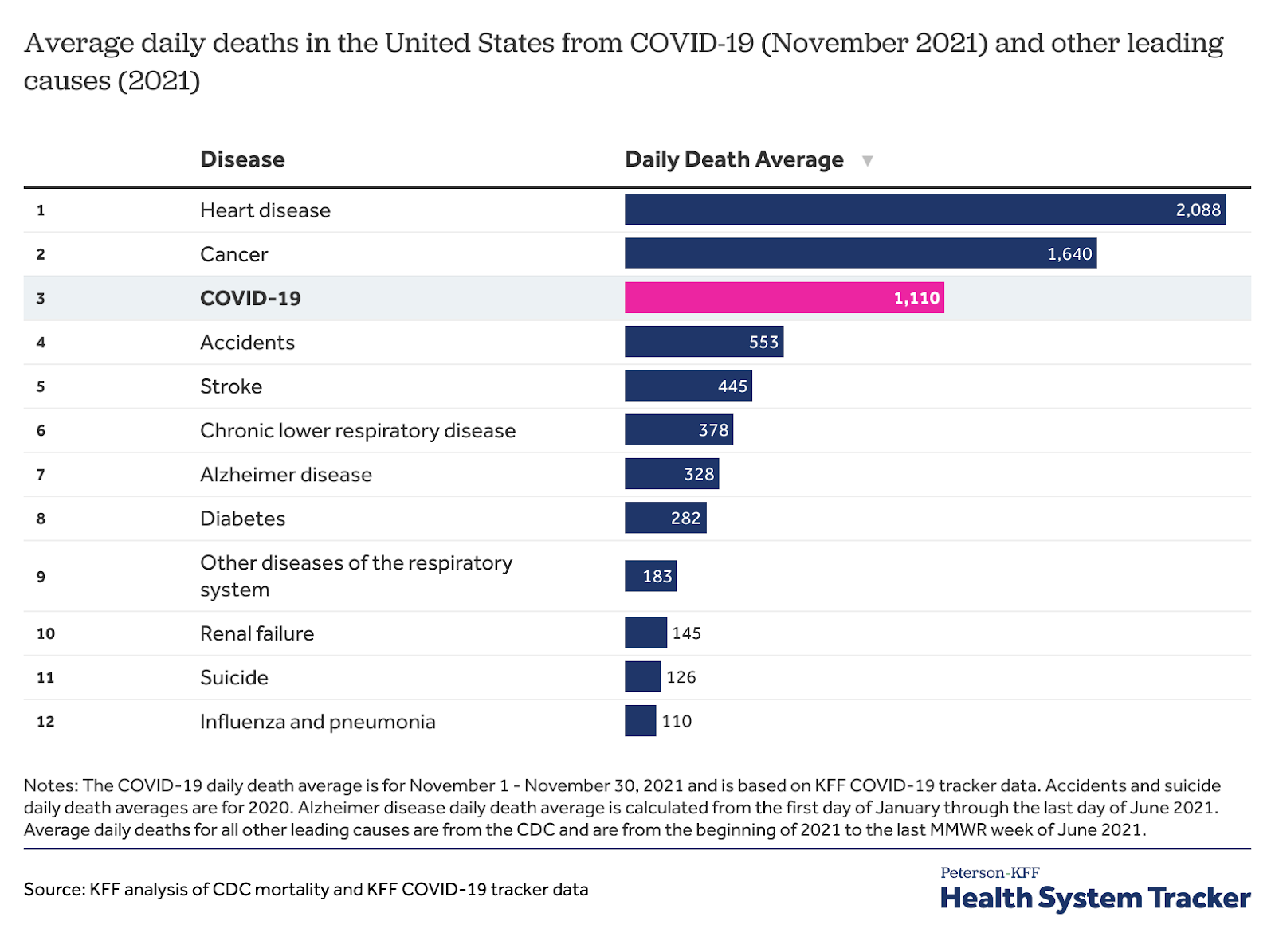
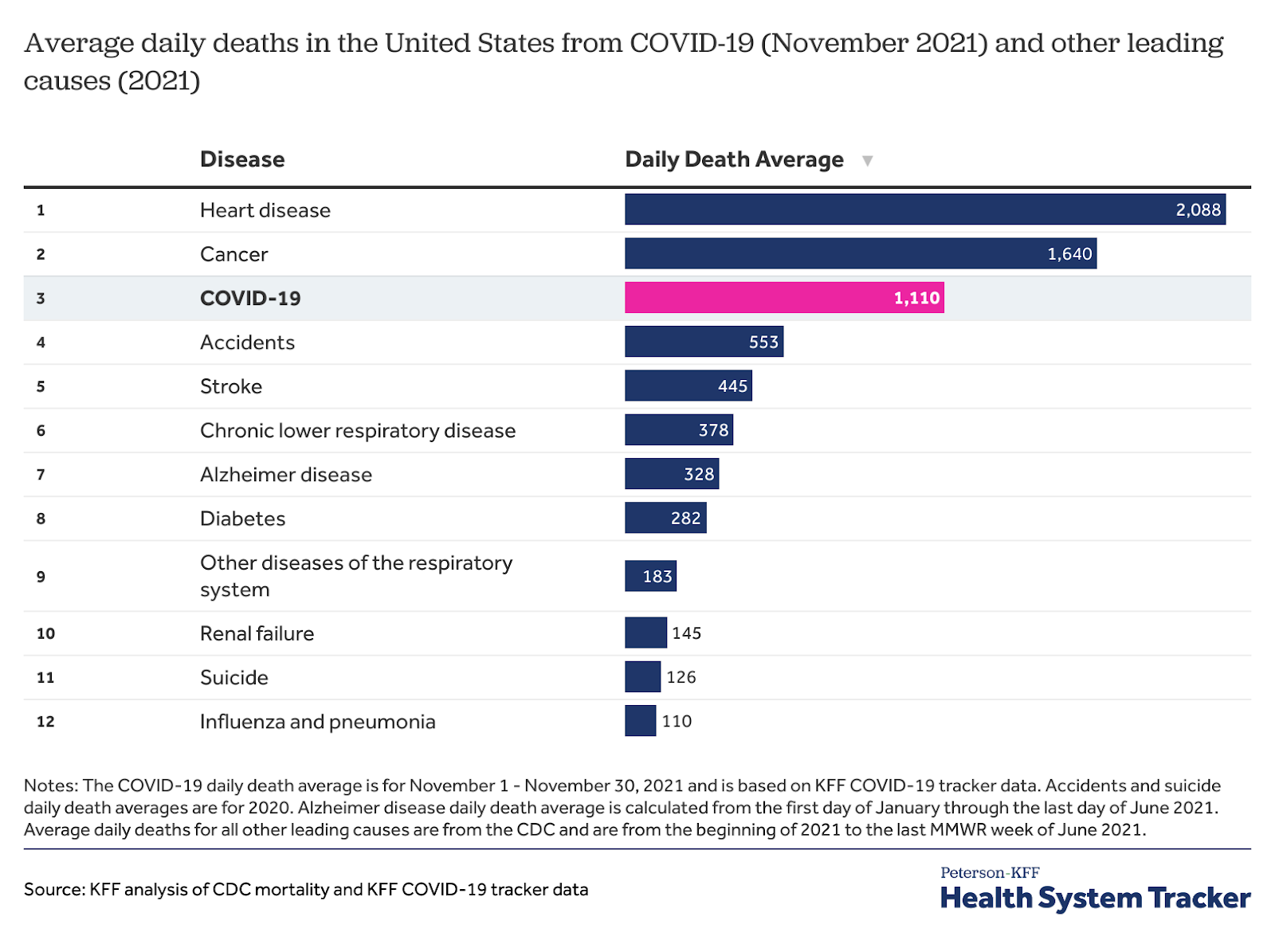
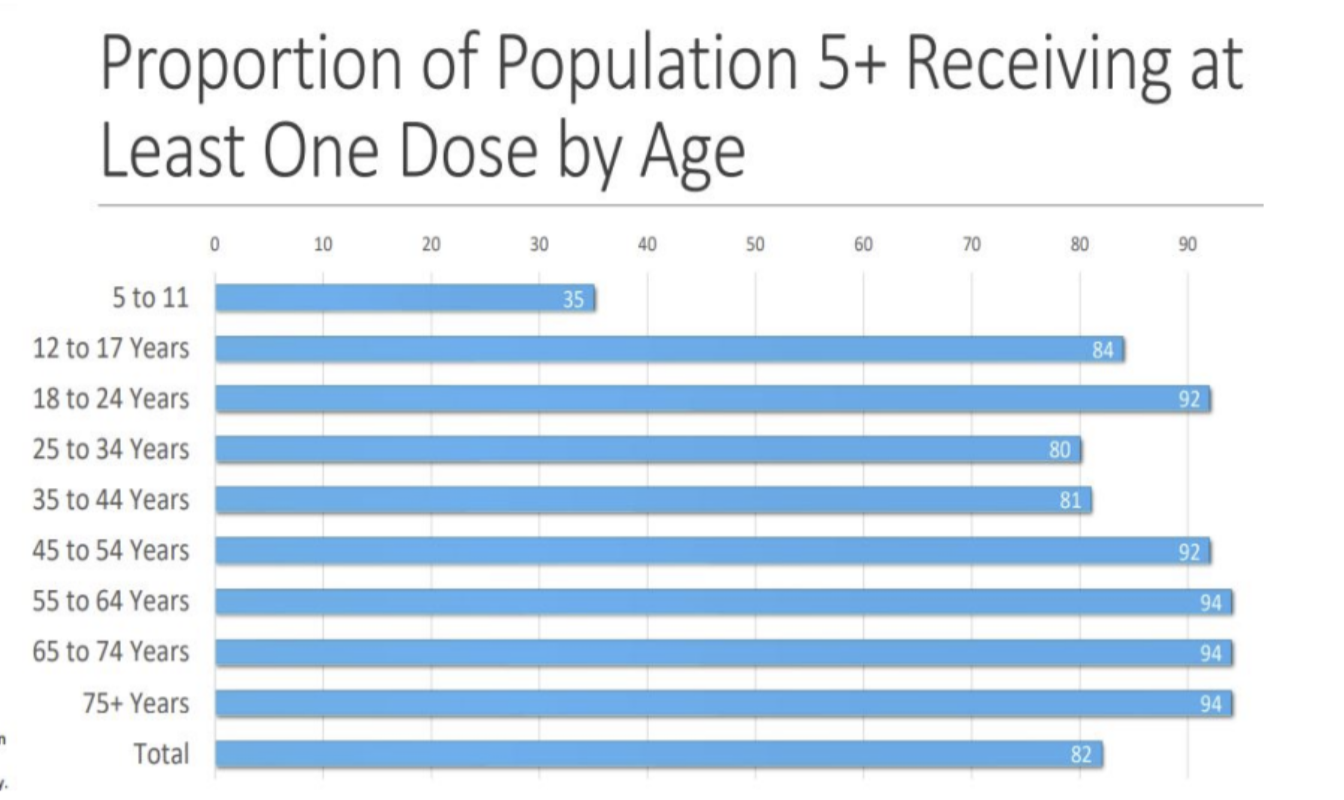
Unless people continue to wear masks and get vaccinated, including their third dose of the vaccine, we will see further spread of the Omicron variants and increase in deaths in people who are not vaccinated, those who have waning immunity, the immunocompromised population, and others with risk factors, particularly those older over the age of 64. SARS-CoV-2 is now in the top ten most common causes of death for children. Anyone over the age of 5 years can now get vaccinated in the United States at no cost. This should get done immediately.
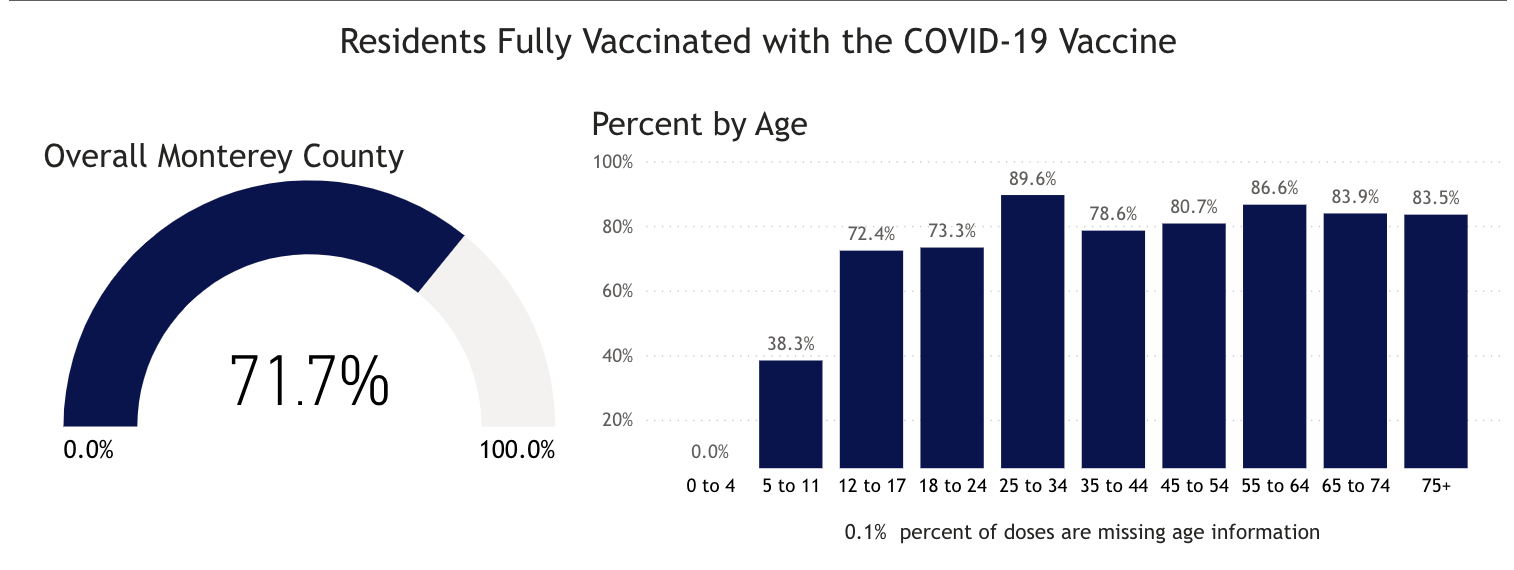
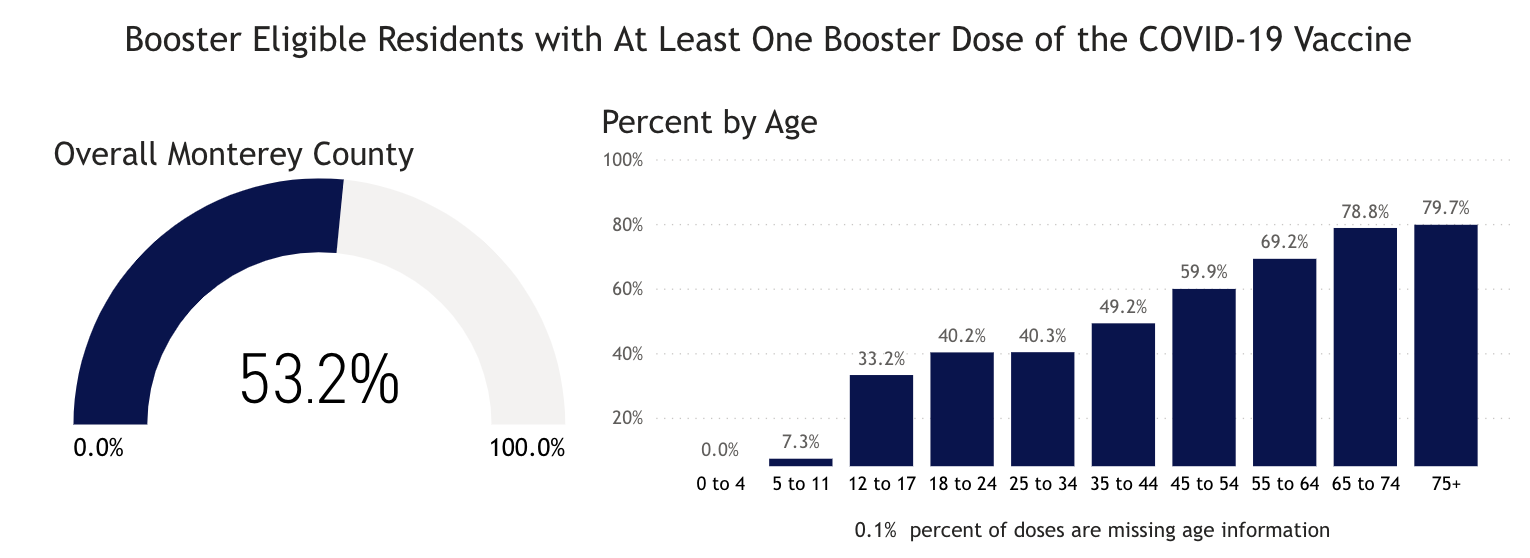
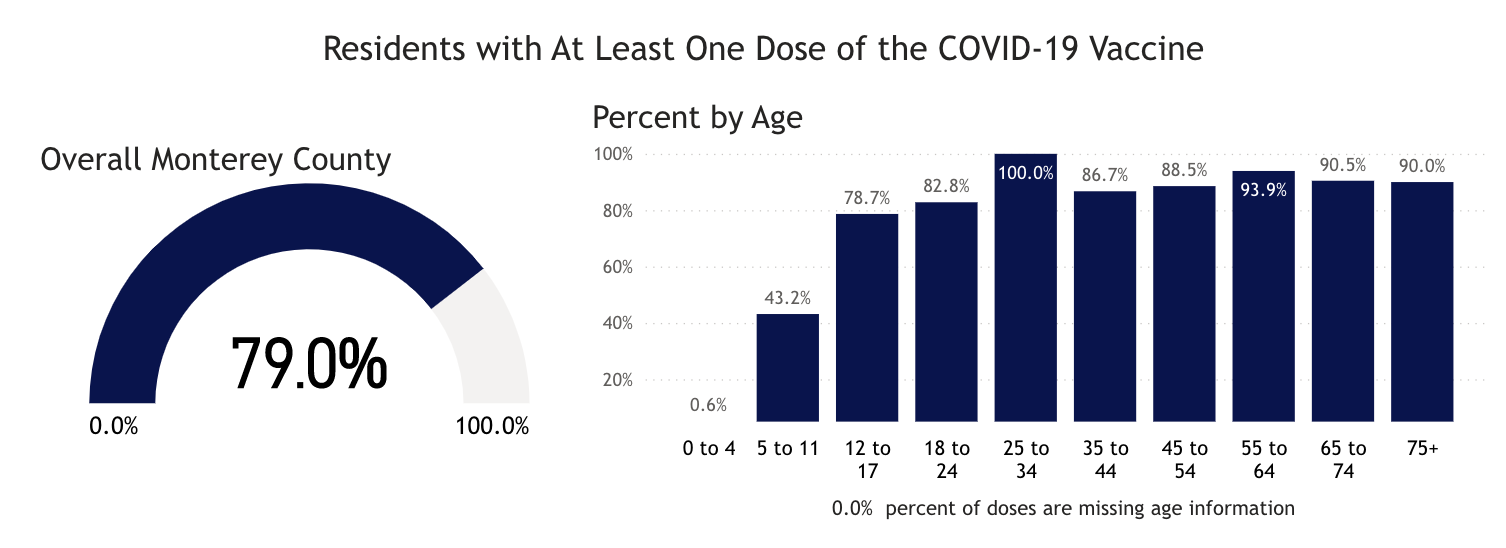
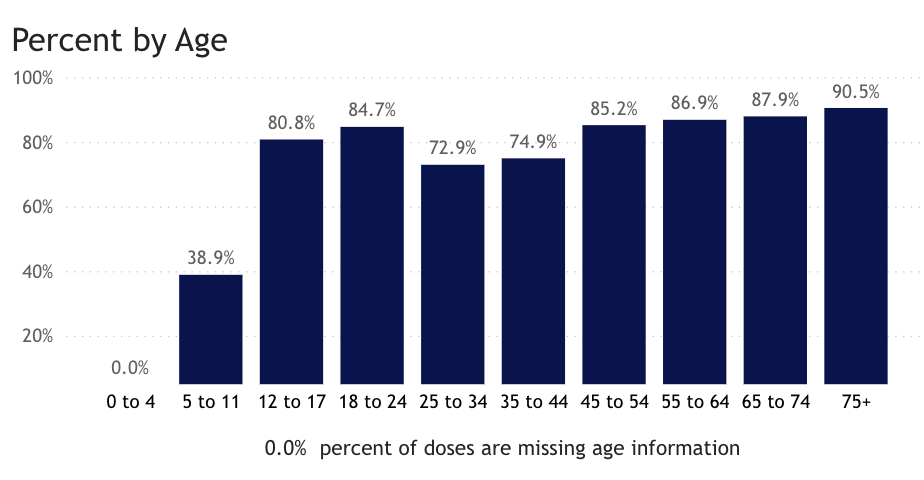
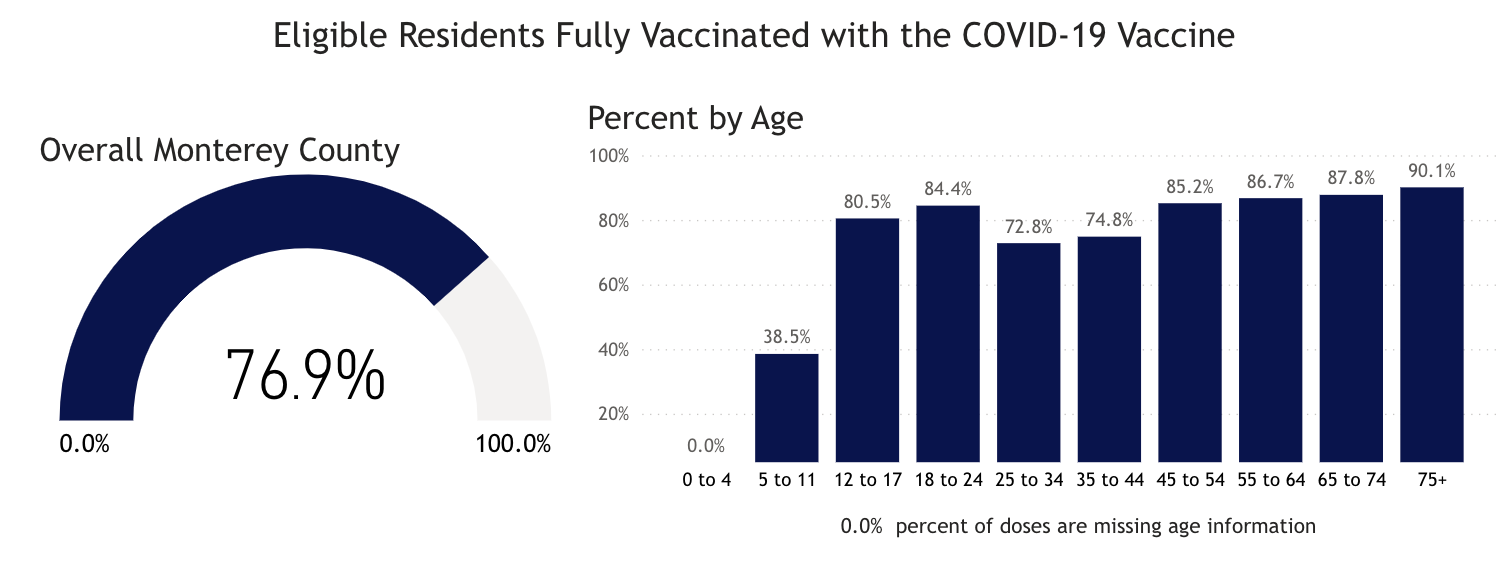
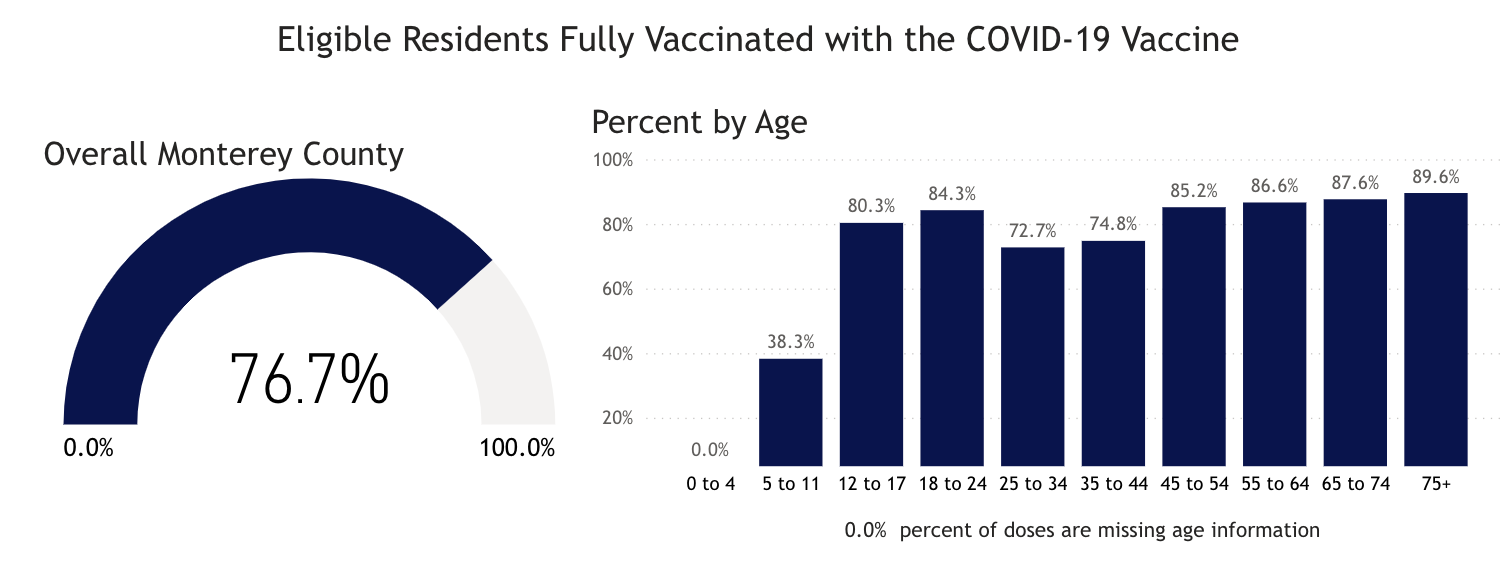
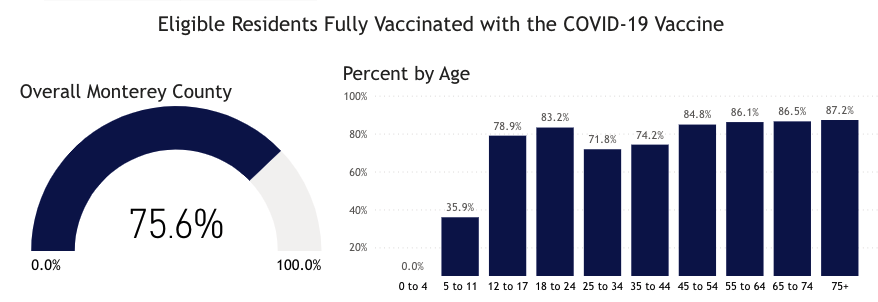
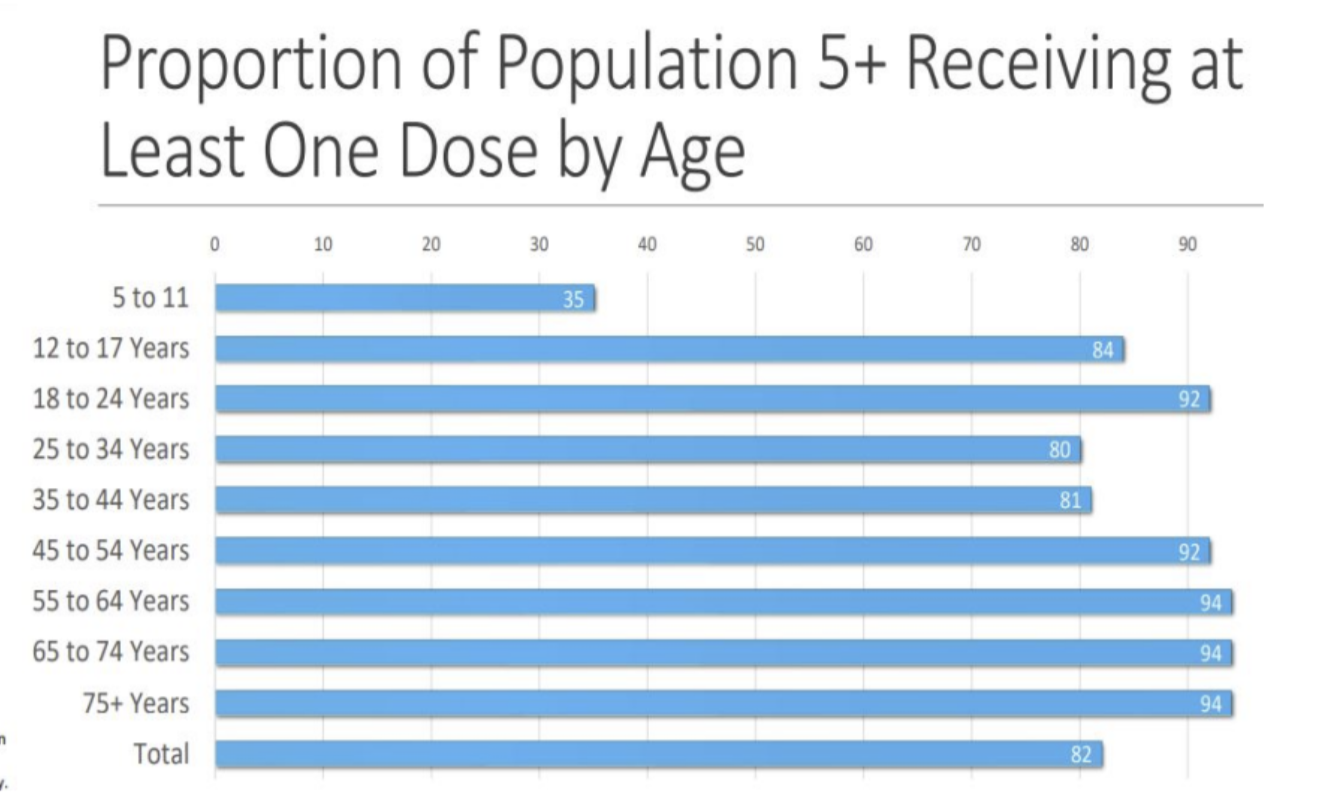
In Monterey County, as of 7/17/22, 0.0% of 0-4 year-olds and 38.3% of 5-11 year-olds have received the first two doses of vaccine, while 72.4% of 12-17 year-olds have received two doses. Only 53% of Monterey County residents have received a third dose of the vaccine. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. We would anticipate, with the start of school on August 5 and the low vaccination rates in our county, that we’ll have a marked increase in the number of infected patients. All Monterey County residents should get up to date on COVID-19 vaccinations as soon as possible.
On 7/15/22, the United States had 94,037 documented new infections. There were also 207 deaths. Twenty-one states did not report their infections, and 28 states didn’t report their deaths. In the United States the number of hospitalized patients has been increasing in many areas and was 40,650 on July 15, an increase of 20% compared to the previous 14 days. Now there are 4,180 patients who are seriously or critically ill; that number was 3,400 two weeks ago. The number of critically ill patients has increased by 780 in the last 14 days, while at least 5,412 new deaths occurred (an increase of 29 deaths per day from the previous 14 days). The number of critically ill patients has increased for the sixth time in twenty-three 14-day periods. Patients are still dying each day (average 387/day). Omicron BA.2, BA.2.12.1, BA.4, and BA.5 variants causing infections should continue to increase and critically ill patients may continue to increase. Deaths, which usually lag two to four weeks behind exponential increase in infections, are increasing now. Past infections with a BA.1 or BA.2 variant will not prevent infections with BA.2.12.1, BA.4, or BA.5.
As of 7/15/22, we have had 1,048,693 deaths and 91,170,571 SARS-CoV-2 infections in the United States. We have had 1,663,488 new infections in the last 14 days. We are adding an average of 831,744 infections every seven days. For the pandemic in the United States we are averaging one death for every 86.94 infections or over 11,503 deaths for each one million infections. As of 7/15/22, thirty-eight states have had greater than 500,000 total infections, and 37 states have had greater than 5,000 total deaths. Seventeen states (Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York, and California) have had greater than 70,000 deaths. California and Texas have each had greater than 89,000 deaths with California having 93,017 deaths (20th most deaths in the world).
As of 7/1/22, in the United States, 26.72% of the population has had a documented SARS-CoV-2 infection. In the last 18 months, 23.97% of our country became infected with SARS-CoV-2. On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. In the last 18 months, there were 788,562 new deaths from SARS-CoV-2. For fifteen of those months, vaccines have been available to all adults. During these fifteen months, 477,596 people have died of SARS-CoV-2 infections. Most of the hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 7/15/22, California was ranked 32th in the USA in infection percentage at 26.27%. In California, 22.3% of people were infected in the last 18 months. As of 7/15/22, 38 states have had greater than 25% of their population infected.
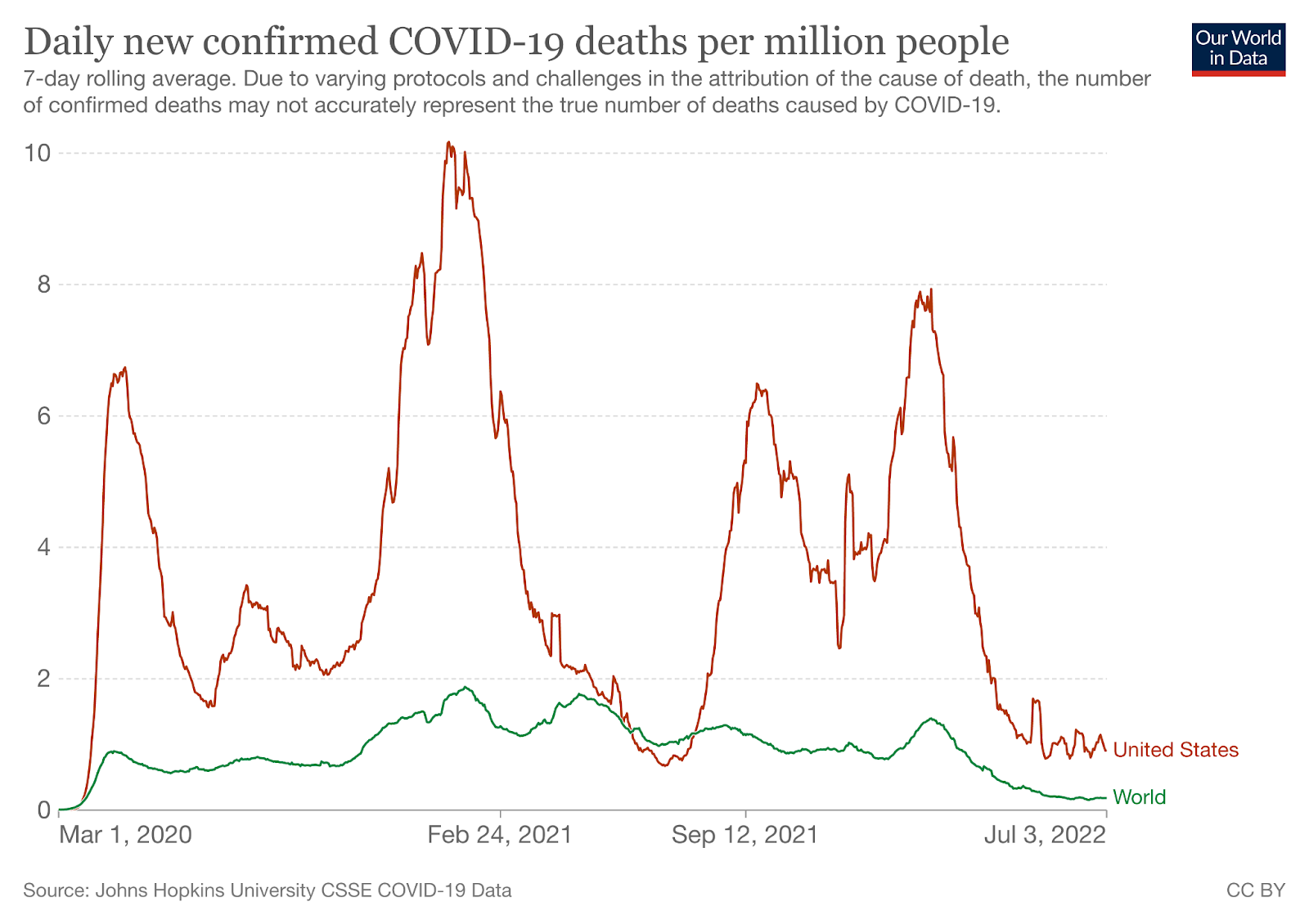
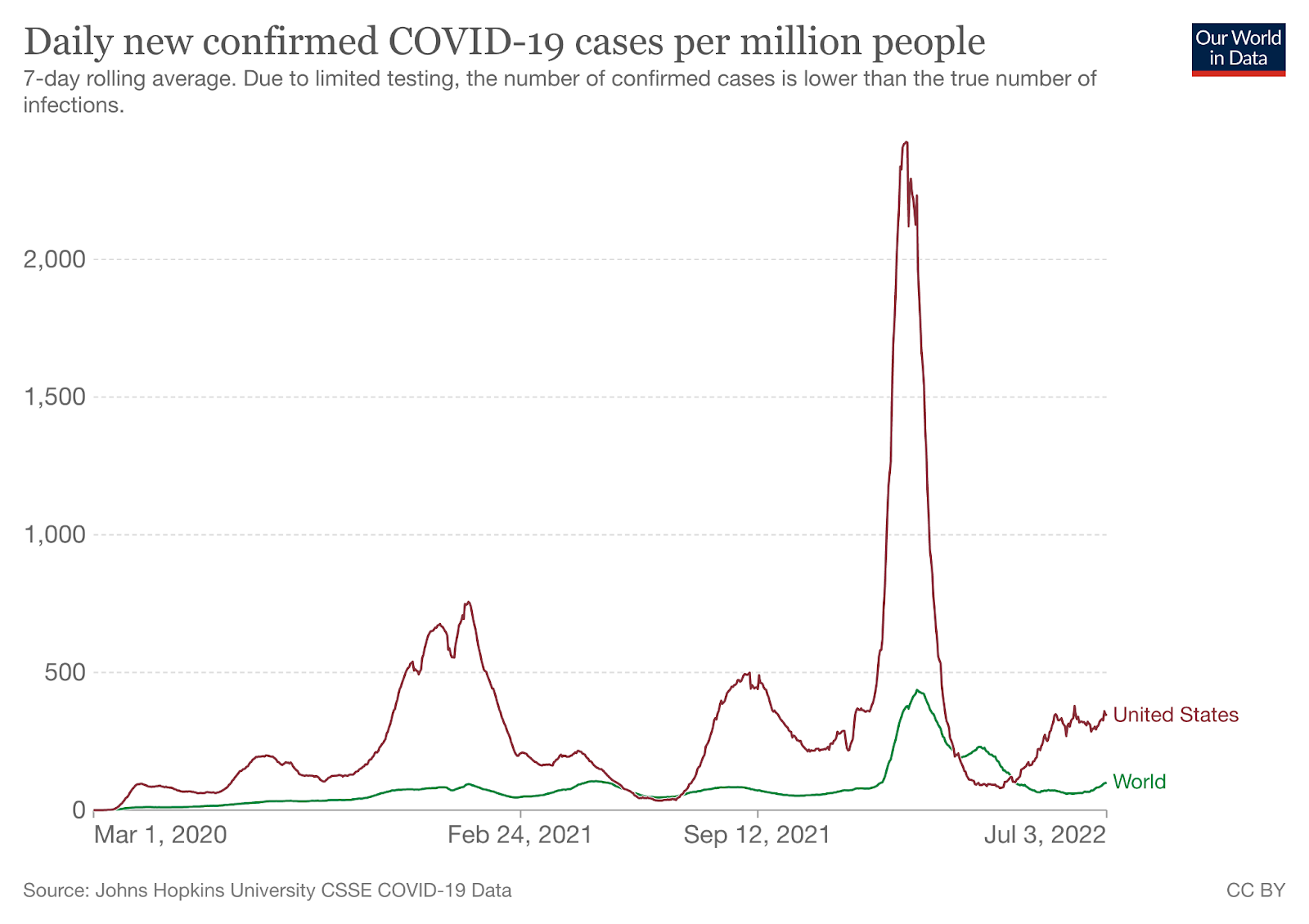
Worldwide, average deaths per day are 1,846 for the last 14 days. The United States has 20.96% (387 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 910,374. The United States accounts for 13.05% of those infections (or 118,821 infections per day).
Watching World Data
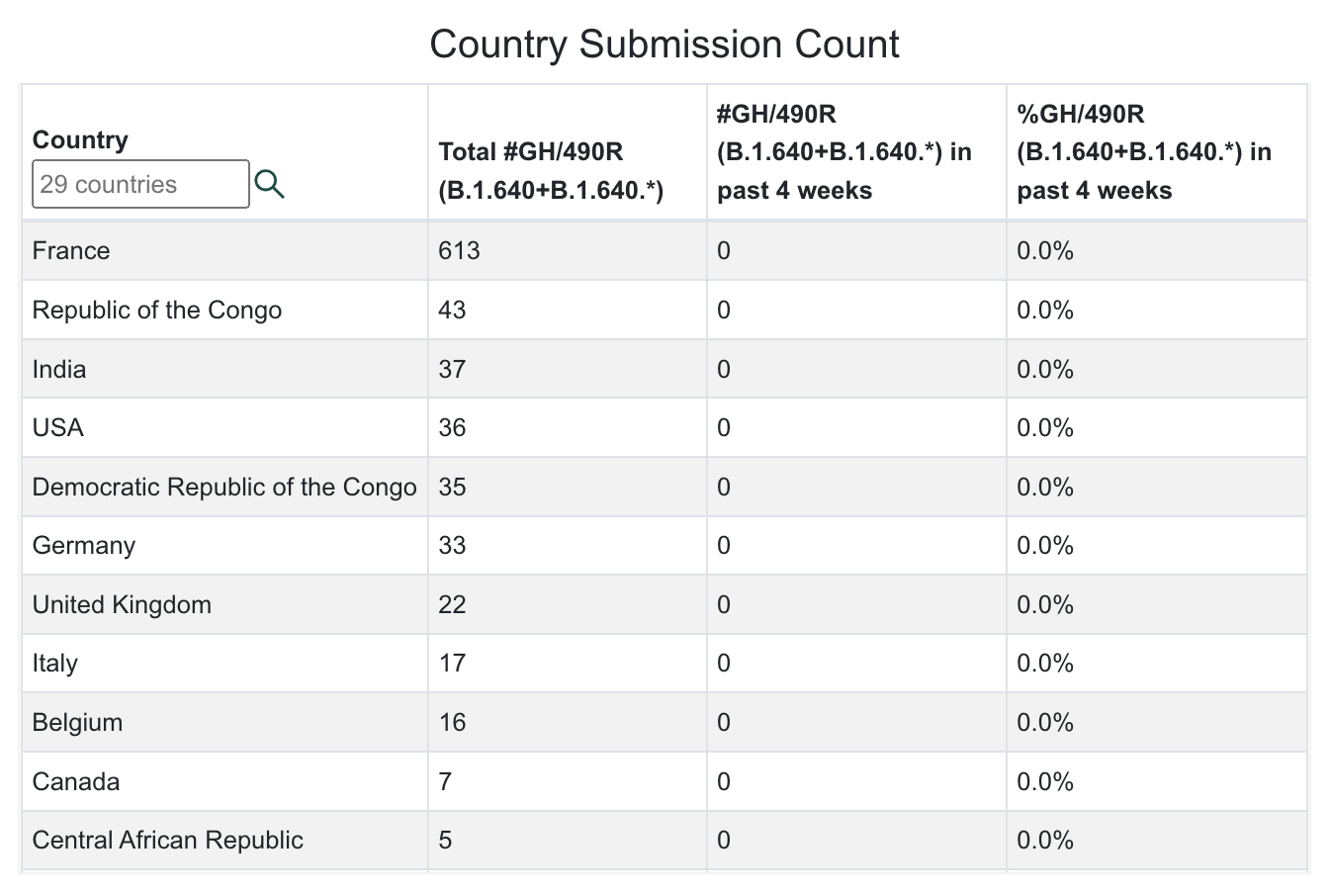
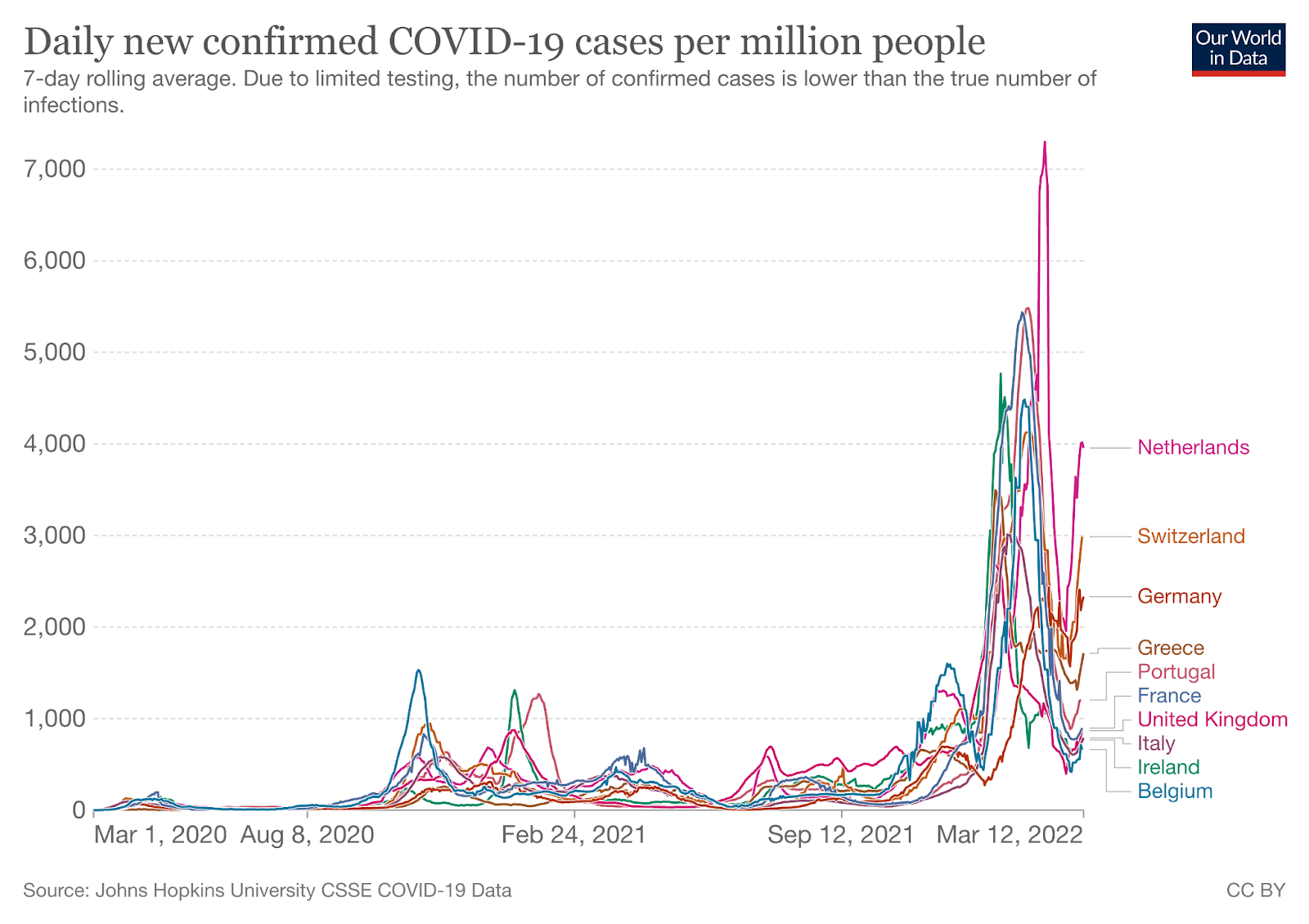
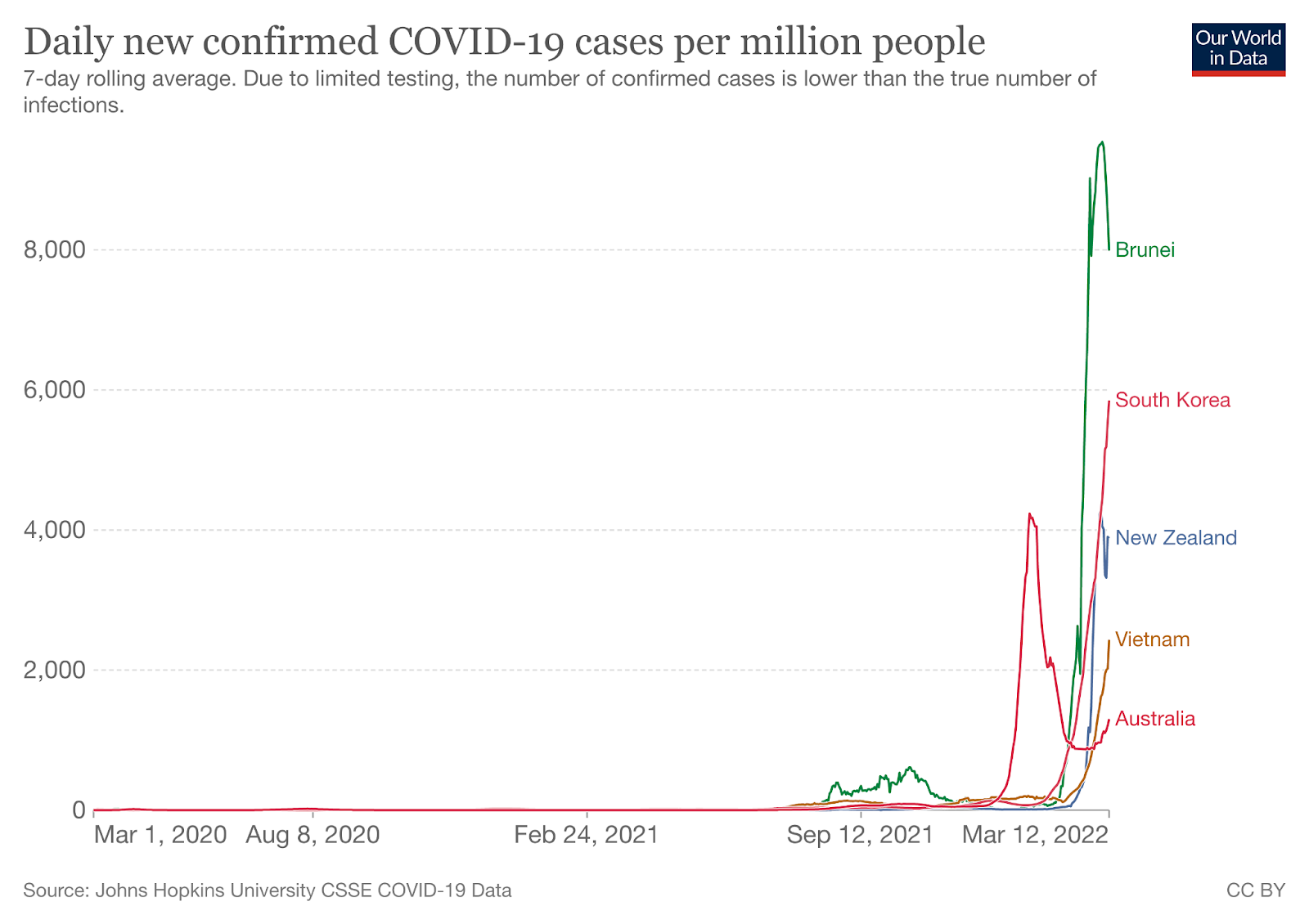
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
| Location | Total Infections as of 7/15/22 | New Infections on 7/15/22 | Total Deaths | New Deaths on 7/15/22 | % of Pop.Infected | SARS-CoV-2 Isolates Currently Known in Location | National/ State Mask Mandate | Currently in Lockdown |
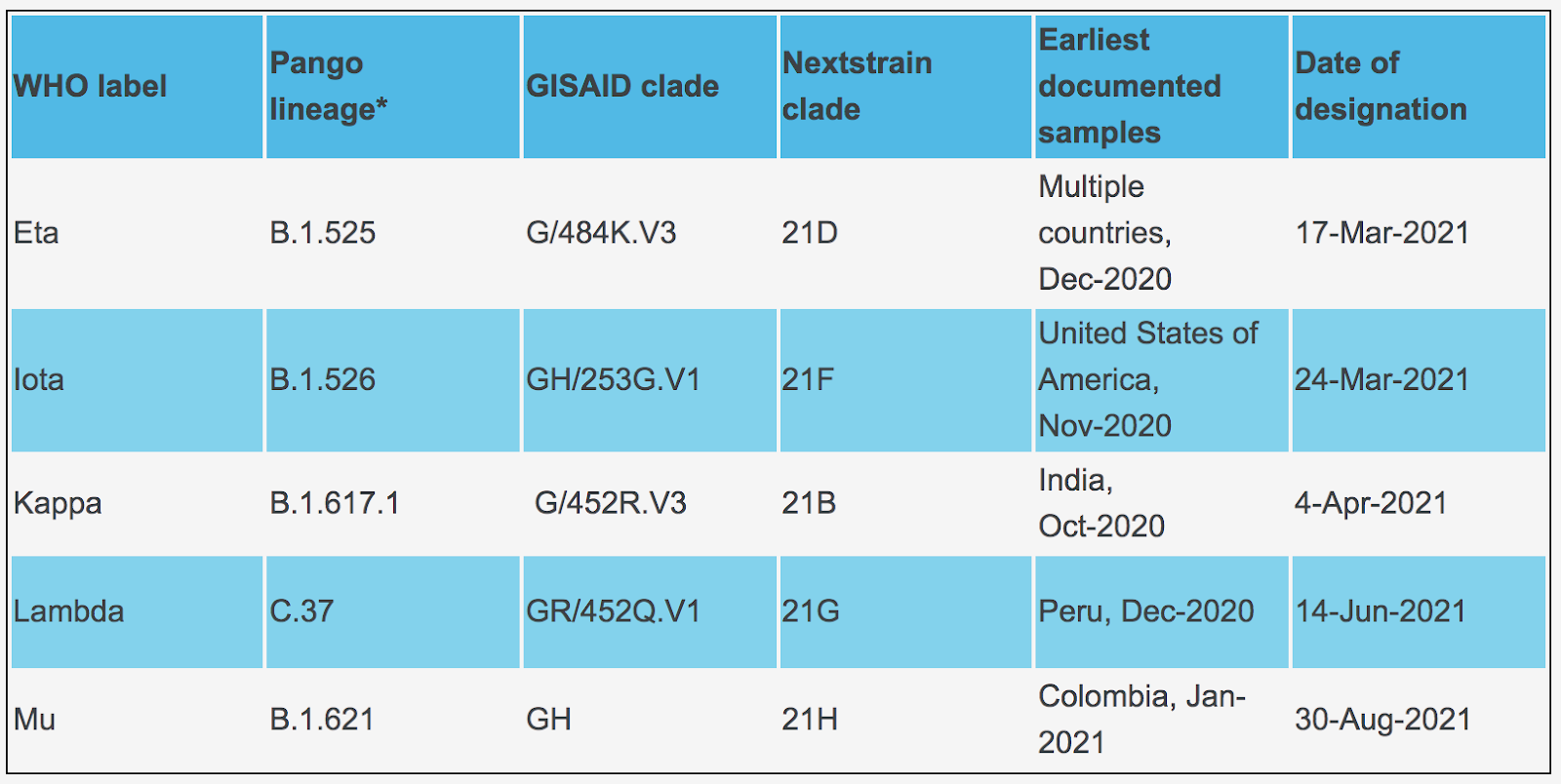
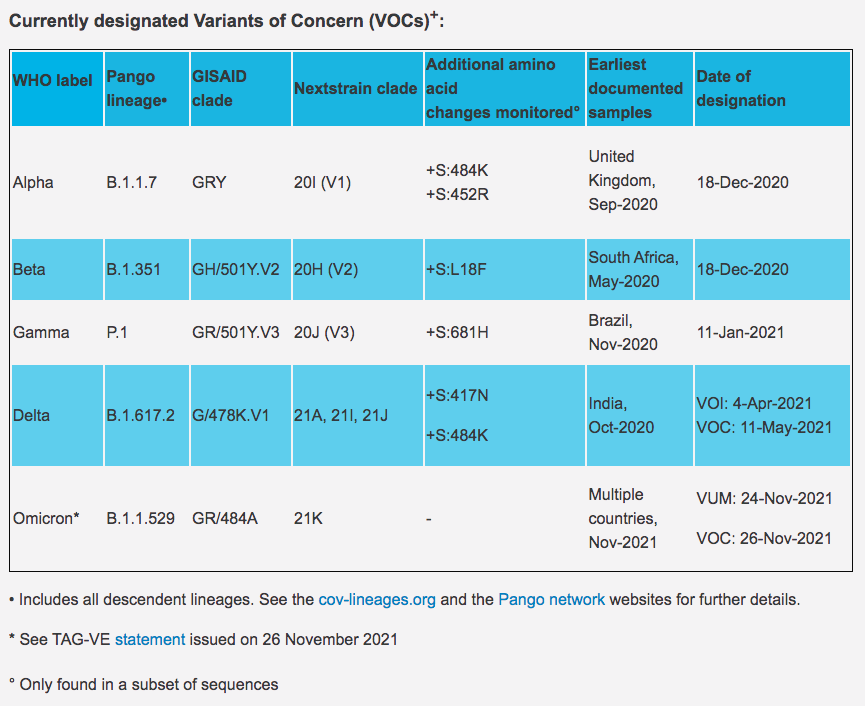
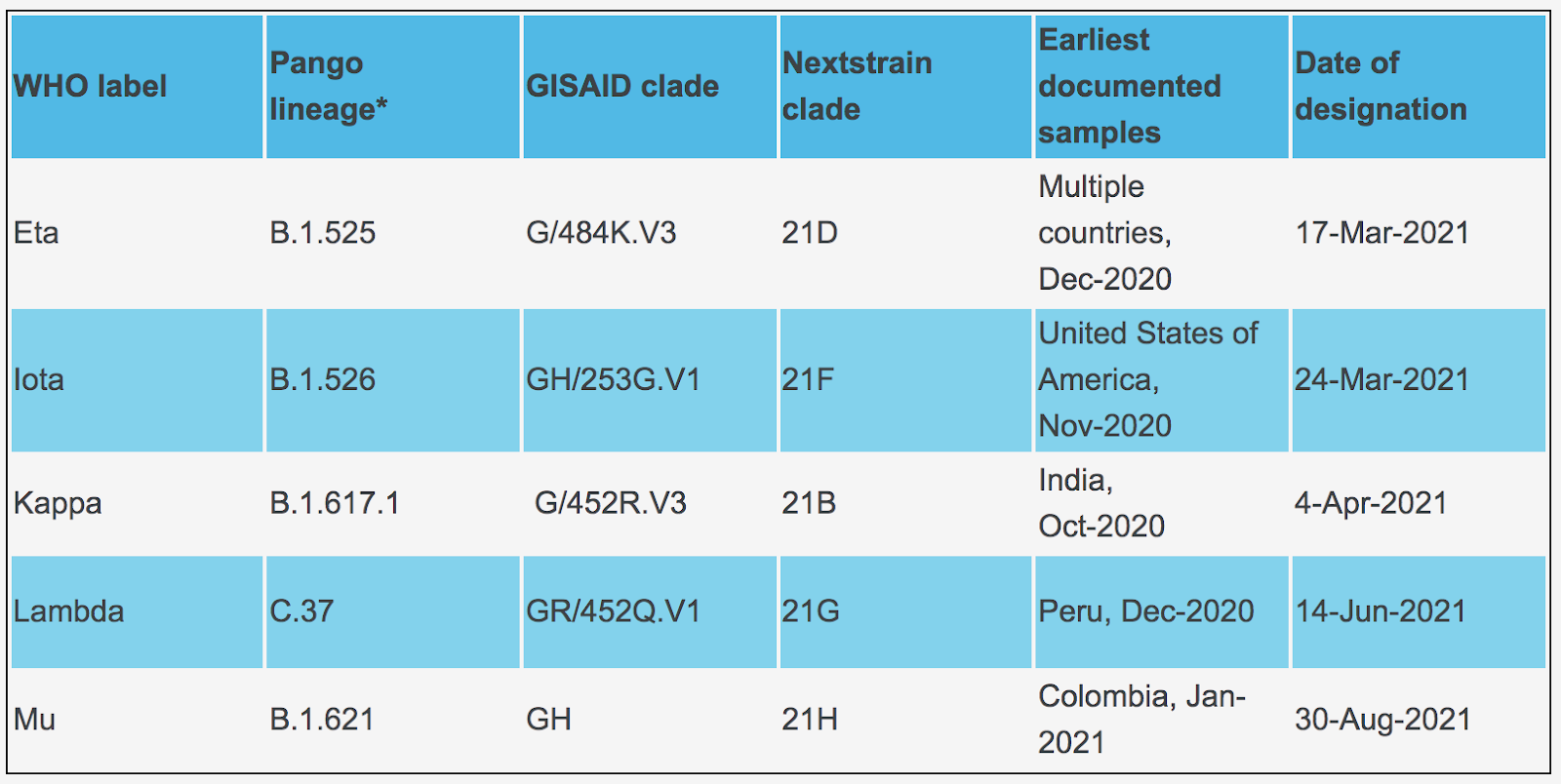
| World | 566,343,288(12,745,232 new infections in 14 days). | 903,272 | 6,385,820(25,848 new deaths in last 14 days) | 1,737 | 7.26% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
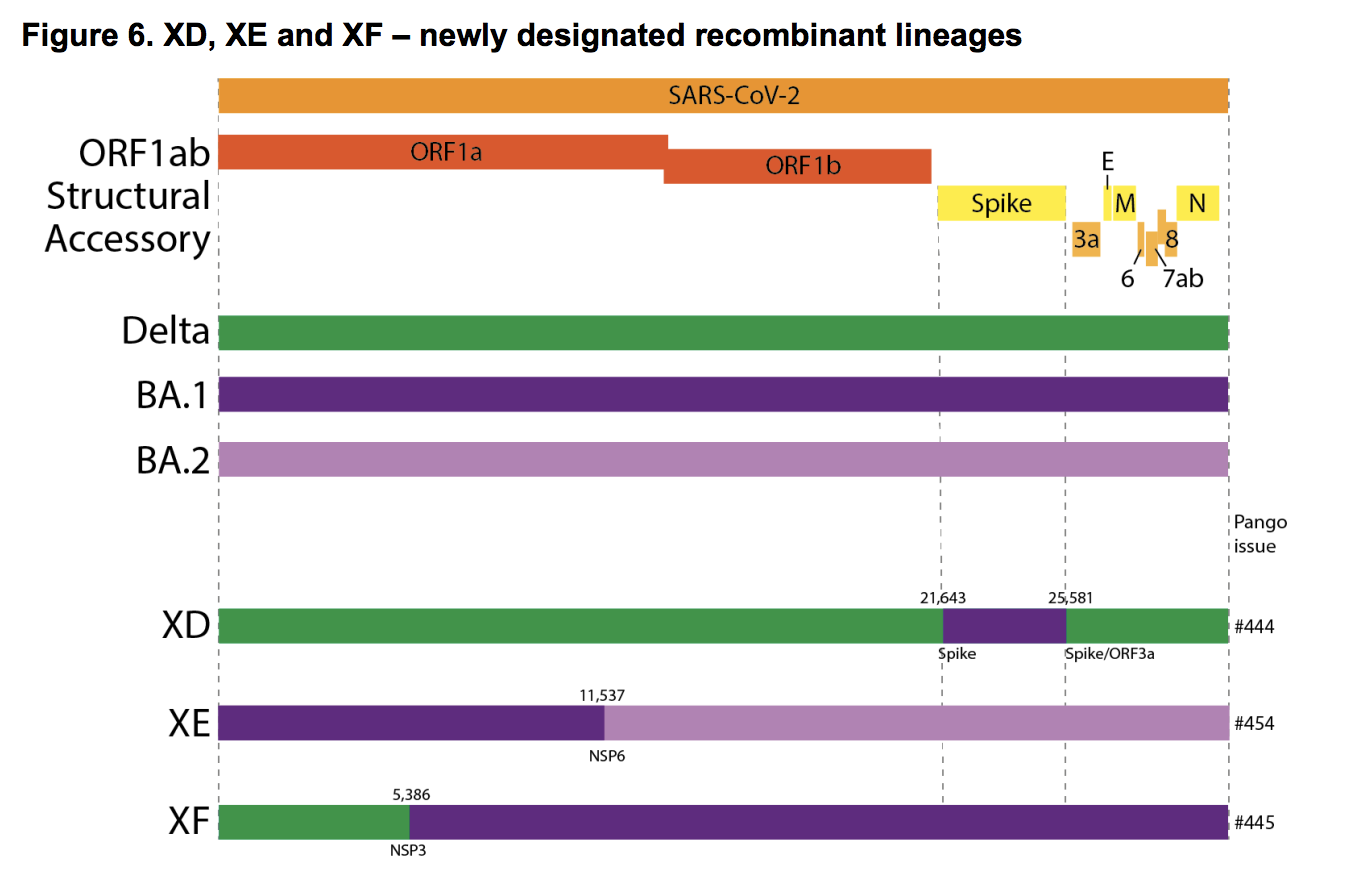
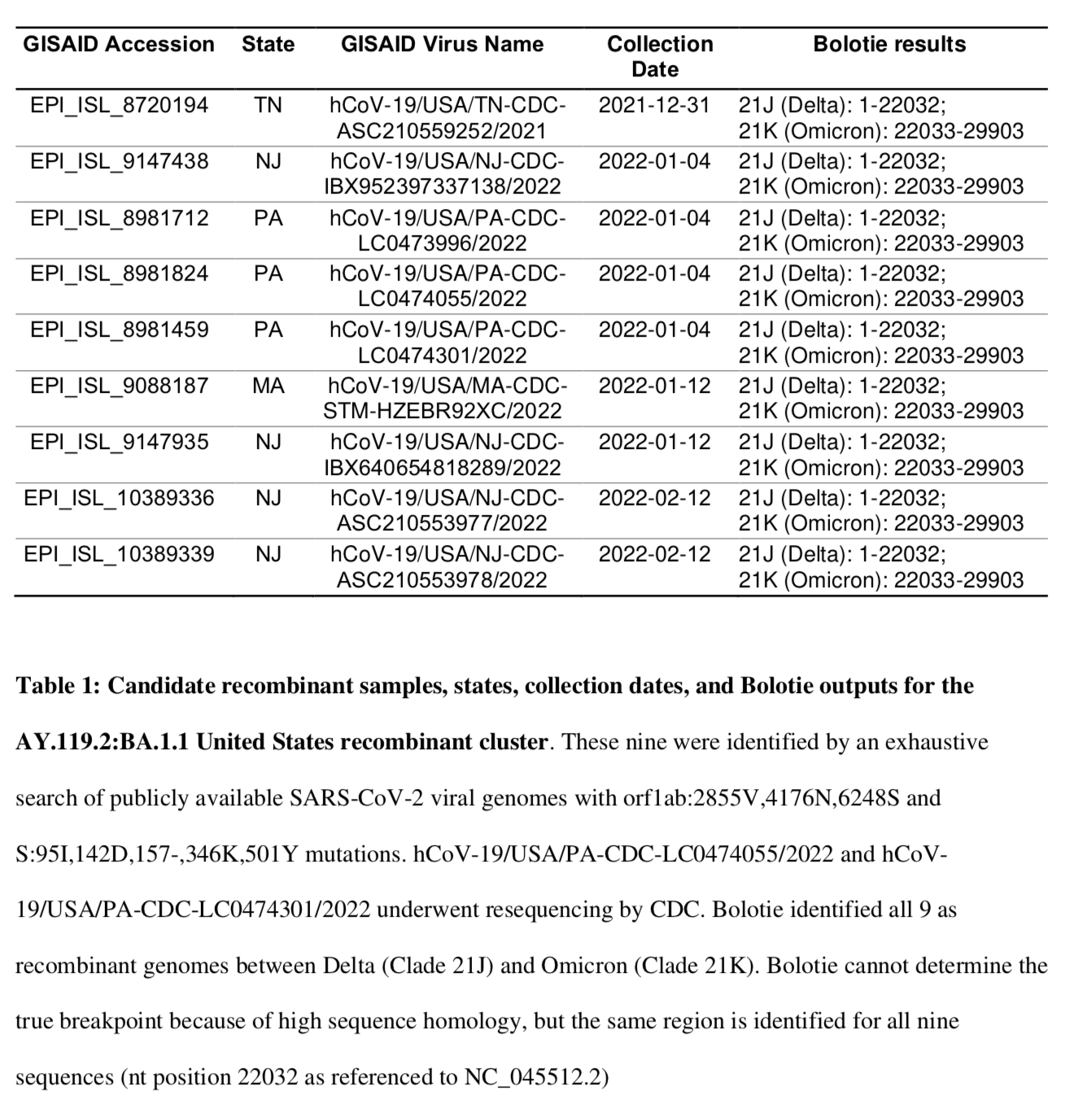
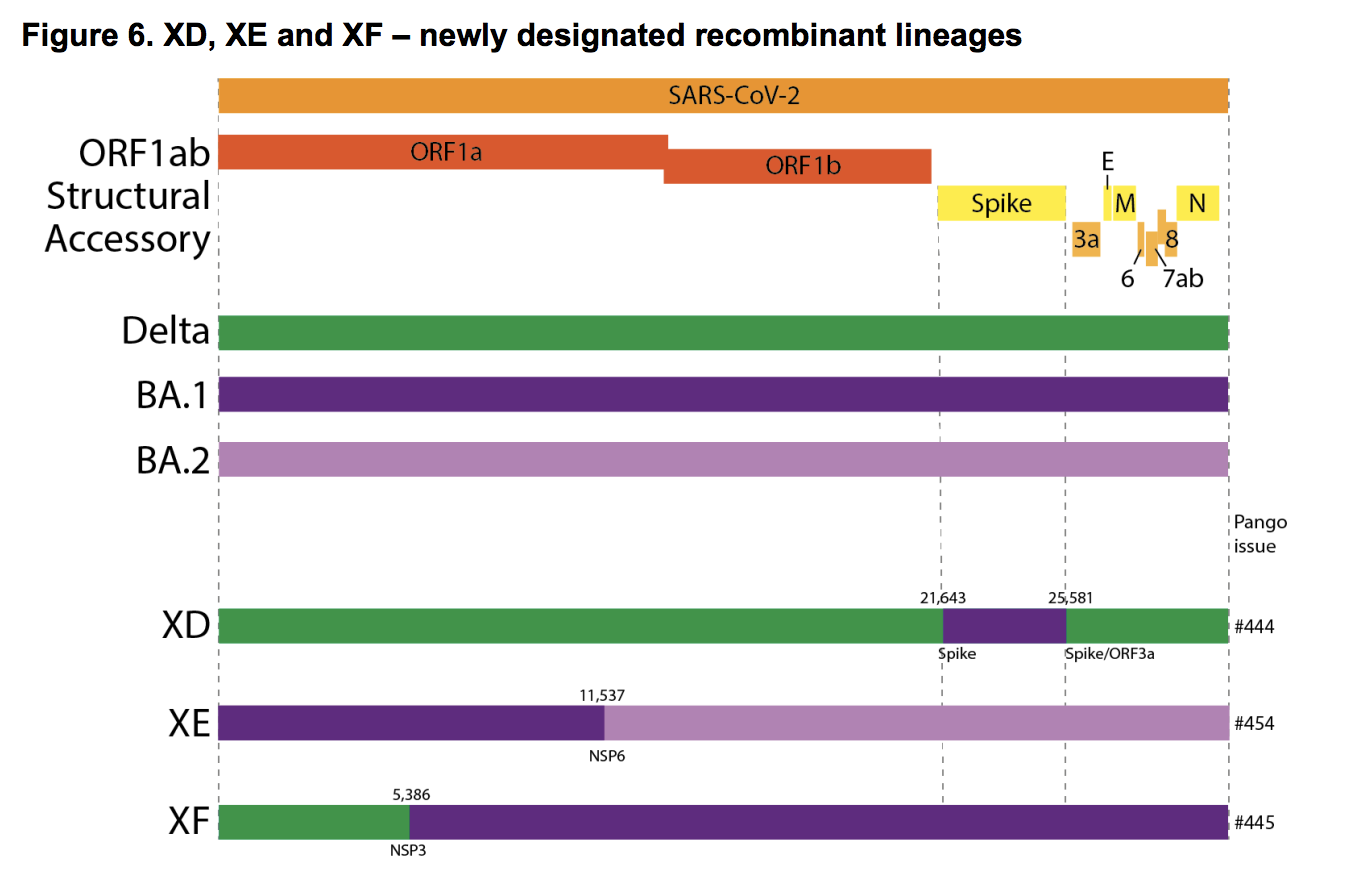
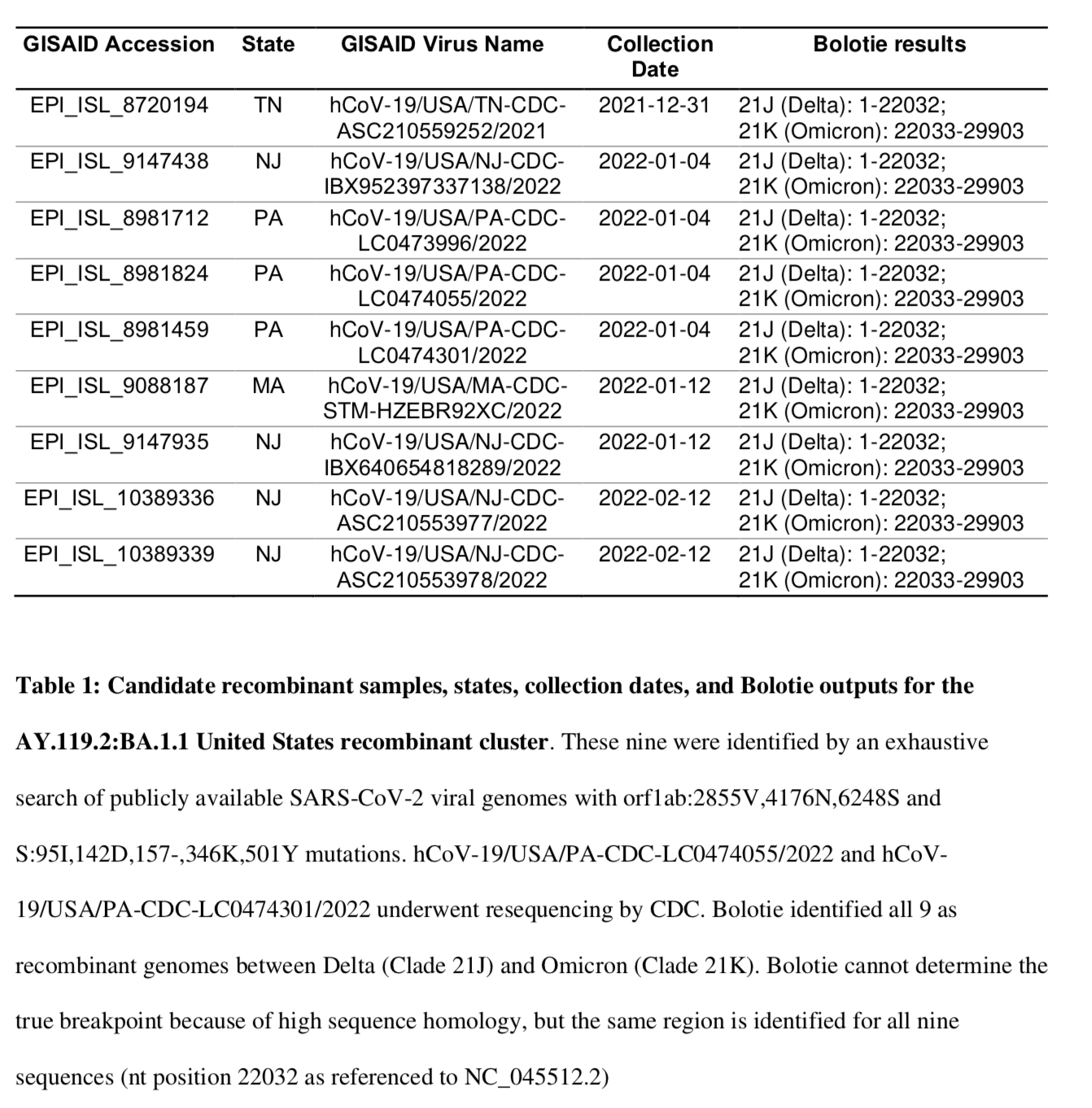
| USA | 91,170,571(ranked #1) 1,663,488 new infections in the last 14 days. | 94,037(ranked #4) 21 states failed to report infections. | 1,048,693(ranked #1) 5,412 new deaths in the last 14 days. | 207 27 states failed to report deaths. | 26.72%* *Not updated | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India) | No | No |
| Brazil | 33,250,117(ranked #3) 816,054 new infections in the last 14 days. | 107,959 (ranked #4) | 675,145(ranked #2; 3,145 new deaths in 14 days) | 299 | 15.42% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| India | 43,730,071(ranked #2); 241,552 new infections in 2 weeks. | 20,044 | 525,660(ranked #3) | 56 | 3.10% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2.75 (India) | No | No |
| United Kingdom* *No reported data for 7/14/22- 7/16/22 | 23,075,360(ranked #6) 334,295 new infections in 2 weeks. | – | 181,580 (ranked #7) | – | 33.63% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India) | No | No |
| California, USA | 10,380,889(ranked #12 in the world; 226,544 new infections in the last 14 days). | 8,694 | 93,017 (ranked #20 in world) 397 new deaths in the last 14 days | 16 | 26.27% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa)BA.5 (South Africa) | No | No |
| Mexico | 6,373,876(ranked #18) 339,174 new infections in 14 days). | 34,885(ranked #9) | 326,335(ranked #5) | 74 | 4.84% | B2 lineageAlpha/B.1.1.7 (UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| South Africa | 3,999,751(ranked #33; 5,528 new infections in 14 days). | 406 | 101,918 (ranked #18) | 3 | 6.57% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| Canada | 4,007,463(ranked #32) 61,376 new infections in 14 days). | 1,881 | 43,555(ranked #24) | 51 | 10.43% . | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Poland | 6,029,947 (ranked #21; 14,313 new infections in 14 days). | 1,974 | 116,470 (ranked #15) | 2 | 15.96% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3 | No | No |
| Russia | 18,480,934(ranked #9), 47,540 new infections in 14 days). | 4,457 | 381,794(ranked #4 in world) | 40 | 12.65% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)R1 (Japan) B.1.640.1 (Congo/France)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Argentina | 9,426,171(ranked #14; 58,999 new infections in 14 days). | ———– | 140,365 (ranked #14) | ——– | 20.47% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gama/P.1 (Brazil)Delta/B.1.617.2 (India)Lambda/C.37 (Peru)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Colombia | 6,223,497(ranked #19, 48,316 new infections in 14 days). | 3,523 | 140,365 (ranked #13) | 26 | 11.97% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Epsilon/B.1.427 + B.1.429 (USA)*Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Peru | 3,714,361(ranked #38, 84,565 new infections in 14 days). | 10,610 | 235,526(ranked #6) | 15 | 10.95% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Iran | 7,270,023(ranked 17th; 31,434 new infections in last 14 days) | 4,772 | 141,477(ranked #11) | 13 | 8.43% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Spain | 13,090,476(ranked 11th; 272,292 new infections in 14 days). | 19,211(ranked #12) | 109,348 (ranked #17) | 134 | 27.97% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
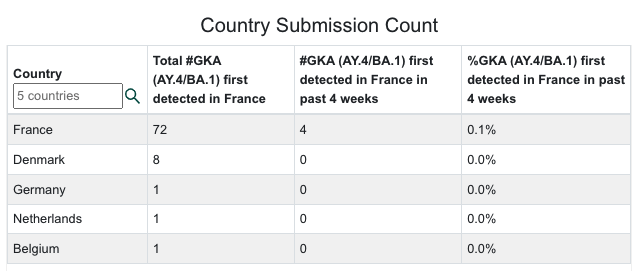
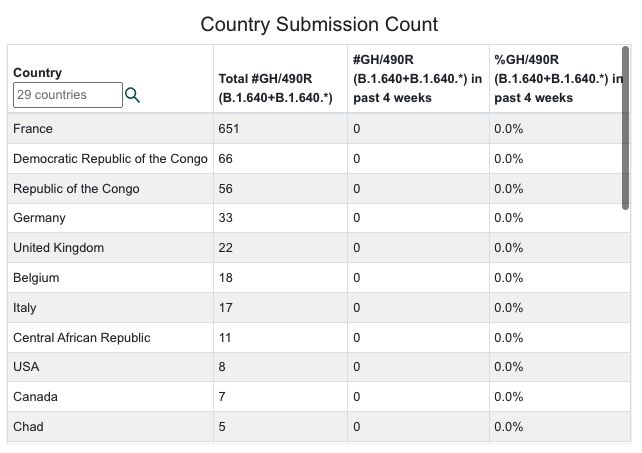
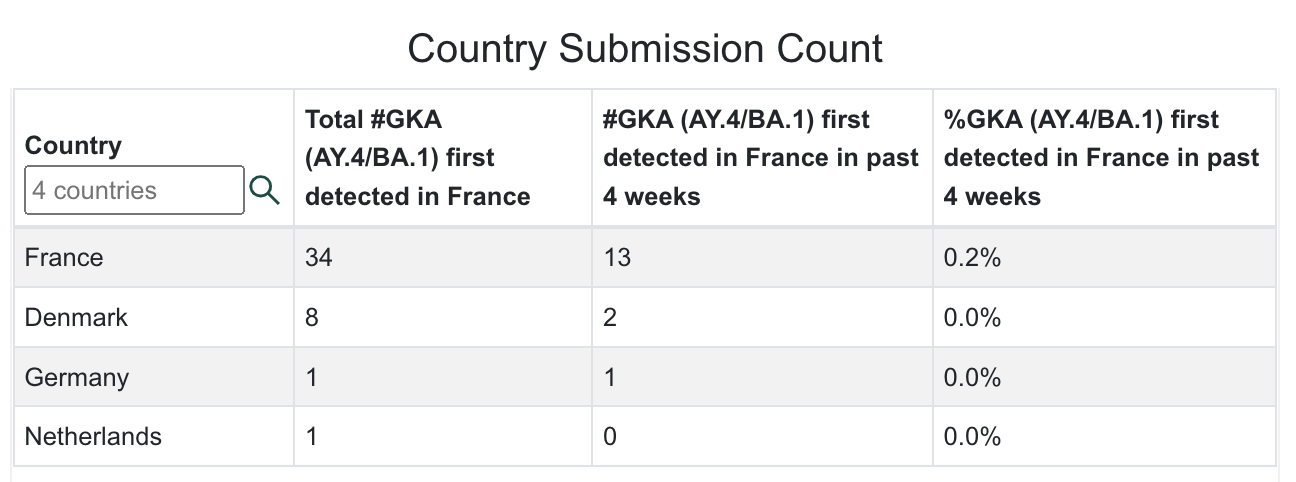
| France | 32,818,901 (ranked #4; 1,609,976 new infections in the last 14 days). | 119,684 (ranked #1) | 150,576 (ranked #10) | 108 | 50.05% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant | No | No |
| Germany | 29,692,989(ranked #5; 1,300,360 new infections in 14 days.). | 123,046 (ranked #2) | 142,535 (ranked #11) | 134 | 35.21% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| South Korea | 18,680,142 (ranked #9 310,285 new infections in 14 days). | 38,864(ranked #8) | 24,712 (ranked #38) | 16 | 36.37% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Vietnam | 10,759,145 (ranked #12; 11,748 new infections in 14 days). | 956 | 43,090 (ranked #26) | – | 10.85% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Netherlands | 8,274,234 (ranked #16; 83,979 new infections in 14 days). | 6,527 | 22,422 (ranked #41) | 5 | 48.07% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Denmark | 3,039,859 (ranked #39) 23,810 new infections in 14 days | 1,567 | 6,551 (ranked #81) | 8 | 52.10% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| North Korea (DPRK) | 4,770,400 (ranked #24; 25,670 new infections in 14 days) | 500 | 74 | – | 18.34% | Omicron/B.1.1.529 South Africa November 2021) | No | No |
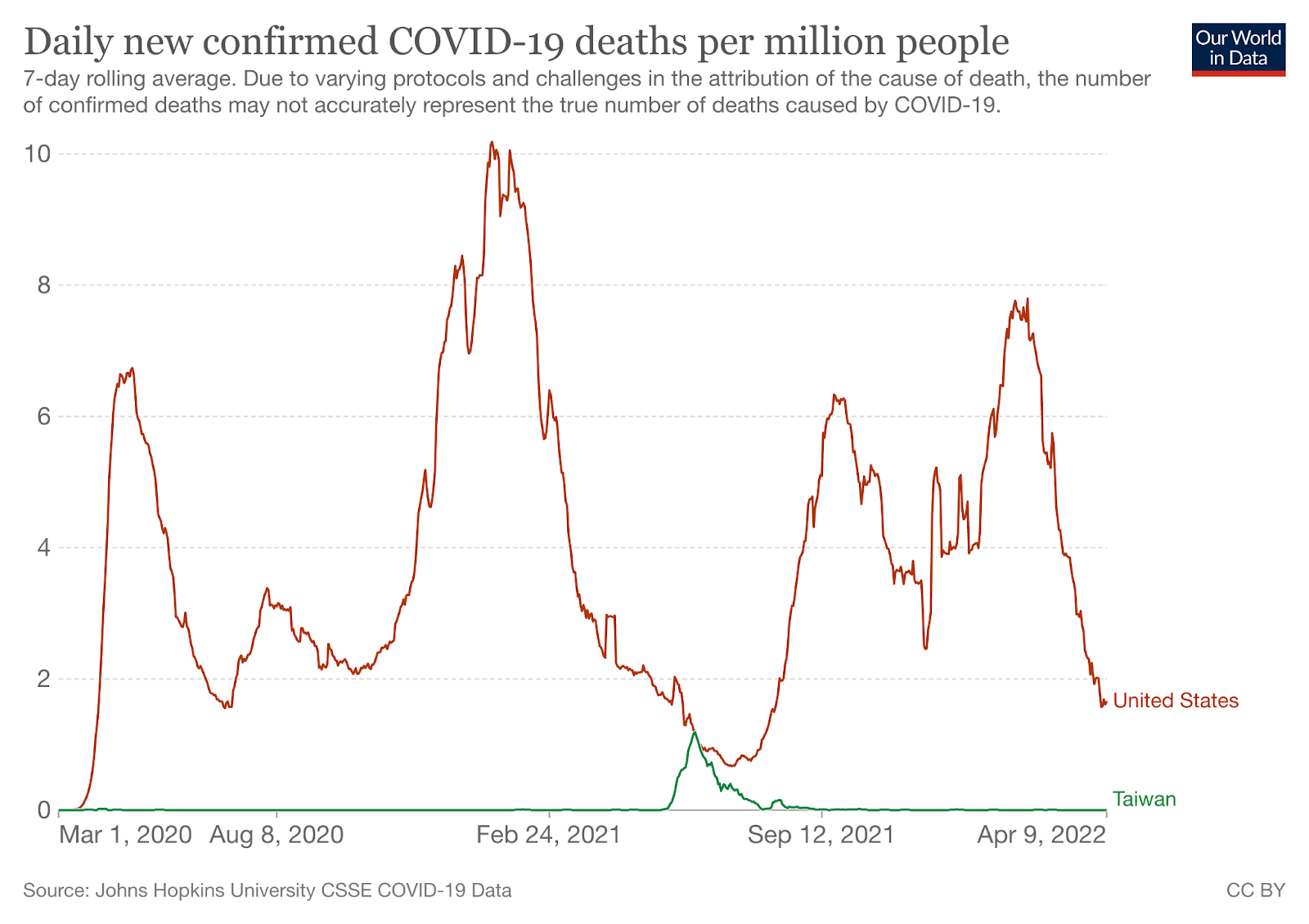
| Taiwan | 4,215,200(ranked #30) 412,171 new infections in 14 days | 25,310 (ranked #10) | 7,917 (ranked #73) | 114 | 17.63% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Japan | 10,000,720(ranked #13) 671,200 new infections in the last 14 days | 97,339(ranked #5) | 31,528(ranked #34) | 34 | 7.95% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
What Our Team Is Reading This Week
- SARS-CoV-2 Omicron BA.5: Evolving tropism and evasion of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. (Preprint) https://doi.org/10.1101/2022.07.07.22277128
- Brain imaging and neuropsychological assessment of individuals recovered from mild to moderate SARS-CoV-2 infection (Preprint) https://doi.org/10.1101/2022.07.08.22277420
- Increased Risk of Herpes Zoster in Adults ≥50 Years Old Diagnosed With COVID-19 in the United States (Open Forum Infectious Diseases) https://doi.org/10.1093/ofid/ofac118
- Neutralization sensitivity of Omicron BA.2.75 to therapeutic monoclonal antibodies (Preprint) https://doi.org/10.1101/2022.07.14.500041
- Neutralizing antibody activity against 21 SARS-CoV-2 variants in older adults vaccinated with BNT162b2 (Nature Microbiology) https://doi.org/10.1038/s41564-022-01163-3
- How COVID-19 affects microvessels in the brain (Brain) https://doi.org/10.1093/brain/awac211
- Fine Analysis of Lymphocyte Subpopulations in SARS-CoV-2 Infected Patients: Differential Profiling of Patients With Severe Outcome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.889813
- SARS-CoV-2 accelerated clearance using a novel nitric oxide nasal spray (NONS) treatment: A randomized trial (The Lancet Regional Health – Southeast Asia) https://doi.org/10.1016/j.lansea.2022.100036
- Effectiveness of 2, 3, and 4 COVID-19 mRNA Vaccine Doses Among Immunocompetent Adults During Periods when SARS-CoV-2 Omicron BA.1 and BA.2/BA.2.12.1 Sublineages Predominated — VISION Network, 10 States, December 2021–June 2022 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7129e1
- Characterization of virologic rebound following nirmatrelvir-ritonavir treatment for COVID-19 (Clinical Infectious Diseases) https://doi.org/10.1093/cid/ciac512
- Potential Autoimmunity Resulting from Molecular Mimicry between SARS-CoV-2 Spike and Human Proteins (Preprint) https://doi.org/10.1101/2021.08.10.455737
- COVID-19 positive patients at higher risk of developing neurodegenerative disorders, new study shows (Medical Express) https://medicalxpress.com/news/2022-06-covid-positive-patients-higher-neurodegenerative.html
- Evidence of previous SARS-CoV-2 infection in seronegative patients with long COVID (eBioMedicine) https://doi.org/10.1016/j.ebiom.2022.104129
- SARS-CoV-2 infection induces inflammatory bone loss in golden Syrian hamsters (Nature Communications) https://doi.org/10.1038/s41467-022-30195-w
- Persistent 129Xe MRI Pulmonary and CT Vascular Abnormalities in Symptomatic Individuals with Post-Acute COVID-19 Syndrome (Radiology) https://doi.org/10.1148/radiol.220492
- ACE2-independent infection of T lymphocytes by SARS-CoV-2 (Signal Transduction and Targeted Therapy) https://doi.org/10.1038/s41392-022-00919-x
- Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae (Preprint) https://doi.org/10.1101/2022.06.14.22276401
- SARS-CoV-2 is detected in the gastrointestinal tract of asymptomatic endoscopy patients but is unlikely to pose a significant risk to healthcare personnel (Gastro Hep Adv) https://doi.org/10.1016/j.gastha.2022.06.002
- Long COVID symptoms in SARS-CoV-2-positive children aged 0–14 years and matched controls in Denmark (LongCOVIDKidsDK): a national, cross-sectional study (Child & Adolescent Health) https://doi.org/10.1016/S2352-4642(22)00154-7
- Age and sex-specific risks of myocarditis and pericarditis following Covid-19 messenger RNA vaccines (Nature Communications) https://doi.org/10.1038/s41467-022-31401-5
- COVID-19 positive patients at higher risk of developing neurodegenerative disorders, new study shows https://medicalxpress.com/news/2022-06-covid-positive-patients-higher-neurodegenerative.html
- Posttranslational modifications optimize the ability of SARS-CoV-2 spike for effective interaction with host cell receptors (Biophysics and Computational Biology) https://doi.org/10.1073/pnas.2119761119
- Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2 (The Lancet) https://doi.org/10.1016/S0140-6736(22)00941-2
- Antibody escape of SARS-CoV-2 Omicron BA.4 and BA.5 from vaccine and BA.1 serum (Cell) https://doi.org/10.1016/j.cell.2022.06.005
- Immunomodulatory treatment in postural tachycardia syndrome: A case series (European Journal of Neurology) https://doi.org/10.1111/ene.14711
- Long COVID-19 Liver Manifestation in Children (JPGN) https://journals.lww.com/jpgn/abstract/9900/long_covid_19_liver_manifestation_in_children.84.aspx
- Cross-reactive immunity against the SARS-CoV-2 Omicron variant is low in pediatric patients with prior COVID-19 or MIS-C (Nature Communications) https://doi.org/10.1038/s41467-022-30649-1
- C.D.C. Dismisses Airborne Transmission of Monkeypox. Some Experts Disagree. (NY Times) https://www.nytimes.com/2022/06/10/health/monkeypox-airborne.html
- Omicron BA.1 breakthrough infection drives cross-variant neutralization and memory B cell formation against conserved epitopes (Science Immunology) https://doi.org/10.1126/sciimmunol.abq2427
- SARS-CoV-2 Infection and Persistence Throughout the Human Body and Brain (National Institutes of Health) https://videocast.nih.gov/watch=45296?jwsource=twi
- Long COVID is associated with extensive in-vivo neuroinflammation on [18F]DPA-714 PET (Preprint) https://doi.org/10.1101/2022.06.02.22275916
- Unexpected worsening of progressive multifocal leucoencephalopathy following COVID-19 pneumonia (Journal of Neurovirology) https://doi.org/10.1007%2Fs13365-021-00980-2
- Virological characteristics of the novel SARS-CoV-2 Omicron variants including BA.2.12.1, BA.4 and BA.5 (Preprint) https://doi.org/10.1101/2022.05.26.493539
- During the Omicron Wave, Death Rates Soared for Older People (NY Times with CDC data) https://www.nytimes.com/2022/05/31/health/omicron-deaths-age-65-elderly.html
- PD-1 blockade counteracts post–COVID-19 immune abnormalities and stimulates the anti–SARS-CoV-2 immune response (JCI Insight) https://insight.jci.org/articles/view/146701
- Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance (Nature Reviews Clinical Oncology) https://doi.org/10.1038/s41571-019-0218-0
- Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study (Observational Research) https://doi.org/10.1007/s00296-022-05146-9
- An early warning system for emerging SARS-CoV-2 variants (Nature Medicine) https://doi.org/10.1038/s41591-022-01836-w
- SARS-CoV-2 Omicron Variant is as Deadly as Previous Waves After Adjusting for Vaccinations, Demographics, and Comorbidities (Preprint) https://doi.org/10.21203/rs.3.rs-1601788/v1
- Partial ORF1ab Gene Target Failure with Omicron BA.2.12.1 (Preprint) https://www.medrxiv.org/content/10.1101/2022.04.25.22274187v1
- COVID-19 Associated Hepatitis in Children (CAH-C) during the second wave of SARS-CoV-2 infections in Central India: Is it a complication or transient phenomenon. (Preprint) https://doi.org/10.1101/2021.07.23.21260716
- Liver and Gastrointestinal Involvement in Patients With COVID-19: A Retrospective Study https://www.cureus.com/articles/90062-liver-and-gastrointestinal-involvement-in-patients-with-covid-19-a-retrospective-study
- Cortical Grey Matter Volume Loss links to Neurological Sequelae in post COVID-19 “Long Haulers” (Preprint) https://doi.org/10.21203/rs.3.rs-1582065/v1
- Virological characteristics of the SARS-CoV-2 Omicron BA.2 spike (Cell) https://doi.org/10.1016/j.cell.2022.04.035
- Continued Emergence and Evolution of Omicron in South Africa: New BA.4 and BA.5 lineages https://www.krisp.org.za/manuscripts/MEDRXIV-2022-274406v1-deOliveira.pdf
- Molecular consequences of SARS-CoV-2 liver tropism (Nature Metabolism) https://doi.org/10.1038/s42255-022-00552-6
- China CDC shares latest COVID-19 data (GISAID) https://www.gisaid.org/resources/gisaid-in-the-news/china-shares-latest-11-apr-2022/#c920
- Persistent COVID-19 symptoms in a community study of 606,434 people in England (Nature) https://www.nature.com/articles/s41467-022-29521-z
- Brain Inflammation and Intracellular α-Synuclein Aggregates in Macaques after SARS-CoV-2 Infection (Viruses) https://www.mdpi.com/1999-4915/14/4/776
- Antibody Resistance of SARS-CoV-2 Omicron BA.1, BA.1.1, BA.2 and BA.3 Sub-lineages (Preprint) https://www.biorxiv.org/content/10.1101/2022.04.07.487489v1
- Infectious viral load in unvaccinated and vaccinated individuals infected with ancestral, Delta or Omicron SARS-CoV-2 (Nature Medicine) https://www.nature.com/articles/s41591-022-01816-0
- Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain (Preprint) https://www.biorxiv.org/content/10.1101/2022.01.07.475453v1
- Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: nationwide self-controlled cases series and matched cohort study (BMJ) https://www.bmj.com/content/377/bmj-2021-069590
- SARS-CoV-2 Infection Induces Ferroptosis of Sinoatrial Node Pacemaker Cells (Circulation Research) https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.320518
- SARS-CoV-2 variants of concern and variants under investigation in England (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1063424/Tech-Briefing-39-25March2022_FINAL.pdf
- Neutralization of Omicron BA.1, BA.2, and BA.3 SARS-CoV-2 by 3 doses of BNT162b2 vaccine (Preprint) https://doi.org/10.1101/2022.03.24.485633
- COVID-19-Associated Encephalitis: Two Case Reports https://www.cureus.com/articles/86903-covid-19-associated-encephalitis-two-case-reports
- First evidence that an emerging mammalian alphacoronavirus is able to infect an avian species (Transboundary and Emerging Diseases) https://doi.org/10.1111/tbed.14535
- SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses (The Lancet) https://doi.org/10.1016/S0140-6736(22)00383-X
- Evidence for SARS-CoV-2 Delta and Omicron co-infections and recombination (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.09.22272113v1
- Culture and identification of a “Deltamicron” SARS-CoV-2 in a three cases cluster in southern France (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.03.22271812v1.full
- Mandatory masking in schools reduced COVID-19 cases during Delta surge (NIH press release) https://www.nih.gov/news-events/news-releases/mandatory-masking-schools-reduced-covid-19-cases-during-delta-surge
- School Masking Policies and Secondary SARS-CoV-2 Transmission (Pediatrics) https://publications.aap.org/pediatrics/article/doi/10.1542/peds.2022-056687/185379/School-Masking-Policies-and-Secondary-SARS-CoV-2
- Transmission of SARS-CoV-2 delta variant (AY.127) from pet hamsters to humans, leading to onward human-to-human transmission: a case study (The Lancet) https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00326-9/fulltext
- COVID-19 Variant Dashboard – USA by Raj Rajnarayanan https://public.tableau.com/app/profile/raj.rajnarayanan/viz/USAVariantDB/VariantDashboard
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 38 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1060337/Technical-Briefing-38-11March2022.pdf
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 37 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1057359/Technical-Briefing-37-25February2022.pdf
- Engineered extracellular vesicles antagonize SARS-CoV-2 infection by inhibiting mTOR signaling (Biomaterials and Biosystems) https://www.sciencedirect.com/science/article/pii/S2666534422000046?via%3Dihub
- Severe Neuro-COVID is associated with peripheral immune signatures, autoimmunity and neurodegeneration: a prospective cross-sectional study (Preprint) https://doi.org/10.21203/rs.3.rs-1385593/v1
- Dynamics of the Delta and Omicron variants of SARS-CoV-2 in the United States: the battle of supremacy in the presence of vaccination, mask usage and antiviral treatment (Preprint) https://doi.org/10.21203/rs.3.rs-1420446/v1
- Virological characteristics of SARS-CoV-2 BA.2 variant (Preprint) https://www.biorxiv.org/content/10.1101/2022.02.14.480335v1
- Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: Evidence from Danish Households (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.28.22270044v1
- Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance — VISION Network, 10 States, August 2021–January 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7107e2.htm?s_cid=mm7107e2_e&ACSTrackingID=USCDC_921-DM75599&ACSTrackingLabel=MMWR%20Early%20Release%20-%20Vol.%2071%2C%20February%2011%2C%202022&deliveryName=USCDC_921-DM75599
- SARS-CoV-2 B.1.1.529 (Omicron) Variant Transmission Within Households — Four U.S. Jurisdictions, November 2021–February 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7109e1.htm?s_cid=mm7109e1_w
- Pediatric Emergency Department Visits Before and During the COVID-19 Pandemic — United States, January 2019–January 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7108e1.htm?s_cid=mm7108e1_w#F2_down
- Birth Of The Omicron Family: BA.1, BA.2, BA.3. Each As Different As Alpha Is From Delta. (Forbes) https://www.forbes.com/sites/williamhaseltine/2022/01/26/birth-of-the-omicron-family-ba1-ba2-ba3-each-as-different-as-alpha-is-from-delta/?sh=403de4ee3da9
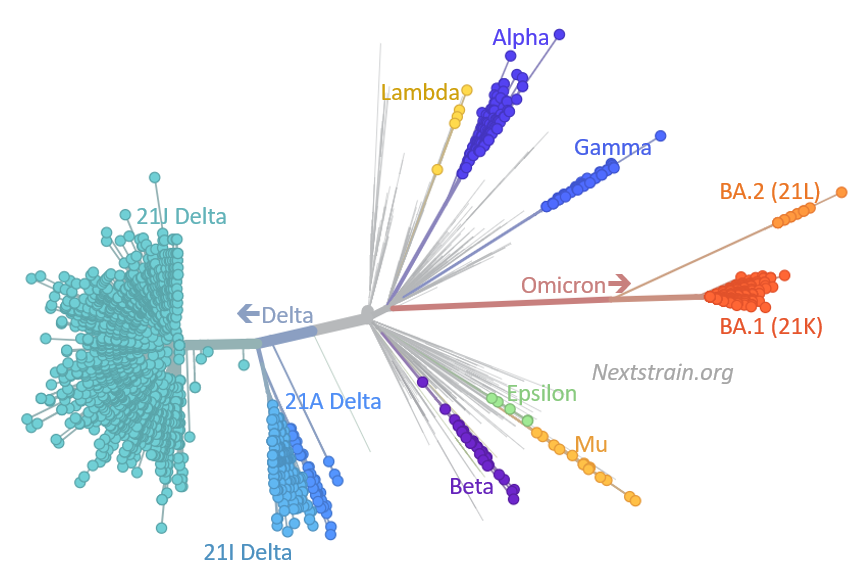
- Take a look at SARS-CoV-2’s family tree. It’s full of surprises (NPR) https://www.npr.org/sections/goatsandsoda/2022/02/09/1047616658/take-a-look-at-sars-cov-2s-family-tree-its-full-of-surprises
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 35 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050999/Technical-Briefing-35-28January2022.pdf
- Memory B cell repertoire from triple vaccinees against diverse SARS-CoV-2 variants (Nature) https://www.nature.com/articles/s41586-022-04466-x_reference.pdf
- Dynamics of infection-elicited SARS-CoV-2 antibodies in children over time (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.14.22269235v1
- Syncytin, envelope protein of human endogenous retrovirus (HERV): no longer ‘fossil’ in human genome (Animal Cells and Systems) https://doi.org/10.1080/19768354.2021.2019109
- Host Chitinase 3-like-1 is a Universal Therapeutic Target for the Delta, Omicron and Other SARS-CoV-2 Viral Variants in COVID 19 (Preprint) https://www.biorxiv.org/content/10.1101/2022.01.21.477274v1
- COVID-19 reinfections among naturally infected and vaccinated individuals (Nature) https://www.nature.com/articles/s41598-022-05325-5
- Duration of Protection against Mild and Severe Disease by Covid-19 Vaccines (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMoa2115481
- Neutralizing immunity in vaccine breakthrough infections from the SARS-CoV-2 Omicron and Delta variants (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.25.22269794v1
- COVID-19 and the Common Cold—Preexisting Coronavirus Antibodies May Hinder SARS-CoV-2 Immunity (JAMA) https://jamanetwork.com/journals/jama/fullarticle/2788621?guestAccessKey=0bbad800-e651-496b-8046-d124bbc63a5a&term=01262022&utm_source=silverchair&utm_medium=email&utm_campaign=article_alert-jama&utm_content=olf&utm_term=012622
- Viral dynamics and duration of PCR positivity of the SARS-CoV-2 Omicron variant https://dash.harvard.edu/handle/1/37370587




























































You must be logged in to post a comment.