
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.

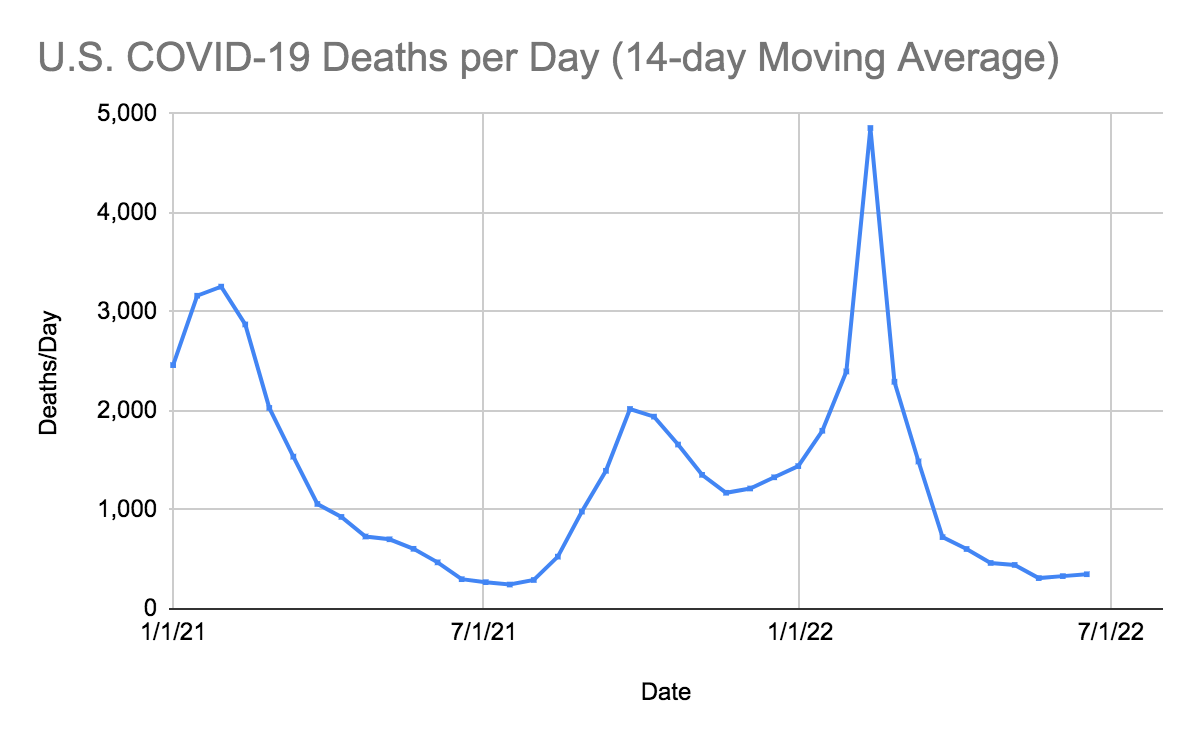
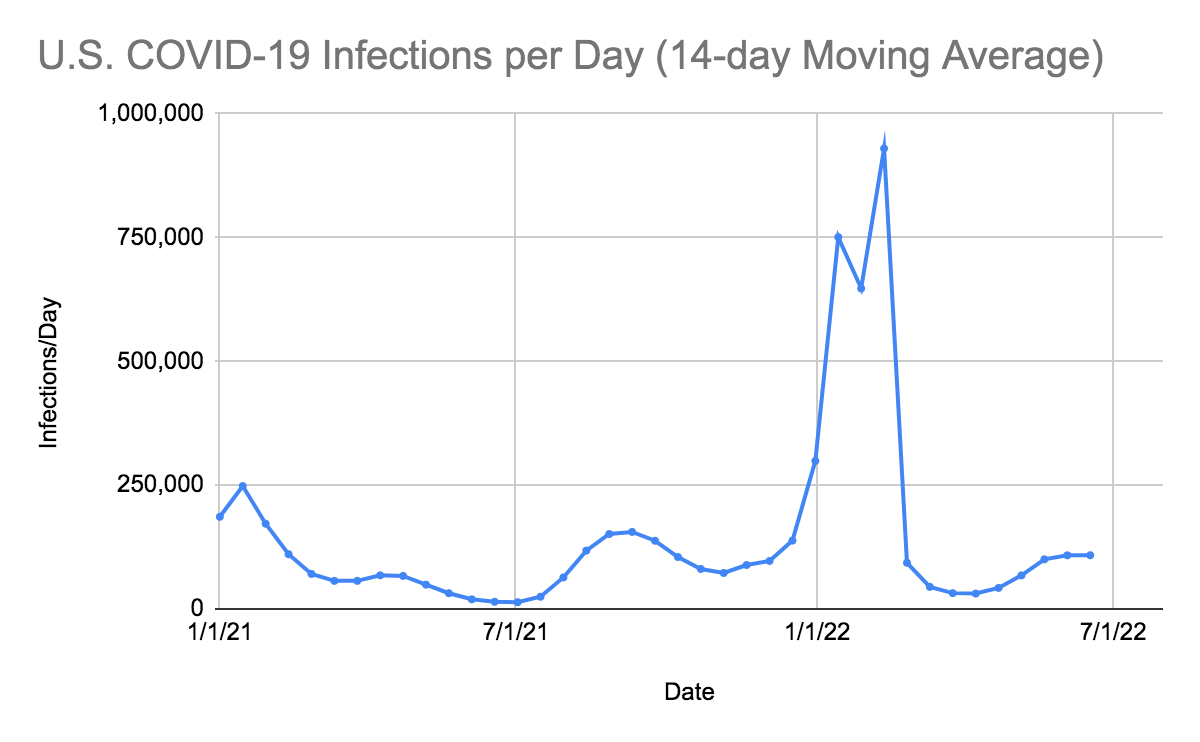
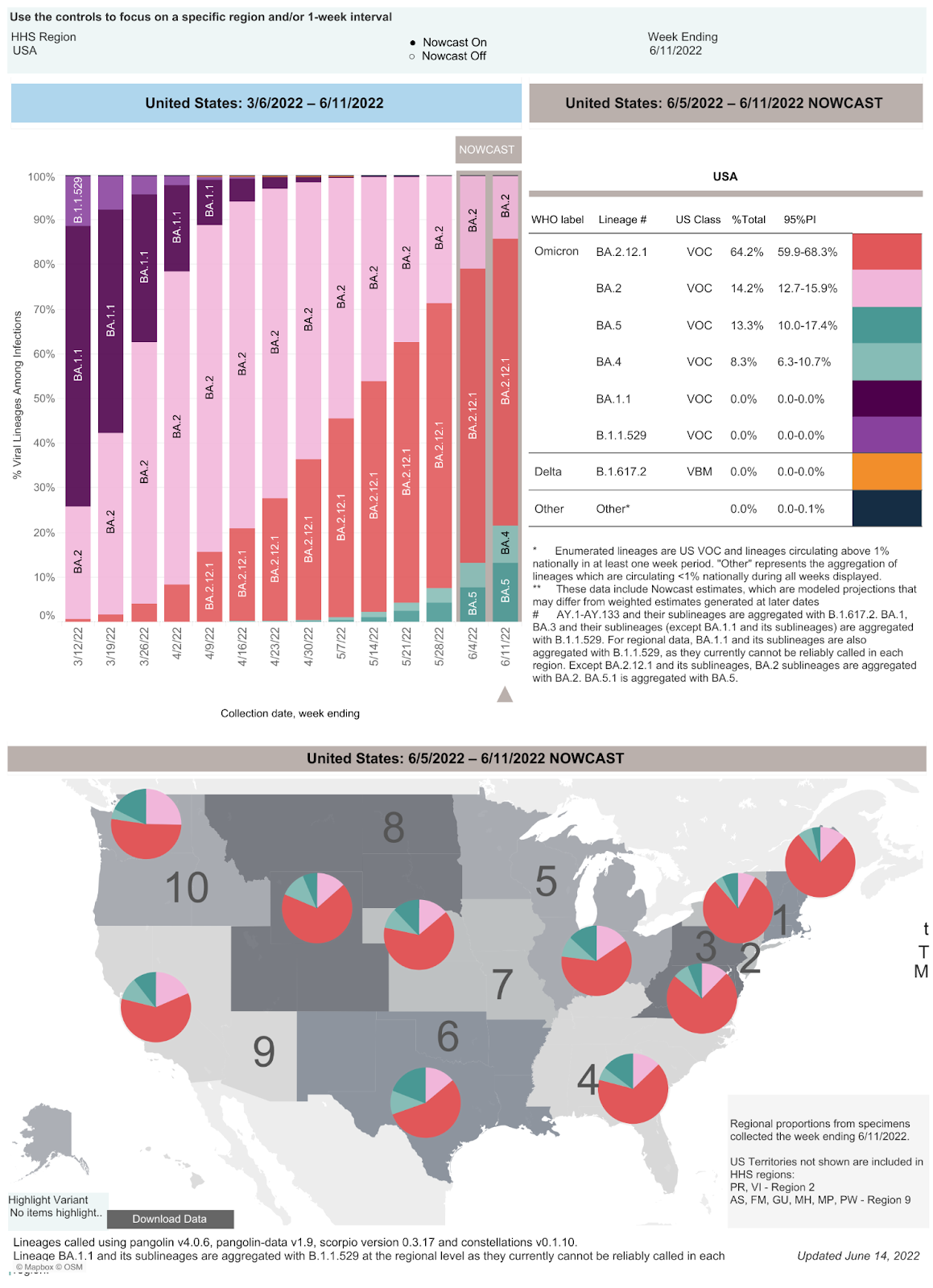
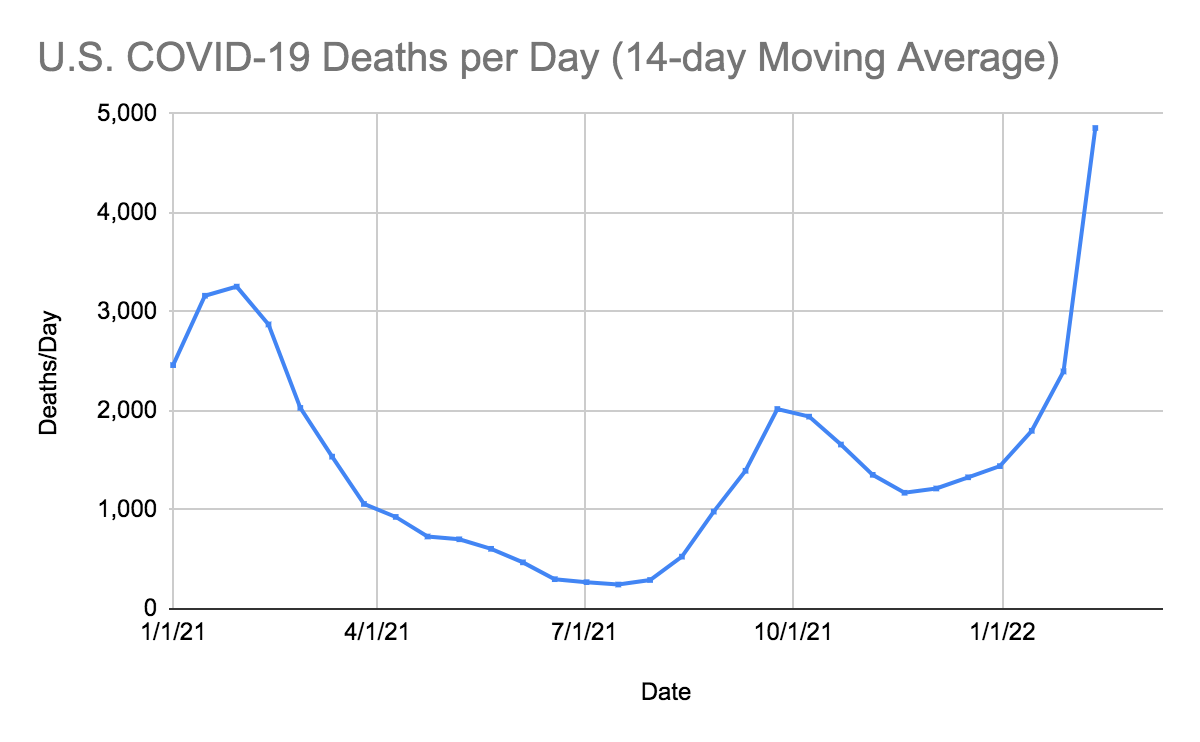
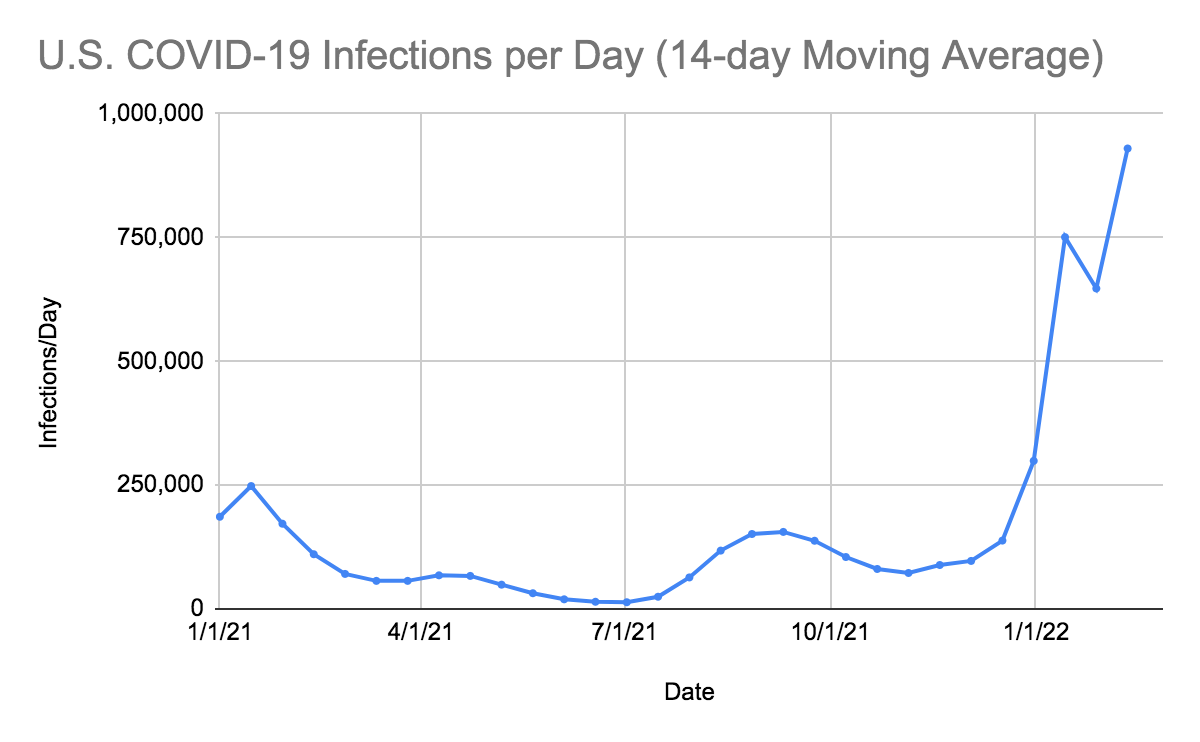
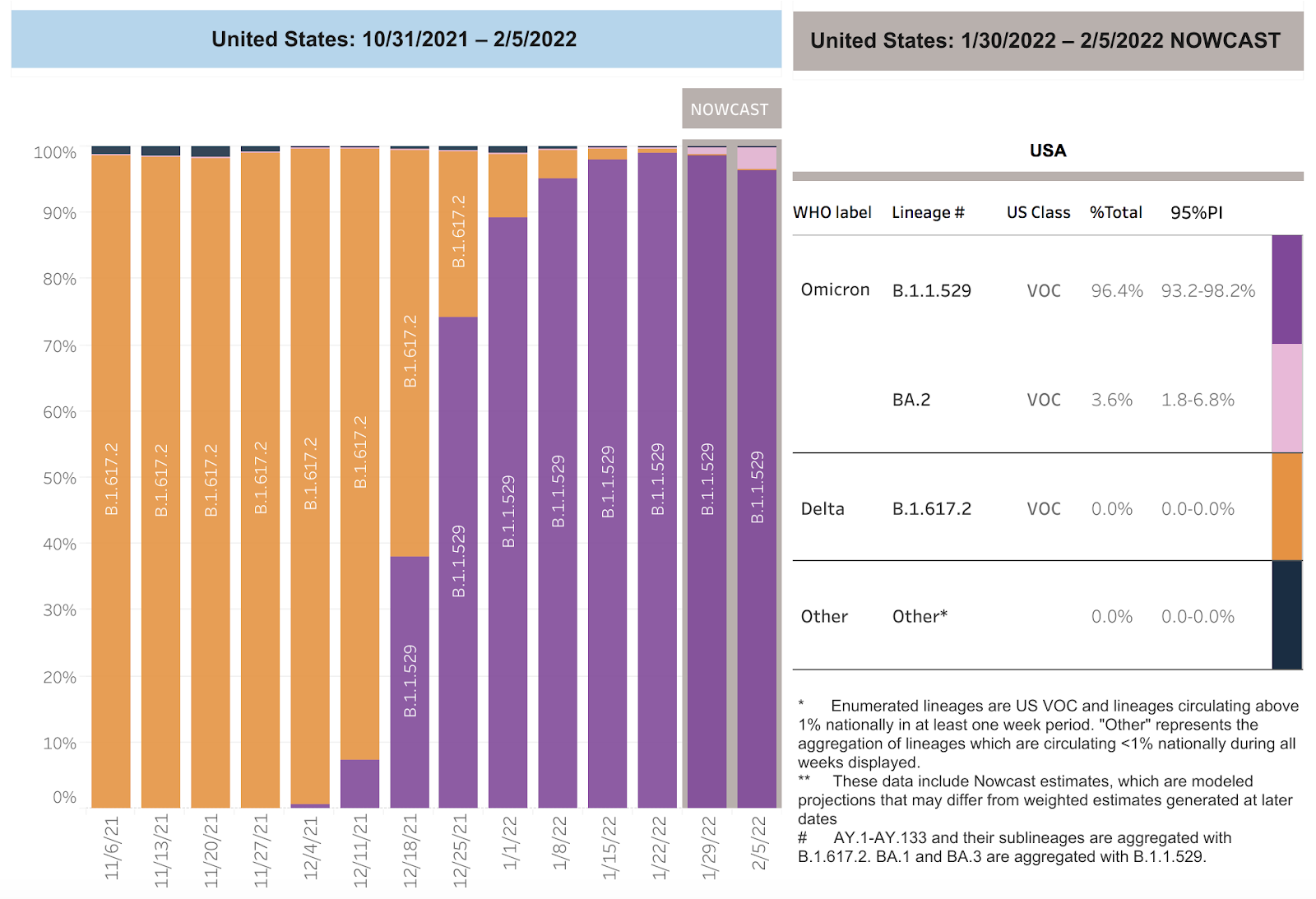
SARS-CoV-2 infections per day have been increasing in the United States for 8 consecutive weeks despite underreporting by states and the failure to capture positive home tests and a decreased screening program in most states. Deaths per day had been decelerating at a rapid rate in the United States but are now increased by 19 more deaths per day. The number of infections have increased as the Omicron BA.2.12.1, BA.2, BA.4, and BA.5 variants of SARS CoV-2 have spread across the nation. The CDC estimates that BA.2.12.1 accounted for 64.2% of isolates, BA.2 accounted for 14.2%, BA.5 accounted for 13.3%, BA.4 accounted for 8.3%, and B.1.1.529 accounted for 0% in the week ending June 11.
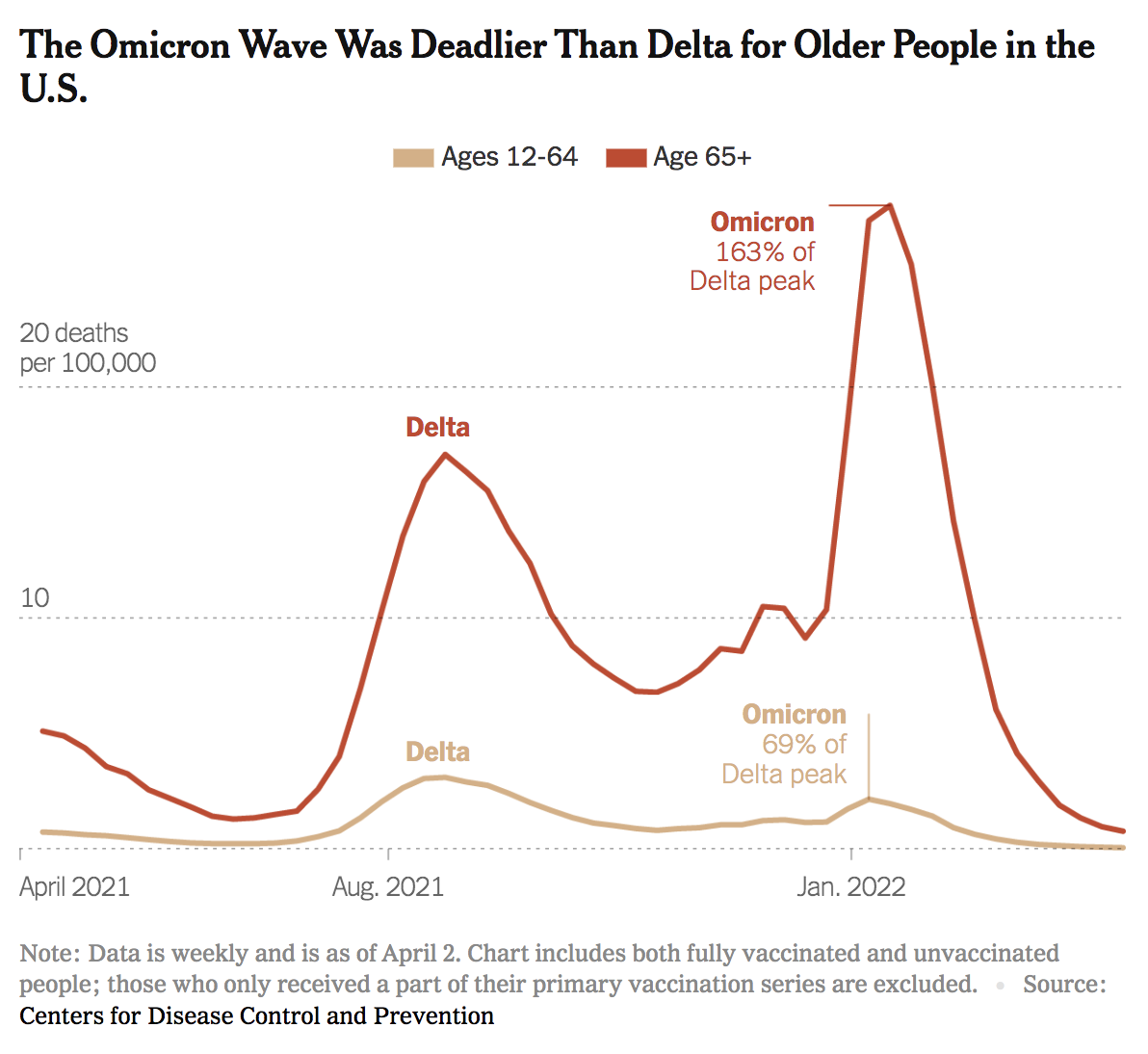
We frequently hear messaging from health officials and politicians that Omicron is “mild,” especially compared to the Delta variant, and as a result, many of our patients believe that they no longer need to wear their masks. This is a dangerous misconception. SARS-CoV-2 still remains a highly transmissible, airborne virus. The following graph, based on CDC data from April 2, 2022, shows that Omicron deaths in people over 65 are much higher than Delta deaths in the same age group. In fact, the peak of Omicron deaths in people over 65 years of age is 163% higher than the Delta peak. The death rate from Omicron is only lower than Delta in the populations between 12 and 64 years of age. Until we have more data on these newer mutants of SARS-CoV-2, we will not know the lethality of each variant. It may take months to measure objective differences in the death rates of new circulating variants. We recommend that all of our patients and family members continue to wear N95 masks in all enclosed spaces.
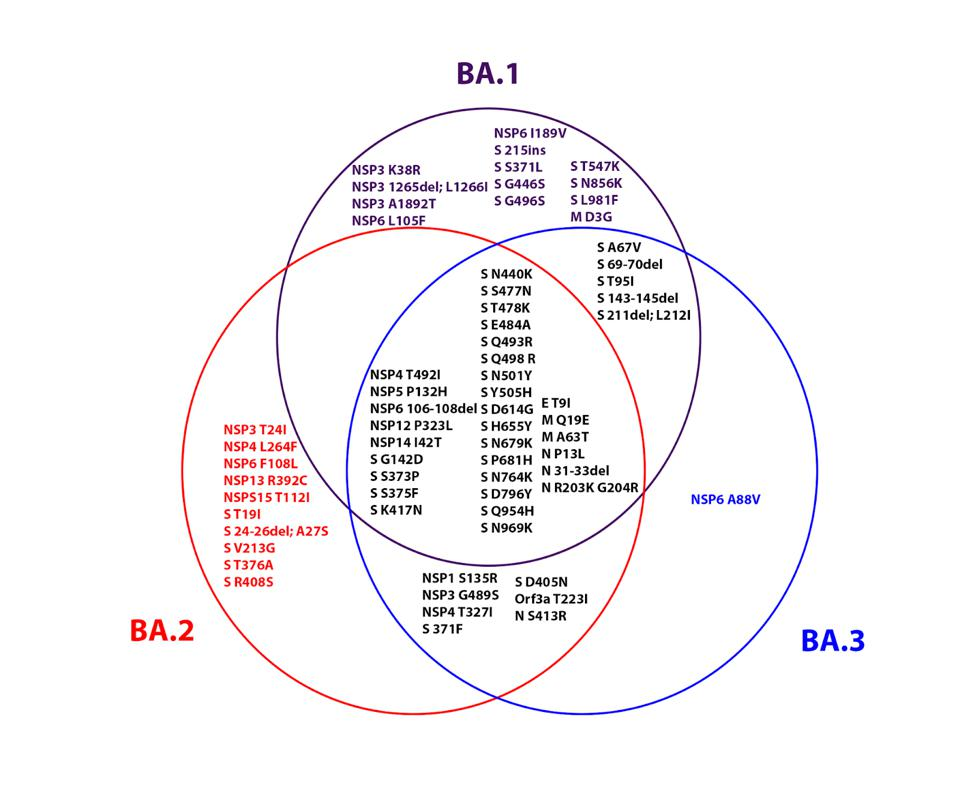
According to the UK Health Security Agency, “BA.4 shares all mutations/deletions with the BA.2 lineage except the following: S: 69/70 deletion, R408 (WT, wild type)*, L452R, F486V, Q493 (WT); ORF 7b: L11F; N: P151S; synonymous SNP G12160A” and “BA.5 shares all mutations/deletions with the BA.2 lineage except the following: S: 69/70 deletion, R408 (WT), L452R, F486V, Q493 (WT); ORF6: D61 (WT); M: D3N; synonymous SNPs: G12160A, A27038G, and C27889T.” On May 12, the European CDC designated both BA.4 and BA.5 as variants of concern.
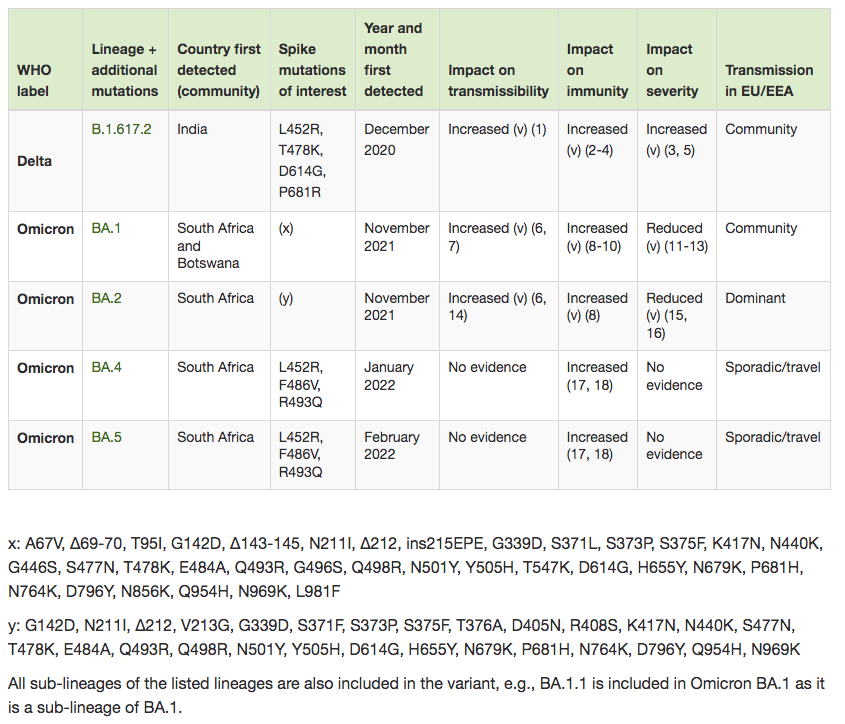
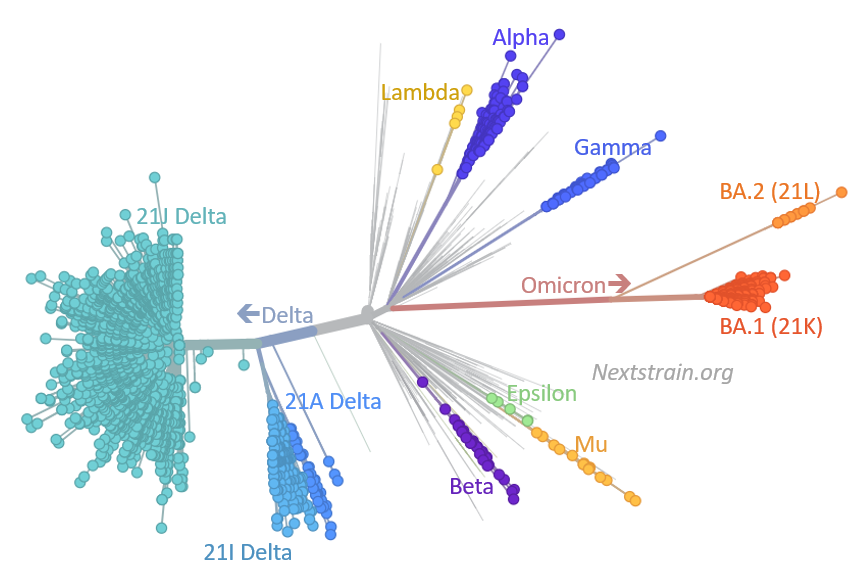
The Omicron variant will continue to mutate just like Delta. There are now 157 Omicron sub-variants (an increase of 57 in the last two weeks) that have been assigned Pango lineages, including 92 sub-lineages of BA.2 (an increase of 42 in two weeks), one sub-lineage of BA.3, three sub-lineages of BA.4, and five sub-lineages of BA.5. There are also two new lineages: BF.1, detected in England, Denmark, Spain and Scotland, and BE.1, detected in South Africa, Austria and England. Curiously, the UK Health Security Agency, which usually releases updates every two weeks, has not released a new Technical Briefing on SARS-CoV-2 variants since May 20.
An additional problem may be the development of recombinant SARS-CoV-2 isolates. A recombinant isolate occurs when two isolates infect the same cell and, in the process of viral reproduction, exchange nucleic acids, creating a new isolate that is a recombination of parts from the genomes of both isolates. A recombinant isolate of Delta AY.4.2.2 and Omicron BA.1.1 was recently reported in the UK. As of 3/25/22 four different recombinant variants of SARS-CoV-2 have been reported by the UK Health Security Agency.
According to the UK Health Security Agency’s Technical Briefing from 3/25/22: “There are currently 3 recombinant lineages being monitored as part of horizon scanning: XD, XE, and XF (Figure 6). XD and XF are Delta and BA.1 recombinants. XE is a BA.1 and BA.2 recombinant and has 3 mutations that are not present in all BA.1 or BA.2 sequences: NSP3 C3241T and V1069I, and NSP12 C14599T. XF and XE are associated with UK sequenced samples. XD is predominantly associated with France. XD contains the unique mutation NSP2:E172D.” As of 5/17/22 the UK Health Security Agency reports 2,049 sequences of the XE recombinant in the UK data.
Omicron variants have mutations which decrease the effectiveness of current vaccines and monoclonal antibodies. The effectiveness of the new Pfizer drug, PAXLOVIDTM, should not be compromised by any of the current mutations in Omicron or Delta variants. Pfizer completed their filing with the FDA on 11/15/21. The FDA approved PAXLOVIDTM on December 22 , 2021.The FDA approved Merck’s drug Molnupiravir on December 23, 2021. On 12/23/21 CVS announced by fax it was selected by the Government to distribute oral PAXLOVIDTM and Molnupiravir. On 12/27/21, another fax from CVS listed which CVS pharmacies in California would have these drugs. Monterey County covers 3,771 square miles with a population of 434,061. Three CVS pharmacies in Monterey, Salinas, and Soledad are the only listed pharmacies in our county. I have now been able to obtain PAXLOVIDTM for infected patients from the CVS in Salinas (phone 831-424-0026), the CVS on Fremont Street in Monterey (phone 831-375-5135) and the CVS in Soledad in south Monterey County (phone 831-678-5110). All require electronic prescriptions written as Paxlovid three tablets twice daily orally for five days (thirty total tablets). Physicians or their staff probably should call to check on drug availability that day.
In the absence of obtaining intravenous Sotrovimab or Bebtelovimab, only oral PAXLOVIDTM and Molnupiravir are available to treat SARS-CoV-2 as an outpatient. Our first Paxlovid failure in an immunocompromised patient was treated the week of 4/5/22 at the Community Hospital of the Monterey Peninsula (Montage) ER as an outpatient with a single one-minute intravenous injection of Bebtelovimab.
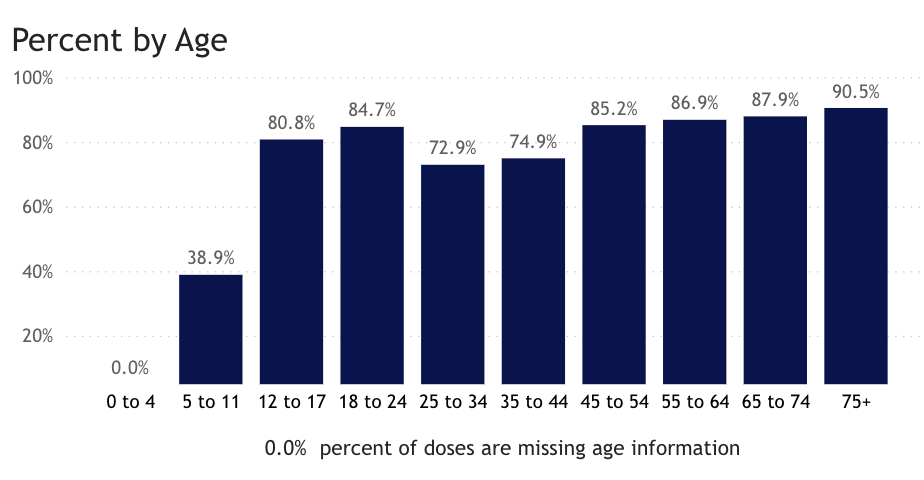
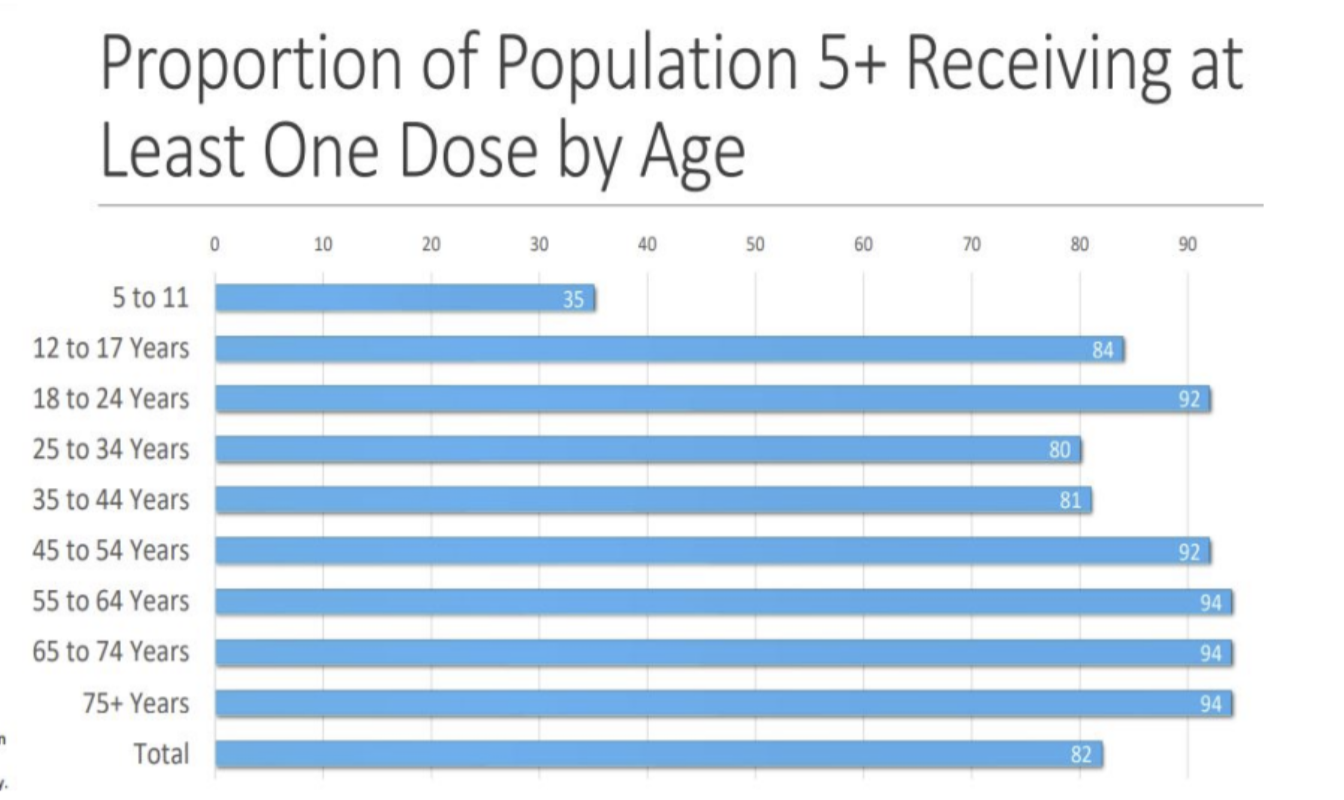
Unless people continue to wear masks and get vaccinated, including their third dose of the vaccine, we will see further spread of the Omicron variants and increase in deaths in people who are not vaccinated, have waning immunity, the immunocompromised population and others with risk factors particularly those older over the age of 64. SARS-CoV-2 is now in the top ten most common causes of death for children. Anyone over the age of 5 years can now get vaccinated in the United States at no cost. This should get done immediately.In Monterey County, as of 6/19/22, only 38.9% of 5-11 year-olds have received the first two doses of vaccine, while 80.8% of 12-17 year-olds have received two doses. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible.
On 6/17/22, the United States had 81,733 documented new infections. There were also 200 deaths. Twenty-one states did not report their infections, and 32 states didn’t report their deaths. In the United States the number of hospitalized patients had been increasing in many areas. Now there are 3.006 patients who are seriously or critically ill; that number was 2,683 two weeks ago. The number of critically ill patients has increased by 323 in the last 14 days, while at least 4,896 new deaths occurred (an increase of 19 deaths per day from the previous 14 days). The number of critically ill patients has increased for the fourth time in twenty-one 14-day periods. Patients are still dying each day (average 350/day). Omicron BA.2, BA.4, BA.5 variants causing infections should continue to increase and critically ill patients may continue to increase. Deaths, which usually lag two to four weeks behind exponential increase in infections, are increasing now. Past infections with a BA.1 or BA.2 variant will not prevent infections with BA.2.12.1, BA.4, or BA.5.
As of 6/17/22, we have had 1,038,265 deaths and 87,968,819 SARS-CoV-2 infections in the United States. We have had 1,518,216 new infections in the last 14 days. We were adding an average of 759,108 infections every seven days. For the pandemic in the United States we are averaging one death for every 84.72 infections or over 11,803 deaths for each one million infections. As of 6/17/22, thirty-seven states have had greater than 500,000 total infections, and 36 states have had greater than 5,000 total deaths. Seventeen states (Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York, and California) have had greater than 69,000 deaths. California and Texas have each had greater than 88,000 deaths with California having 92,181 deaths (20th most deaths in the world).
As of 6/17/22, in the United States, 26.27% of the population has had a documented SARS-CoV-2 infection. In the last 18 months, 23.52% of our country became infected with SARS-CoV-2. On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. In the last 18 months, there were 778,134 new deaths from SARS-CoV-2. For fifteen of those months, vaccines have been available to all adults. During these fifteen months, 467,168 people have died of SARS-CoV-2 infections. Most of the hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 6/17/22, California was ranked 35th in the USA in infection percentage at 25.03%. In California, 21.06% of people were infected in the last 18 months. As of 6/17/22, 35 states have had greater than 25% of their population infected.
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Merck has developed the oral drug Molnupiravir, which induces RNA mutagenesis by viral RNA-dependent RNA polymerase of SARS-CoV-2 and other viruses. According to Kabinger et al, “Viral RNA-dependent RNA polymerase uses the active form of Molnupiravir, β-D-N4-hydroxycytidine triphosphate, as a substrate instead of cytidine triphosphate or uridine triphosphate. When the RNA-dependent RNA polymerase uses the resulting RNA as a template, β-D-N4-hydroxycytidine triphosphate directs incorporation of either guanine or adenine, leading to mutated (viral) RNA products. Analysis of RNA-dependent RNA polymerase–RNA complexes that contain mutagenesis products has demonstrated that β-D-N4-hydroxycytidine (the active form of Molnupiravir) can form stable base pairs with either guanine or adenine in RNA-dependent RNA polymerase explaining how the polymerase escapes proofreading and synthesizes mutated RNA” (quotation modified for clarity). The results of the phase 3 trial of Molnupiravir were published in the NEJM article “Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients” by Angélica Jayk Bernal, M.D. et al. (December 16, 2021 DOI: 10.1056/NEJMoa2116044). In this phase 3 study in the Molnupiravir group, 28 patients were hospitalized and one death occurred. In the placebo group, 53 patients were hospitalized and 9 died. Overall, 47% of hospitalizations and deaths were prevented by Molnupiravir. If you do a post hoc analysis and just look at deaths, Molnupiravir would prevent 89% of deaths. An Emergency Use Authorization by the FDA for Molnupiravir was approved on 12/24/21.The dose of Molnupiravir approved is four 200 mg capsules orally twice a day for five days. Diarrhea is reportedly a side effect in two percent of patients. I treated my first patient with Molnupiravir on 1/28/22. Currently more Molnupiravir is available weekly in the United States than PAXLOVID™ (see chart below; data from PHE.gov). Locally Molnupiravir is still available at CVS in Monterey (Fremont Blvd.; phone number: 831-375-5135) and CVS in Salinas (East Alisal Street; phone number 831-424-0026).
FDA Approved Intramuscular Prophylaxis of SARS-CoV-2 Immunocompromised Patients
Evusheld (from AstraZeneca) contains two human monoclonal antibodies, Tixagevimab (150 mg in 1.5 mL) and Cilgavimab (150 mg in 1.5 mL), in separate vials. According to the manufacturer, “Tixagevimab and Cilgavimab are two recombinant human IgG1κ monoclonal antibodies with amino acid substitutions to extend antibody half-life (YTE), reduce antibody effector function, and minimize the potential risk of antibody-dependent enhancement of disease (TM). Tixagevimab and Cilgavimab can simultaneously bind to non-overlapping regions of the receptor binding domain (RBD) of SARS-CoV-2 spike protein. Tixagevimab, Cilgavimab, and their combination bind to spike protein with equilibrium dissociation constants of KD = 2.76 pM, 13.0 pM and 13.7 pM, respectively, blocking its interaction with human ACE2, the SARS-CoV-2 receptor, which is required for virus attachment. Tixagevimab, Cilgavimab, and their combination blocked RBD binding to human ACE2 with IC50 values of 0.32 nM (48 ng/mL), 0.53 nM (80 ng/mL), and 0.43 nM (65 ng/mL), respectively.” Each monoclonal antibody is administered intramuscularly to immunocompromised patients in two separate injections every six months. Evusheld availability in California is limited and has been rationed/distributed by our local Public Health Department only to hospitals. Physicians in Monterey County who want to receive a distribution (or redistribution) of Evusheld need to be added to the list of eligible facilities by the State Therapeutics group. The first step is for the Monterey County EMS Agency (phone: 831-755-5713) to make a request to the State Therapeutics group to have the facility added to the system for further verification. Due to extremely limited availability, evidently the State Therapeutics group is currently only considering additions on a case by case basis. Physicians who wish to submit their facility for consideration will need to provide the following information to the Monterey County EMS Agency:
- Facility/Provider Name for Registration
- Provider Type (Hospital, Pharmacy, Etc)
- Shipping Address
- Contact Name(s)
- Contact Email(s)
- Contact Phone Number(s)
As for my immunocompromised patients: We provided this information by email to the Monterey County EMS Agency on 1/26/22 and will update you when or if we become an eligible provider and receive our first doses of Evusheld.
On 2/24/22, the FDA revised its dosing guidance for Evusheld, doubling the dosage of its two components, Tixagevimab and Cilgavimab, from 150 mg each to 300 mg each. They explain, “Based on the most recent information and data available, Evusheld may be less active against certain Omicron subvariants. The dosing regimen was revised because available data indicate that a higher dose of Evusheld may be more likely to prevent infection by the COVID-19 Omicron subvariants BA.1 and BA.1.1 than the originally authorized Evusheld dose.” Patients who have already received their first administration of Evusheld intramuscularly will need to contact their healthcare provider to get a second 150 mg injection of Tixagevimab and Cilgavimab. If you have not received Evusheld yet, the correct dose is 3 mL/300 mg of each monoclonal antibody injected intramuscularly. This large volume necessitates administration of the antibodies in the gluteus, with two separate injections.
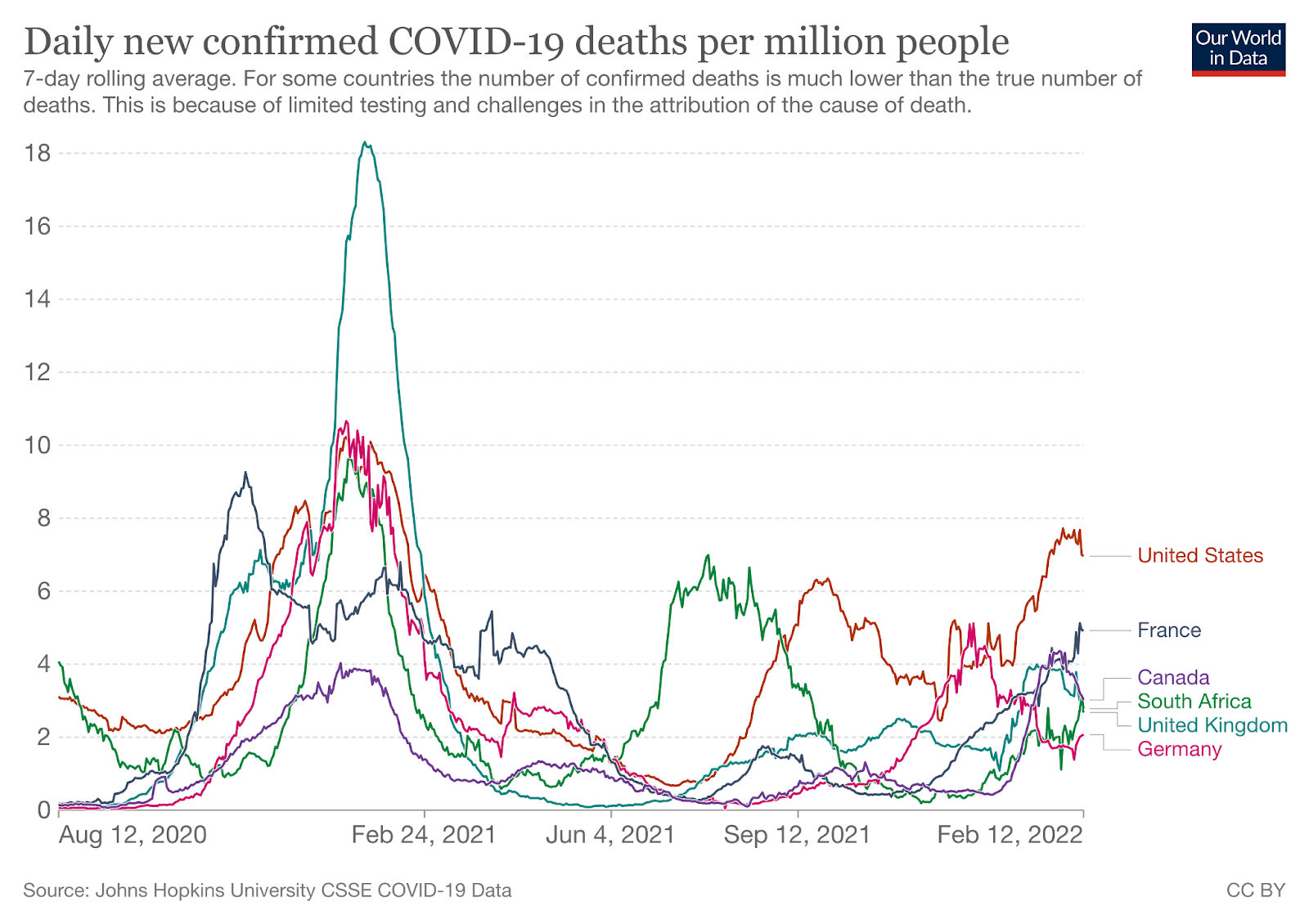
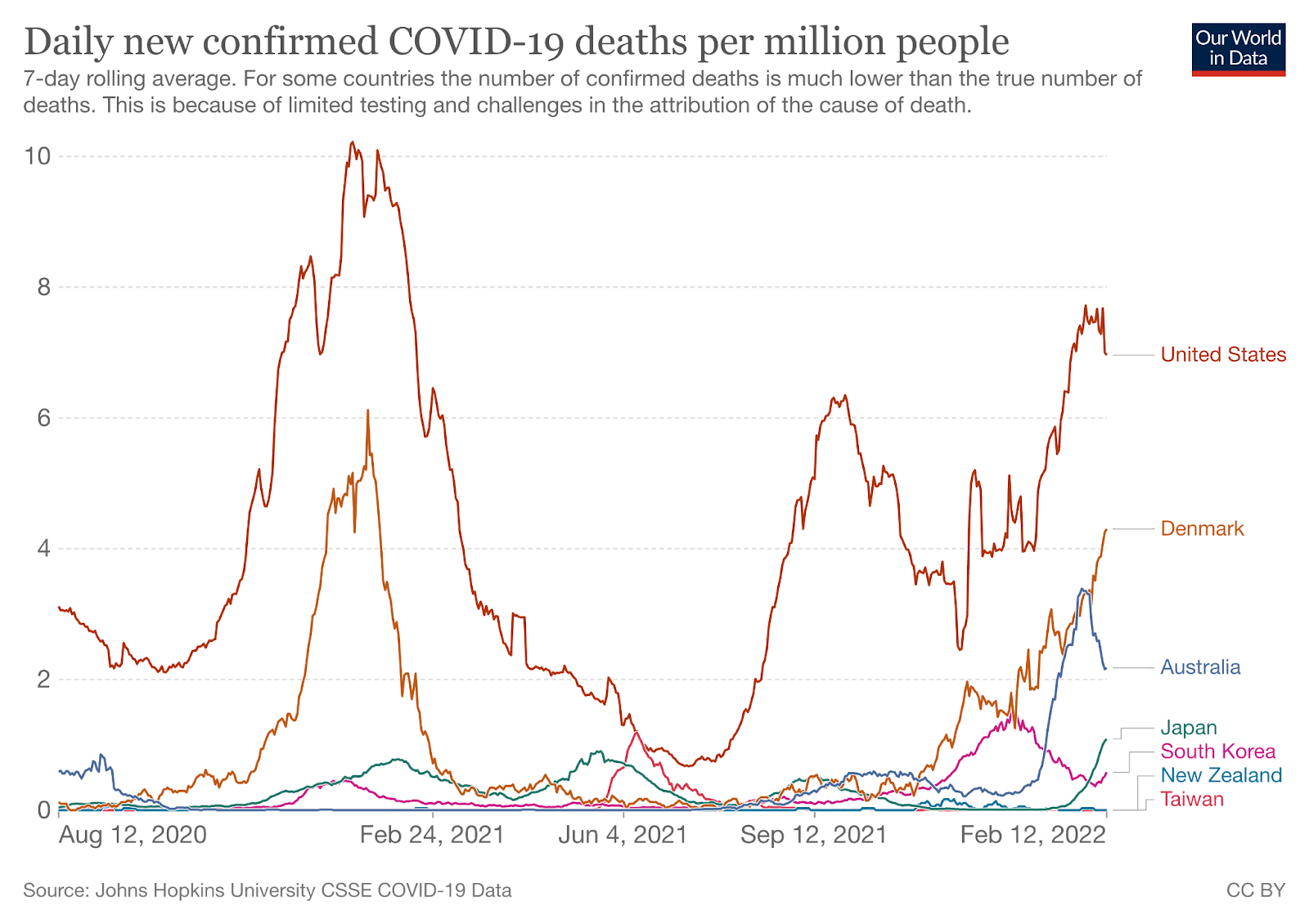
Watching World Data
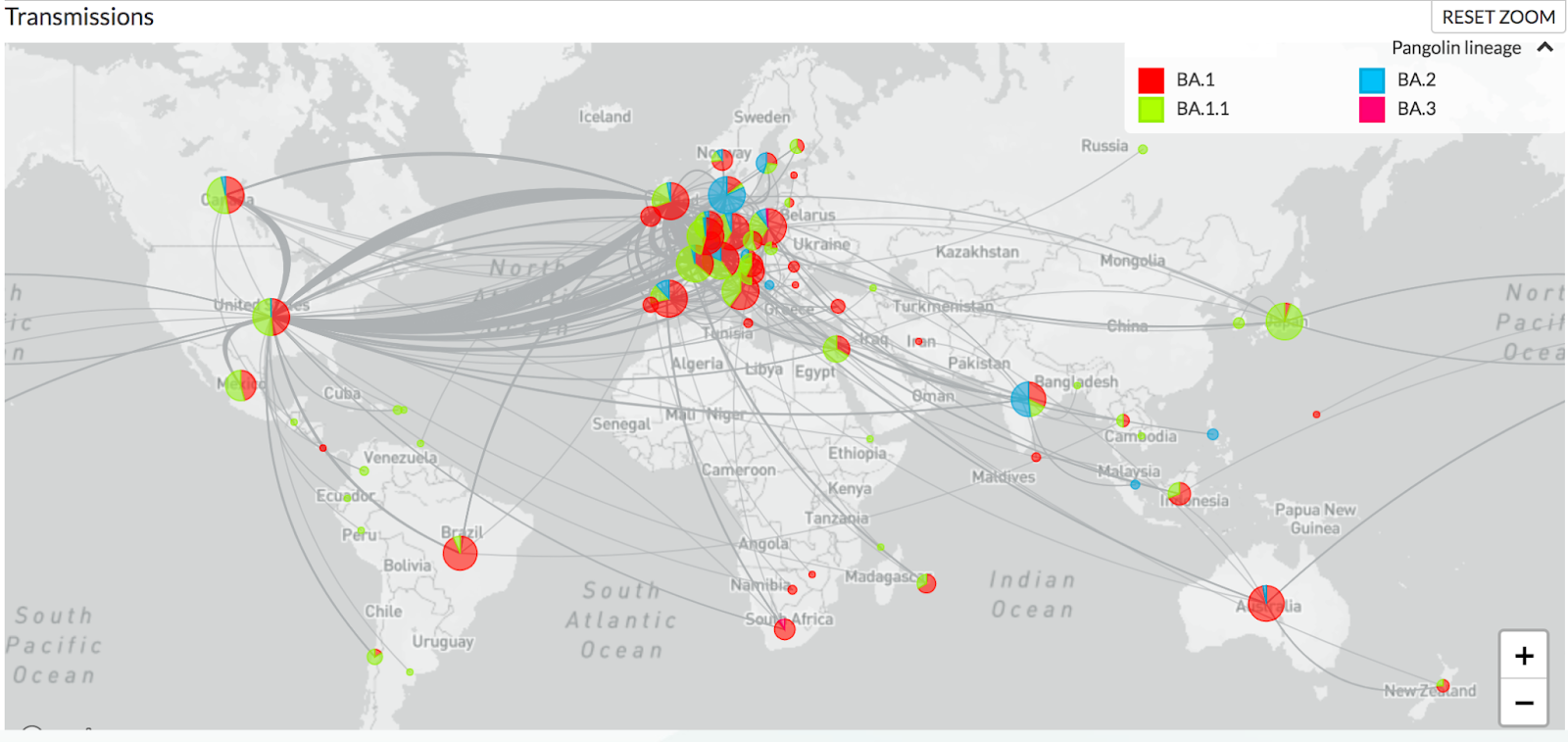
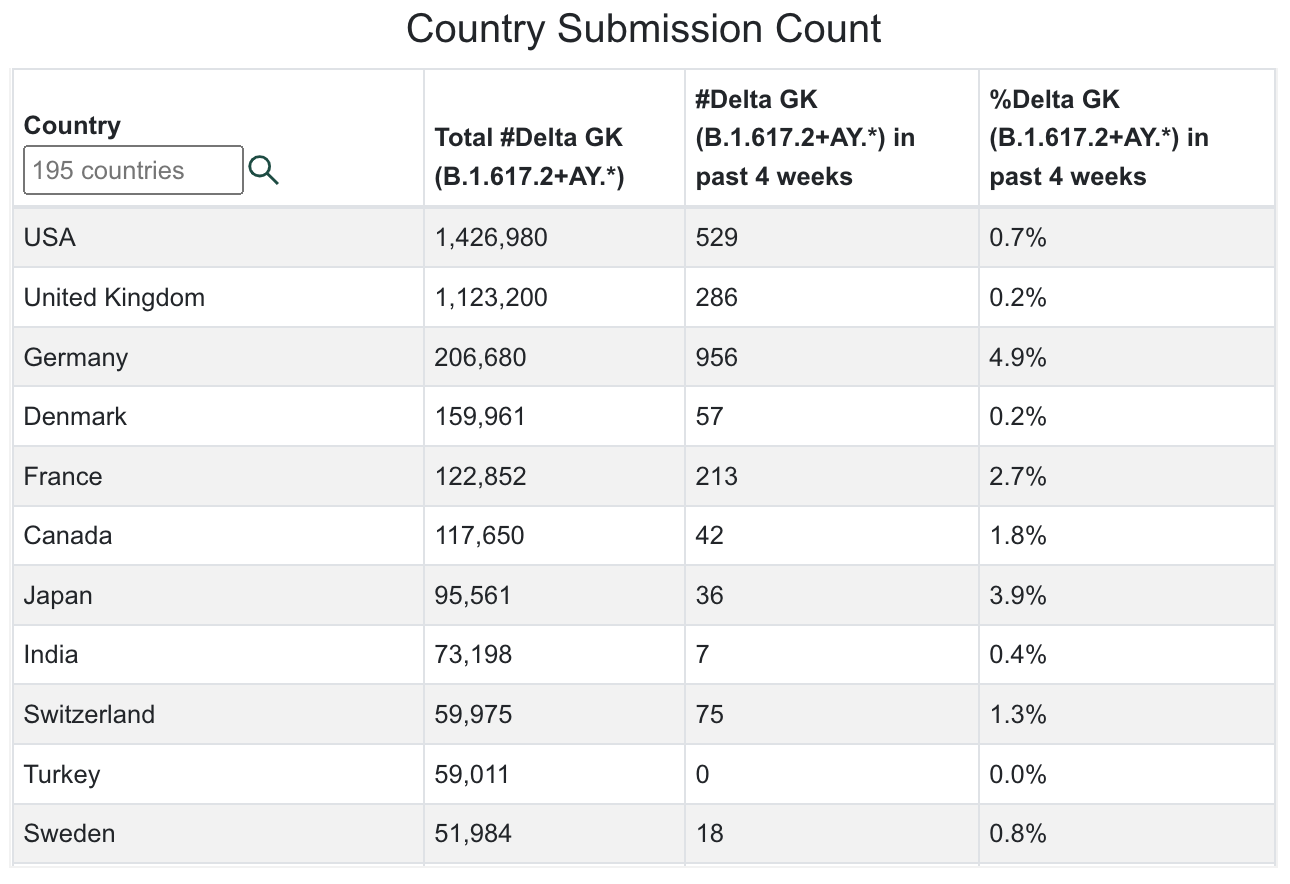
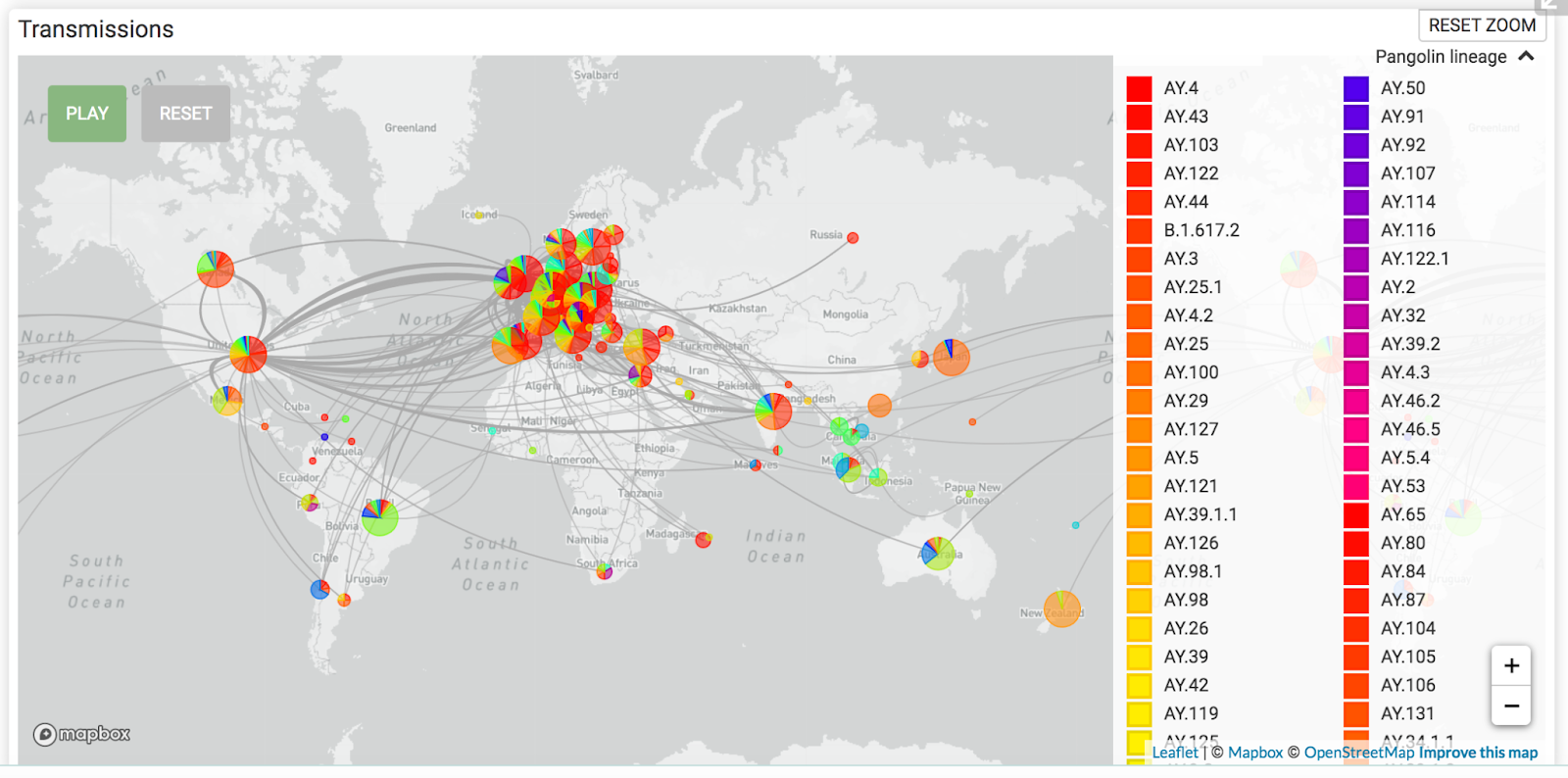
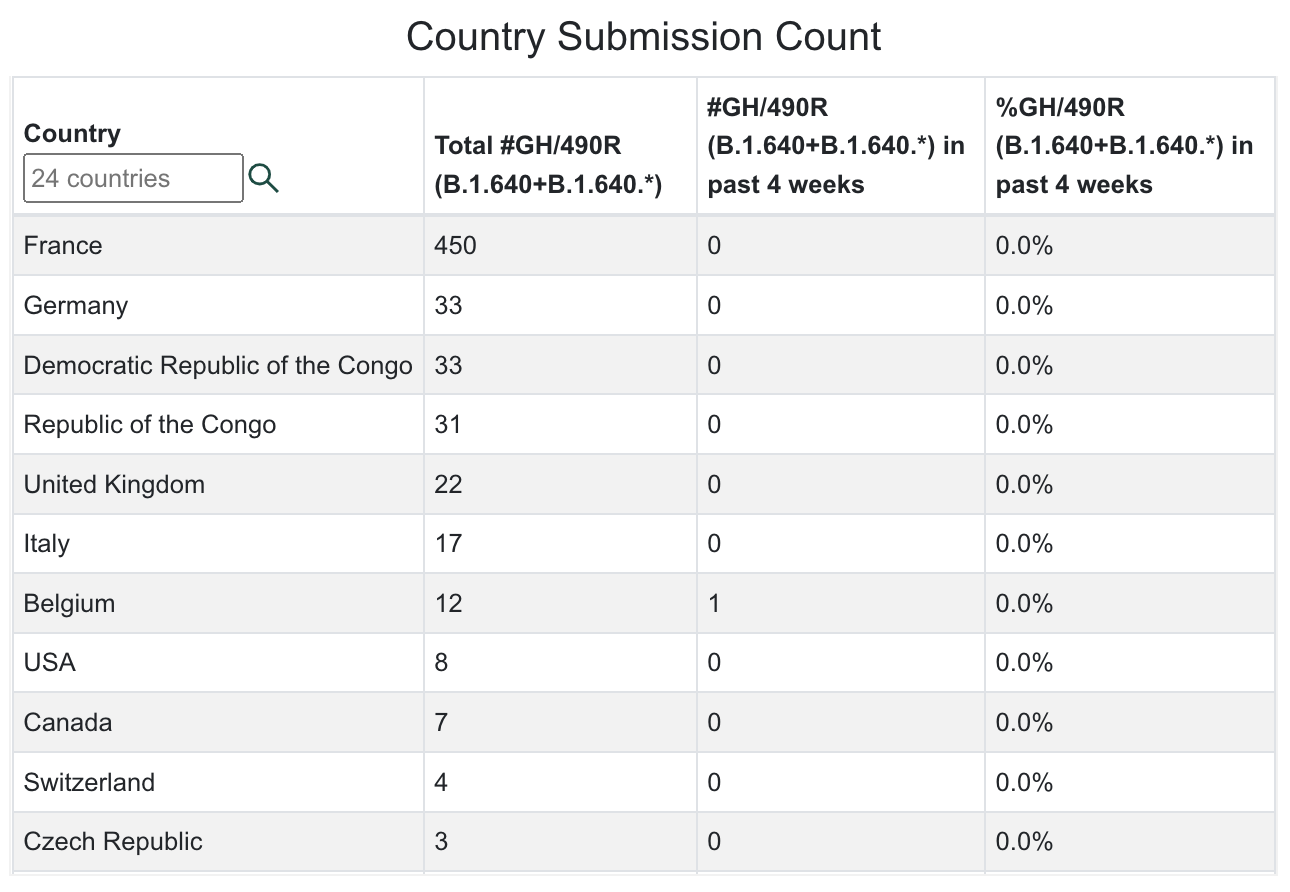
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
| Location | Total Infections as of 6/17/22 | New Infections on 6/17/22 | Total Deaths | New Deaths on 6/17/22 | % of Pop.Infected | SARS-CoV-2 Isolates Currently Known in Location | National/ State Mask Mandate | Currently in Lockdown |
| World | 543,620,349(8,989,675 new infections in 14 days). | 497,265 | 6,339,387(20,374 new deaths in last 14 days) | 1,091 | 6.97% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| USA | 87,968,819(ranked #1) 1,518,216 new infections in the last 14 days. | 81,733(ranked #1) 21 states failed to report infections. | 1,038,265(ranked #1) 4,896 new deaths in the last 14 days. | 200 32 states failed to report deaths. | 26.27% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| Brazil | 31,673,375(ranked #3) 535,896 new infections in the last 14 days. | 28,672 (ranked #6) | 668,968(ranked #2; 1,949 new deaths in 14 days) | 76 | 14.69% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| India | 43,283,793(ranked #2); 101,921 new infections in 2 weeks. | 13,216 | 524,840(ranked #3) | – | 3.07% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| United Kingdom | 22,472,503(ranked #6) 166,610 new infections in 2 weeks. | 12,054 | 179,537 (ranked #7) | 65 | 32.76% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| California, USA | 9,892,097(ranked #13 in the world; 233,150 new infections in the last 14 days). | 14,603 | 92,181 (ranked #20 in world) | 45 | 25.03% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| Mexico | 5,852,596(ranked #21) 70,191 new infections in 14 days). | 9,406 | 325,340(ranked #5) | 69 | 4.48% | B2 lineageAlpha/B.1.1.7 (UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| South Africa | 3,984,646(ranked #30; 19,224 new infections in 14 days). | 971 | 105,589 (ranked #18) | 5 | 6.55% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.2.12.1BA.4 (South Africa)BA.5 (South Africa) | No | No |
| Canada | 3,910,211(ranked #32) 30,111 new infections in 14 days). | 782 | 41,723(ranked #25) | 6 | 10.18% . | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Poland | 6,010,919 (ranked #20; 2,724 new infections in 14 days). | 48 | 116,390 (ranked #15) | – | 15.91% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3 | No | No |
| Turkey | 15,085,742(ranked #10, 12,995 new infections in 14 days). | ———— | 98,996 (ranked #19) | ——— | 17.51% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Russia | 18,391,797(ranked #7), 47,833 new infections in 14 days). | 3,373 | 380,333(ranked #4 in world) | 63 | 12.59% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)R1 (Japan) B.1.640.1 (Congo/France)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Argentina | 9,313,453(ranked #13; 82,880 new infections in 14 days). | ———– | 128,984 (ranked #14) | ——– | 20.24% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gama/P.1 (Brazil)Delta/B.1.617.2 (India)Lambda/C.37 (Peru)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Colombia | 6,131,657(ranked #18, 26,642 new infections in 14 days). | – | 139,908 (ranked #13) | – | 11.80% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Epsilon/B.1.427 + B.1.429 (USA)*Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Peru | 3,596,374(ranked #35, 12,974 new infections in 14 days). | 1,400 | 213,374(ranked #6) | 13 | 10.61% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Iran | 7,234,523(ranked 17th; 1,909 new infections in last 14 days) | 156 | 141,361(ranked #11) | 1 | 8.40% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Spain | 12,563,399(ranked 11th; 160,154 new infections in 14 days). | 16,090 | 107,482 (ranked #17) | 81 | 26.85% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| France | 30,079,458 (ranked #4; 483,566 new infections in the last 14 days). | 50,605 (ranked #3) | 149,039 (ranked #10) | 43 | 45.88% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant | No | No |
| Germany | 27,124,459(ranked #5; 613,531 new infections in 14 days.). | 28,471 (ranked #7) | 140,292 (ranked #12) | – | 32.17% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| South Korea | 18,263,643 (ranked #8 121,808 new infections in 14 days). | 7,186(ranked #17) | 21,416 (ranked #39) | 9 | 35.56% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Vietnam | 10,736,408 (ranked #12; 12,735 new infections in 14 days). | 723 | 43,083 (ranked #24) | – | 10.83% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Netherlands | 8,122,258 (ranked #15; 32,021 new infections in 14 days). | 3,855 | 22,343 (ranked #41) | 1 | 47.19% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Denmark | 2,996,713 (ranked #39) 10,405 new infections in 14 days | 995 | 6,421 (ranked #81) | – | 51.38% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| North Korea (DPRK) | 4,581,420 (ranked #24; 663,840 new infections in 14 days) | 23,160 (ranked #8) | 73 | – | 17.62% | Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Taiwan | 3,190,746(ranked #38) | 55,220 (ranked #2) | 4,868 (ranked #89) | 154 (ranked #2) | 13.34% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Japan | 9,108,323(ranked #14) | 15,802(ranked #10) | 30,980(ranked #31) | 17 | 7.24% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
What Our Team Is Reading This Week
- Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2 (The Lancet) https://doi.org/10.1016/S0140-6736(22)00941-2
- Antibody escape of SARS-CoV-2 Omicron BA.4 and BA.5 from vaccine and BA.1 serum (Cell) https://doi.org/10.1016/j.cell.2022.06.005
- Immunomodulatory treatment in postural tachycardia syndrome: A case series (European Journal of Neurology) https://doi.org/10.1111/ene.14711
- Long COVID-19 Liver Manifestation in Children (JPGN) https://journals.lww.com/jpgn/abstract/9900/long_covid_19_liver_manifestation_in_children.84.aspx
- Cross-reactive immunity against the SARS-CoV-2 Omicron variant is low in pediatric patients with prior COVID-19 or MIS-C (Nature Communications) https://doi.org/10.1038/s41467-022-30649-1
- C.D.C. Dismisses Airborne Transmission of Monkeypox. Some Experts Disagree. (NY Times) https://www.nytimes.com/2022/06/10/health/monkeypox-airborne.html
- Omicron BA.1 breakthrough infection drives cross-variant neutralization and memory B cell formation against conserved epitopes (Science Immunology) https://doi.org/10.1126/sciimmunol.abq2427
- SARS-CoV-2 Infection and Persistence Throughout the Human Body and Brain (National Institutes of Health) https://videocast.nih.gov/watch=45296?jwsource=twi
- Long COVID is associated with extensive in-vivo neuroinflammation on [18F]DPA-714 PET (Preprint) https://doi.org/10.1101/2022.06.02.22275916
- Unexpected worsening of progressive multifocal leucoencephalopathy following COVID-19 pneumonia (Journal of Neurovirology) https://doi.org/10.1007%2Fs13365-021-00980-2
- Virological characteristics of the novel SARS-CoV-2 Omicron variants including BA.2.12.1, BA.4 and BA.5 (Preprint) https://doi.org/10.1101/2022.05.26.493539
- During the Omicron Wave, Death Rates Soared for Older People (NY Times with CDC data) https://www.nytimes.com/2022/05/31/health/omicron-deaths-age-65-elderly.html
- PD-1 blockade counteracts post–COVID-19 immune abnormalities and stimulates the anti–SARS-CoV-2 immune response (JCI Insight) https://insight.jci.org/articles/view/146701
- Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance (Nature Reviews Clinical Oncology) https://doi.org/10.1038/s41571-019-0218-0
- Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study (Observational Research) https://doi.org/10.1007/s00296-022-05146-9
- An early warning system for emerging SARS-CoV-2 variants (Nature Medicine) https://doi.org/10.1038/s41591-022-01836-w
- SARS-CoV-2 Omicron Variant is as Deadly as Previous Waves After Adjusting for Vaccinations, Demographics, and Comorbidities (Preprint) https://doi.org/10.21203/rs.3.rs-1601788/v1
- Partial ORF1ab Gene Target Failure with Omicron BA.2.12.1 (Preprint) https://www.medrxiv.org/content/10.1101/2022.04.25.22274187v1
- COVID-19 Associated Hepatitis in Children (CAH-C) during the second wave of SARS-CoV-2 infections in Central India: Is it a complication or transient phenomenon. (Preprint) https://doi.org/10.1101/2021.07.23.21260716
- Liver and Gastrointestinal Involvement in Patients With COVID-19: A Retrospective Study https://www.cureus.com/articles/90062-liver-and-gastrointestinal-involvement-in-patients-with-covid-19-a-retrospective-study
- Cortical Grey Matter Volume Loss links to Neurological Sequelae in post COVID-19 “Long Haulers” (Preprint) https://doi.org/10.21203/rs.3.rs-1582065/v1
- Virological characteristics of the SARS-CoV-2 Omicron BA.2 spike (Cell) https://doi.org/10.1016/j.cell.2022.04.035
- Continued Emergence and Evolution of Omicron in South Africa: New BA.4 and BA.5 lineages https://www.krisp.org.za/manuscripts/MEDRXIV-2022-274406v1-deOliveira.pdf
- Molecular consequences of SARS-CoV-2 liver tropism (Nature Metabolism) https://doi.org/10.1038/s42255-022-00552-6
- China CDC shares latest COVID-19 data (GISAID) https://www.gisaid.org/resources/gisaid-in-the-news/china-shares-latest-11-apr-2022/#c920
- Persistent COVID-19 symptoms in a community study of 606,434 people in England (Nature) https://www.nature.com/articles/s41467-022-29521-z
- Brain Inflammation and Intracellular α-Synuclein Aggregates in Macaques after SARS-CoV-2 Infection (Viruses) https://www.mdpi.com/1999-4915/14/4/776
- Antibody Resistance of SARS-CoV-2 Omicron BA.1, BA.1.1, BA.2 and BA.3 Sub-lineages (Preprint) https://www.biorxiv.org/content/10.1101/2022.04.07.487489v1
- Infectious viral load in unvaccinated and vaccinated individuals infected with ancestral, Delta or Omicron SARS-CoV-2 (Nature Medicine) https://www.nature.com/articles/s41591-022-01816-0
- Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain (Preprint) https://www.biorxiv.org/content/10.1101/2022.01.07.475453v1
- Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: nationwide self-controlled cases series and matched cohort study (BMJ) https://www.bmj.com/content/377/bmj-2021-069590
- SARS-CoV-2 Infection Induces Ferroptosis of Sinoatrial Node Pacemaker Cells (Circulation Research) https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.320518
- SARS-CoV-2 variants of concern and variants under investigation in England (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1063424/Tech-Briefing-39-25March2022_FINAL.pdf
- Neutralization of Omicron BA.1, BA.2, and BA.3 SARS-CoV-2 by 3 doses of BNT162b2 vaccine (Preprint) https://doi.org/10.1101/2022.03.24.485633
- COVID-19-Associated Encephalitis: Two Case Reports https://www.cureus.com/articles/86903-covid-19-associated-encephalitis-two-case-reports
- First evidence that an emerging mammalian alphacoronavirus is able to infect an avian species (Transboundary and Emerging Diseases) https://doi.org/10.1111/tbed.14535
- SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses (The Lancet) https://doi.org/10.1016/S0140-6736(22)00383-X
- Evidence for SARS-CoV-2 Delta and Omicron co-infections and recombination (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.09.22272113v1
- Culture and identification of a “Deltamicron” SARS-CoV-2 in a three cases cluster in southern France (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.03.22271812v1.full
- Mandatory masking in schools reduced COVID-19 cases during Delta surge (NIH press release) https://www.nih.gov/news-events/news-releases/mandatory-masking-schools-reduced-covid-19-cases-during-delta-surge
- School Masking Policies and Secondary SARS-CoV-2 Transmission (Pediatrics) https://publications.aap.org/pediatrics/article/doi/10.1542/peds.2022-056687/185379/School-Masking-Policies-and-Secondary-SARS-CoV-2
- Transmission of SARS-CoV-2 delta variant (AY.127) from pet hamsters to humans, leading to onward human-to-human transmission: a case study (The Lancet) https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00326-9/fulltext
- COVID-19 Variant Dashboard – USA by Raj Rajnarayanan https://public.tableau.com/app/profile/raj.rajnarayanan/viz/USAVariantDB/VariantDashboard





You must be logged in to post a comment.