
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.

SARS-CoV-2 infections and deaths per day had been decelerating at a rapid rate in the United States. The rate of decline has lessened as the increased infection rate and infectivity of the Omicron BA.1 variant of SARS CoV-2. The outbreak is still caused by variants of concern Omicron BA.1.1, BA.1, BA.2 and to a lesser degree BA.3 (particularly in Poland). Omicron variants are at least four times as infectious as the already highly infectious Delta variants. UK scientists have found that the household secondary attack rate for Omicron is 21.6%, compared to 10.7% with Delta, meaning people infected with Omicron are twice as likely to infect household members as they would be if infected with Delta. They also estimate a “three- to eight-fold increased risk of reinfection with the Omicron variant.”
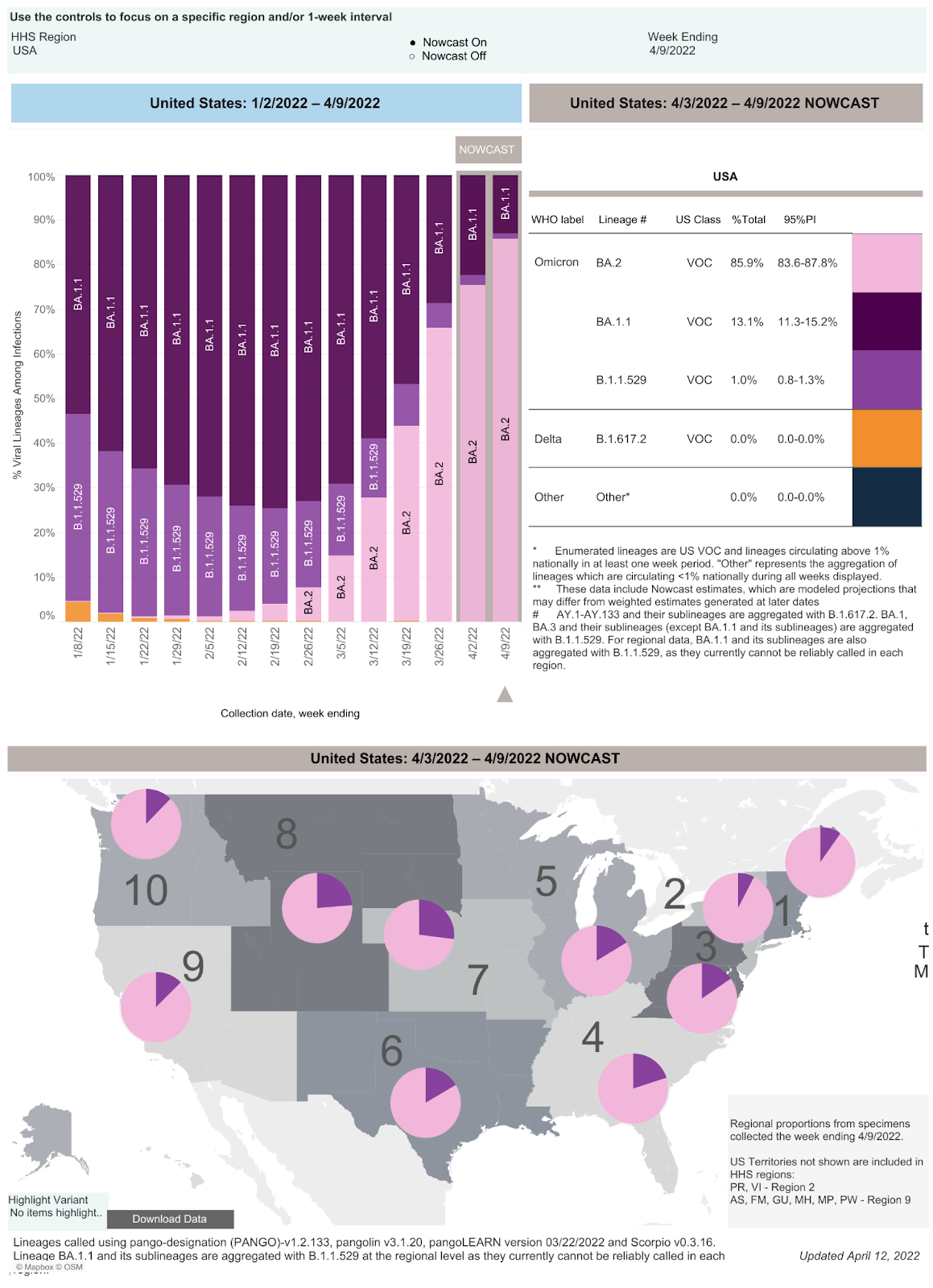
I would expect the Omicron variant to continue to mutate just like Delta. There are now already 63 Omicron sub-variants that have been assigned Pango lineages, including 18 sub-lineages of BA.2, which is rapidly spreading in the United States and makes up greater than 85.9% of isolates as of 4/9/22, according to the CDC.
An additional problem may be the development of recombinant SARS-CoV-2 isolates. A recombinant isolate occurs when two isolates infect the same cell and, in the process of viral reproduction, exchange nucleic acids, creating a new isolate that is a recombination of parts from the genomes of both isolates. A recombinant isolate of Delta AY.4.2.2 and Omicron BA.1.1 was recently reported in the UK. As of 3/25/22 four different recombinant variants of SARS-CoV-2 have been reported by the UK Health Security Agency.
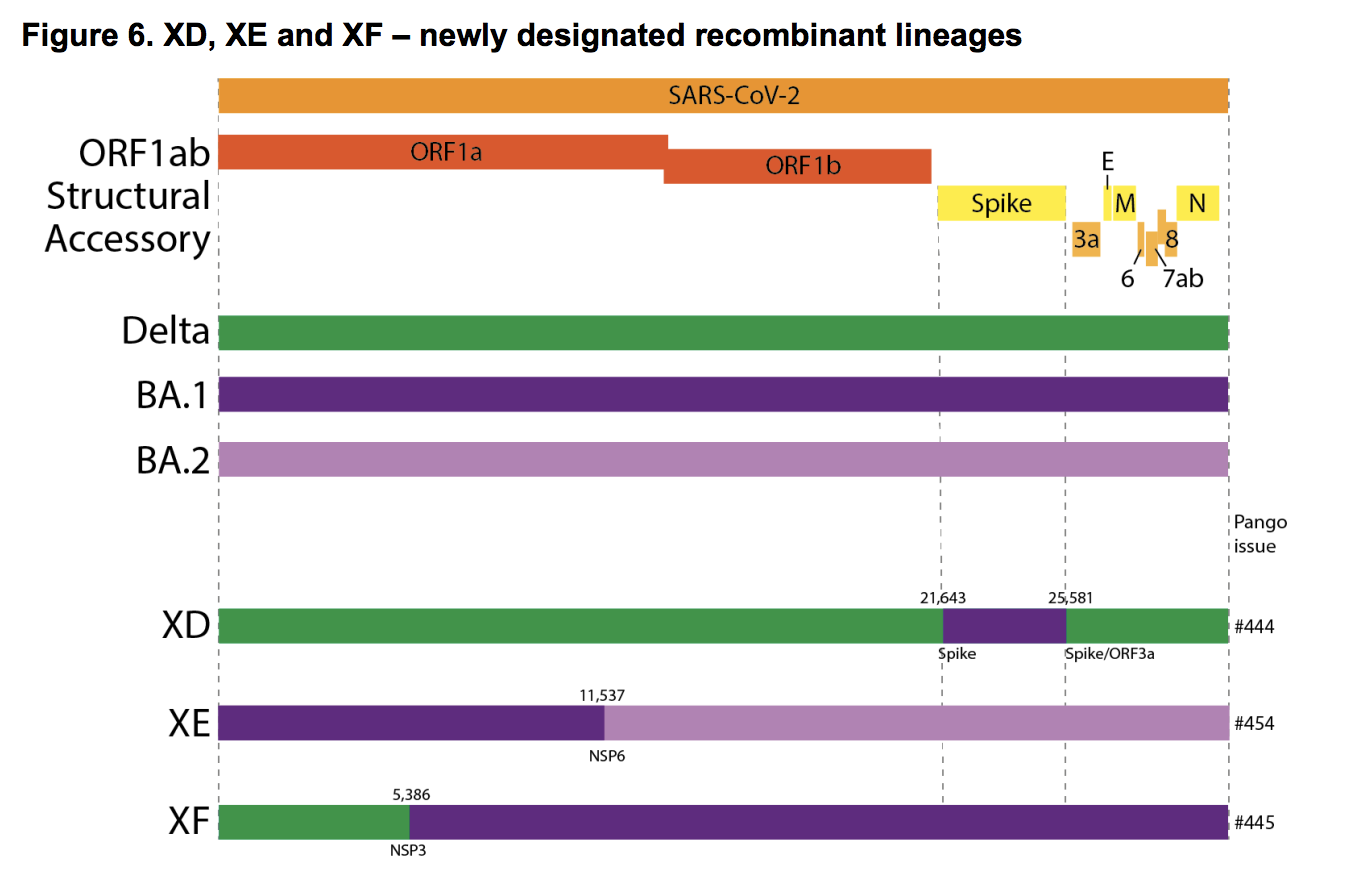
According to the UK Health Security Agency’s Technical Briefing from 3/25/22: “There are currently 3 recombinant lineages being monitored as part of horizon scanning: XD, XE, and XF (Figure 6). XD and XF are Delta and BA.1 recombinants. XE is a BA.1 and BA.2 recombinant and has 3 mutations that are not present in all BA.1 or BA.2 sequences: NSP3 C3241T and V1069I, and NSP12 C14599T. XF and XE are associated with UK sequenced samples. XD is predominantly associated with France. XD contains the unique mutation NSP2:E172D.”
As of 4/5/22 the UK Health Security Agency reports 1,179 sequences of the XE recombinant in the UK data. The figure below shows a breakdown of XE data by gender and age group. We can see there were more XE infections in children and young adults than there were in the 70+ age groups.

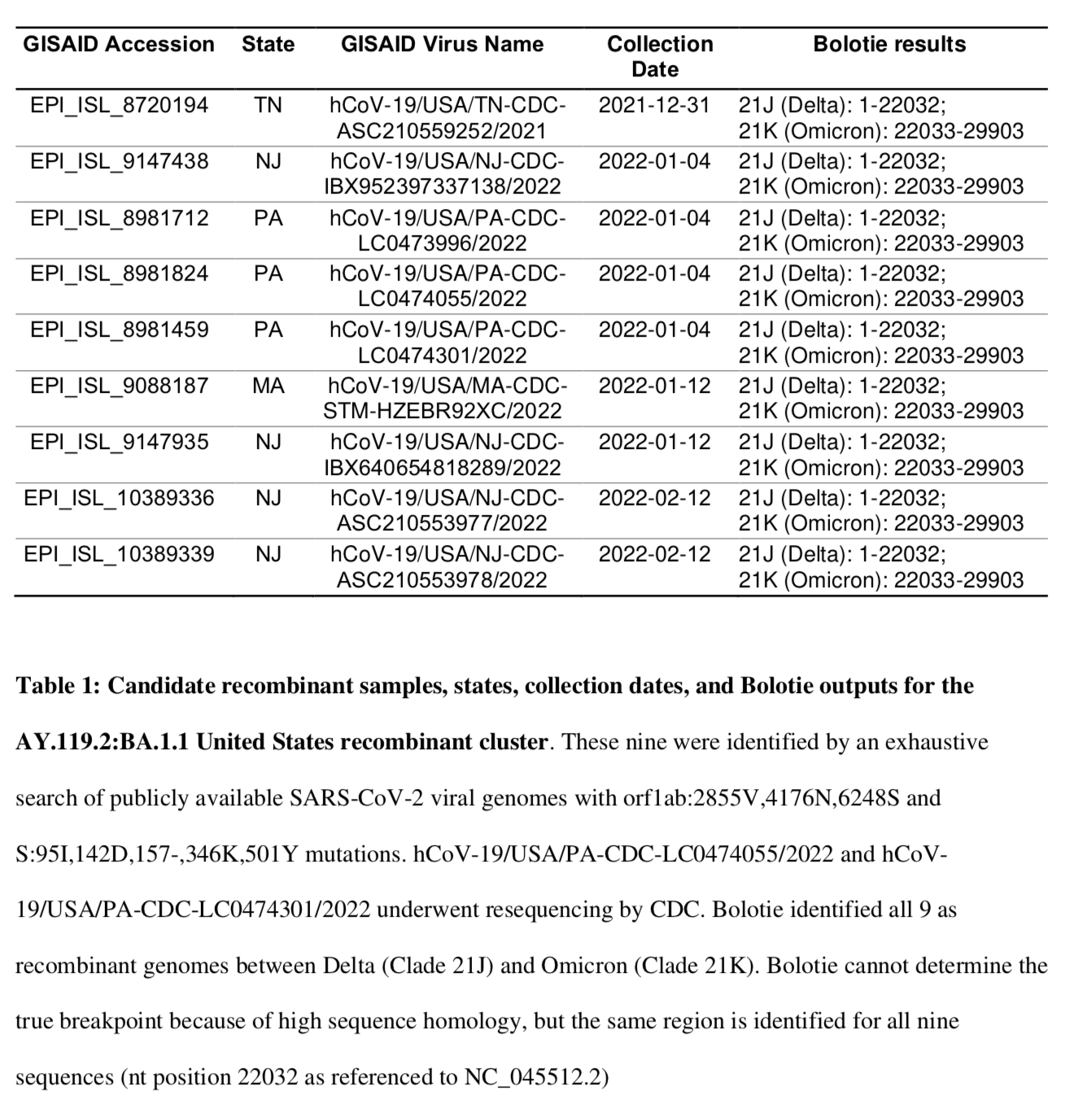
The US recombinant isolate, Delta AY.119.2-Omicron BA.1.1, has a Omicron spike sequence from amino acid 158 through amino acid 339 and was recently found in four states (Tennessee [original isolate 12/31/21], Pennsylvania [3 isolates], New Jersey [4 isolates] and Massachusetts [one isolate]; see table below.)
We do not know yet whether any recombinant isolates will rapidly spread or have enhanced morbidity and mortality.
We expect to see additional Omicron variants, recombinant variants and probably new pandemic SARS- CoV-2 lineages as uncontrolled infection continues in multiple continents and countries.
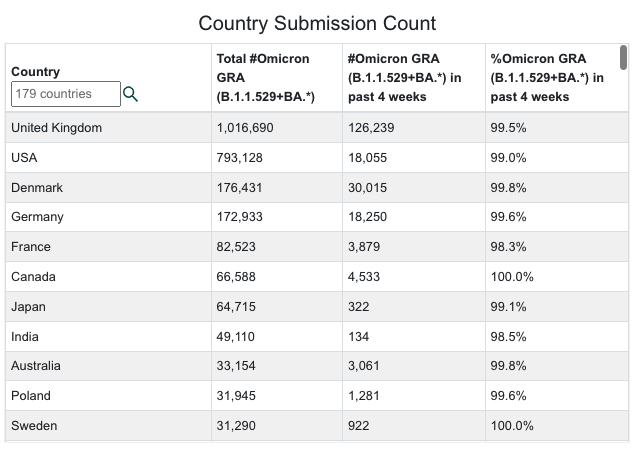
As of 3/27/21 the Omicron variants, which were first seen in South Africa on 11/08/21, are now in all 50 states, Puerto Rico and the District of Columbia. As of 4/10/22 Omicron has been identified on all seven continents and in at least 179 countries.
Omicron variants have mutations which decrease the effectiveness of current vaccines and monoclonal antibodies. The effectiveness of the new Pfizer drug, PAXLOVIDTM, should not be compromised by any of the current mutations in Omicron or Delta variants. Pfizer completed their filing with the FDA on 11/15/21. The FDA approved PAXLOVIDTM on December 22 , 2021.The FDA approved Merck’s drug Molnupiravir on December 23, 2021. On 12/23/21 CVS announced by fax it was selected by the Government to distribute oral PAXLOVIDTM and Molnupiravir. On 12/27/21, another fax from CVS listed which CVS pharmacies in California would have these drugs. Monterey County covers 3,771 square miles with a population of 434,061. Three CVS pharmacies in Monterey, Salinas, and Soledad are the only listed pharmacies in our county. I have now been able to obtain PAXLOVIDTM for infected patients from the CVS in Salinas (phone 831-424-0026), the CVS on Fremont Street in Monterey (phone 831-375-5135) and the CVS in Soledad in south Monterey County (phone 831-678-5110). All require electronic prescriptions written as Paxlovid three tablets twice daily orally for five days (thirty total tablets). Physicians or their staff probably should call to check on drug availability that day.
In the absence of obtaining intravenous Sotrovimab or Bebtelovimab, only oral PAXLOVIDTM and Molnupiravir are available to treat SARS-CoV-2 as an outpatient. Our first Paxlovid failure in an immunocompromised patient was treated the week of 4/5/22 at the Community Hospital of the Monterey Peninsula (Montage) ER as an outpatient with a single one-minute intravenous injection of Bebtelovimab.
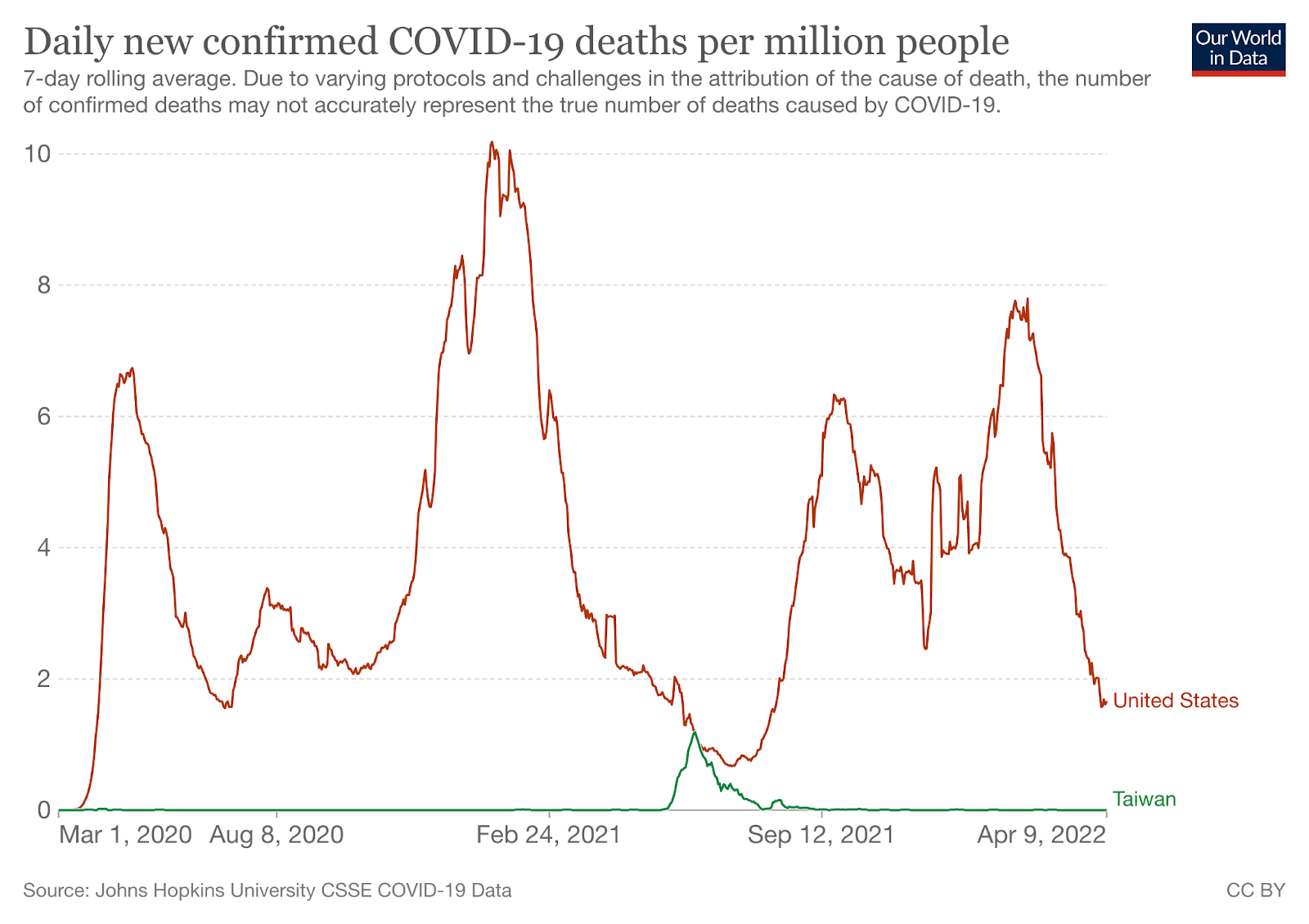
Vaccination will not prevent you from getting an Omicron variant infection. For now only masking (N95 rated masks, please!) and social distancing will have any effect on acquisition of infection with these variants. Furthermore, we do not believe that a 5-day quarantine or isolation period is sufficient for any COVID-19 infection. The Taiwanese CDC agrees with both our recommendations on quarantine period and masking. In fact, the Taiwanese CDC has recommended N95 masking since the beginning of the pandemic (and made these masks universally available to their population). Taiwan has one of the lowest death rates per million during the course of the pandemic (see graph below).
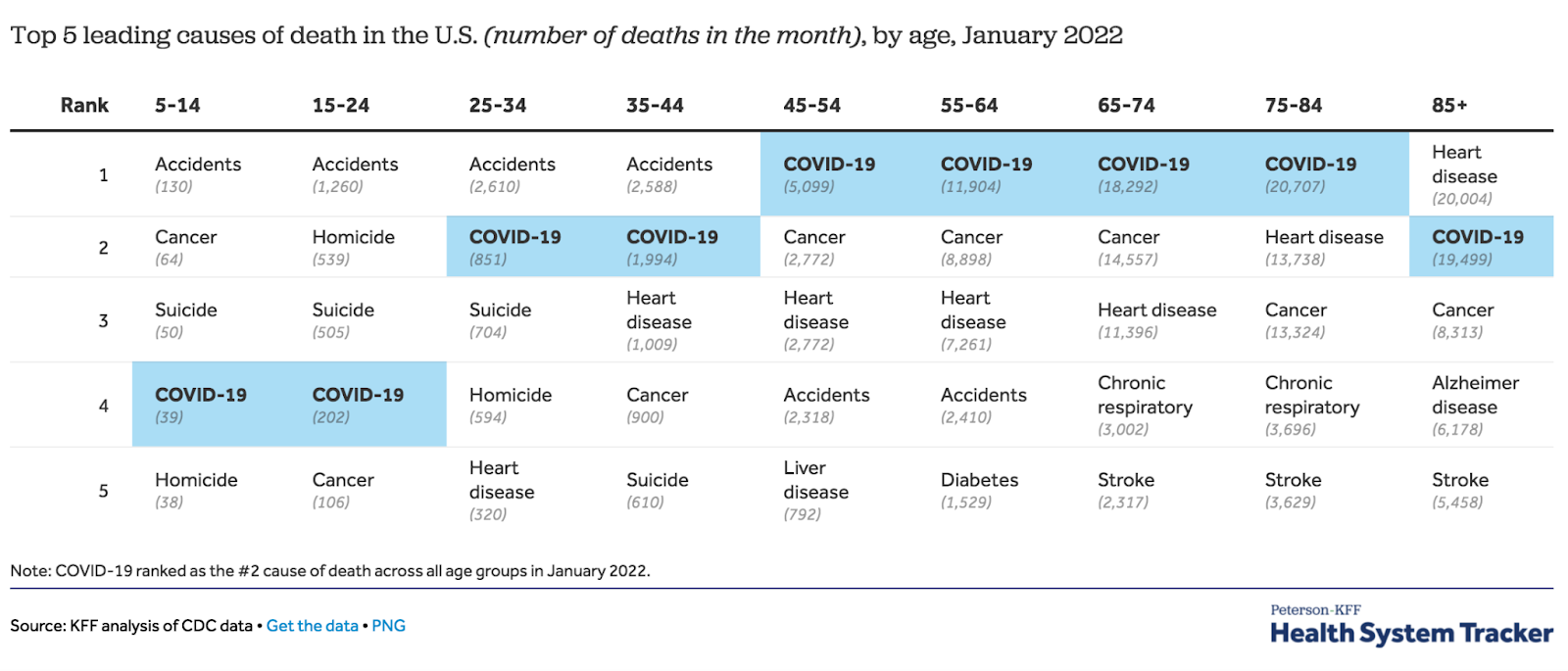
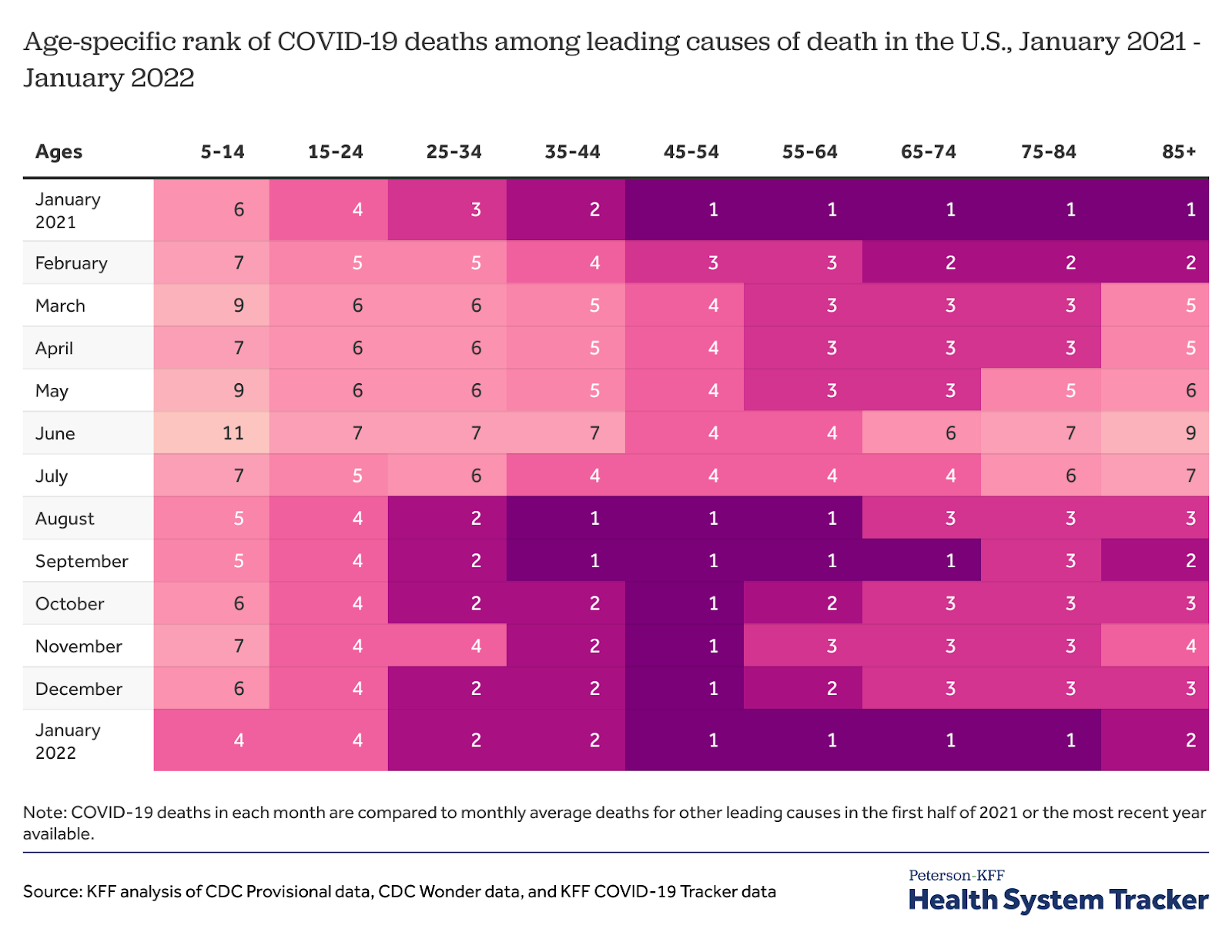
According to a KFF analysis of CDC data, in January 2022, SARS-CoV-2 was in the top four causes of death in the United States for all age groups, including children. It was the number one cause of death in people aged 45-84.
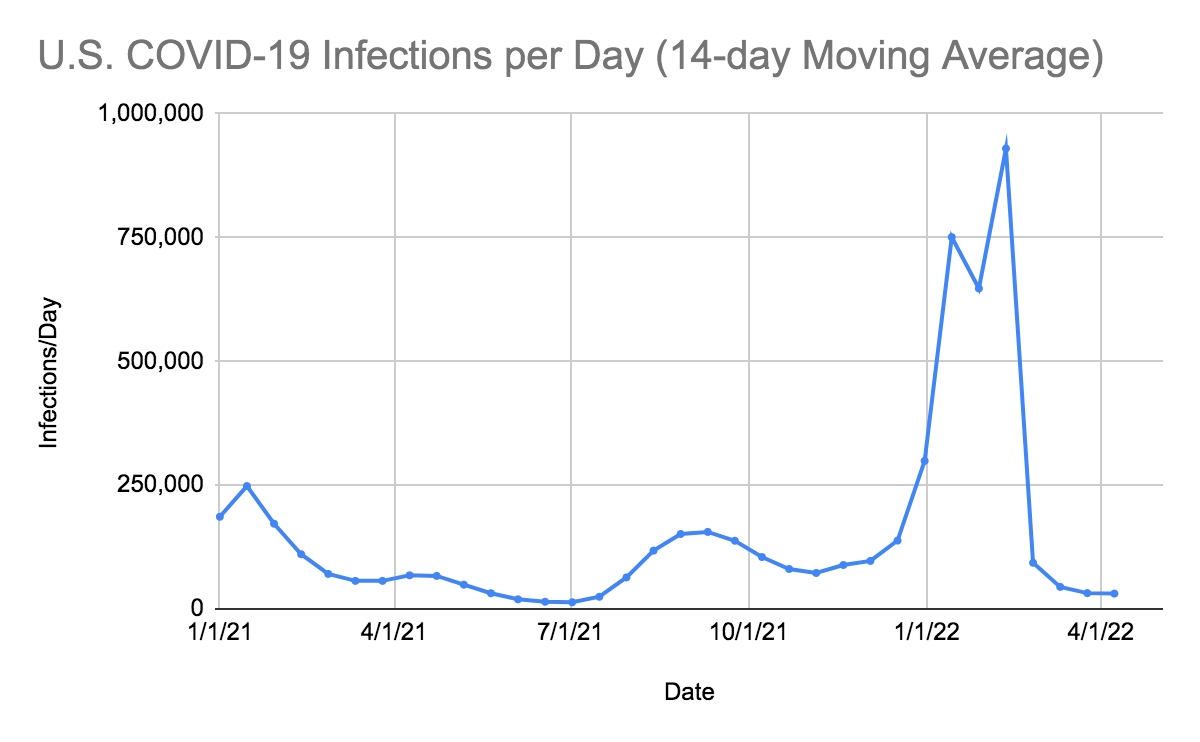
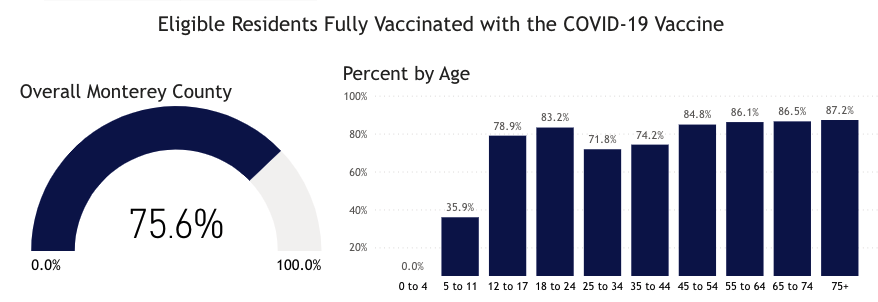
In the last 14 days, the number of infections has decreased by 873 infections per day compared to the preceding 14-day period. Our infections per day have decreased for the fourth time in the last 14 weeks. Unless people get vaccinated, including their third dose of the vaccine, we will see further spread of the Omicron variants and increase in deaths in people who are not vaccinated, have waning immunity, the immunocompromised population and others with risk factors particularly those older than over the age of 64. Anyone over the age of 5 years can now get vaccinated in the United States at no cost. This should get done immediately. In Monterey County, as of 4/10/22, only 35.9% of 5-11 year-olds have received the first two doses of vaccine, while 78.9% of 12-17 year-olds have received two doses.
Omicron Subvariant BA.2 Is Here and Dominant
Per CDC data ending in 4/9/22, the Delta variant accounted for 0.0% of new infections in the United States, while Omicron BA1.1 accounted for 13.1%, Omicron B.1.1.529 accounts for 1.0%, and Omicron subvariant BA.2 accounted for 85.9%. It’s worth noting that in the last 30 days, according to GISAID, the United States has only sequenced 3.67% of cases.
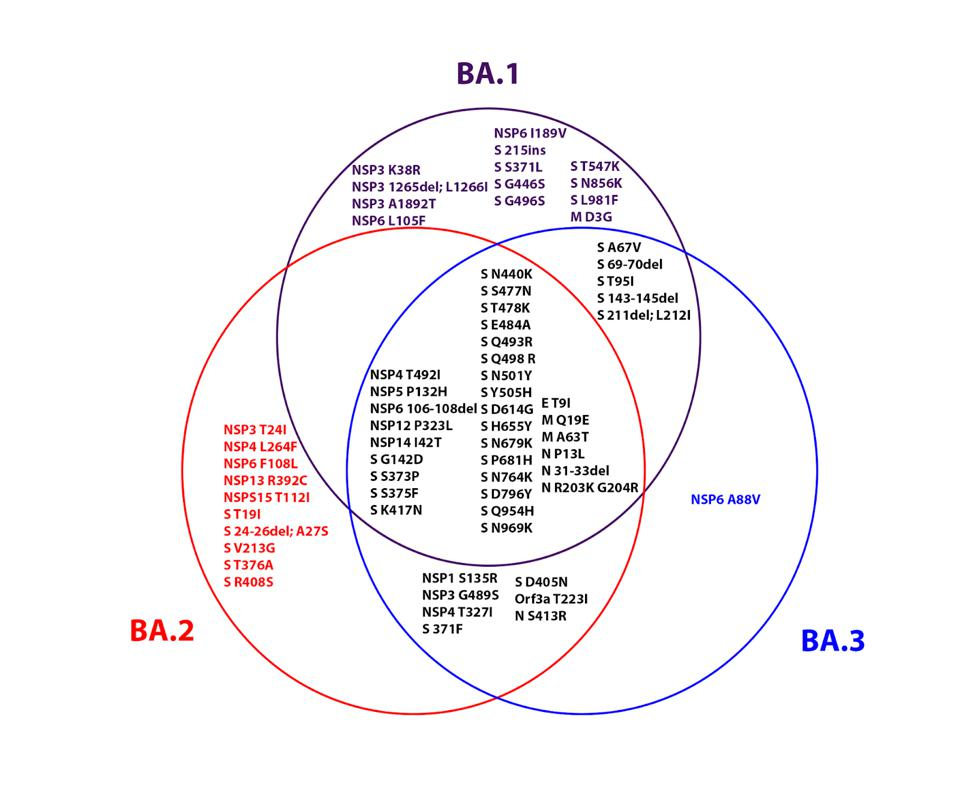
and differences between the three Omicron family viruses. ACCESS HEALTH INTERNATIONAL
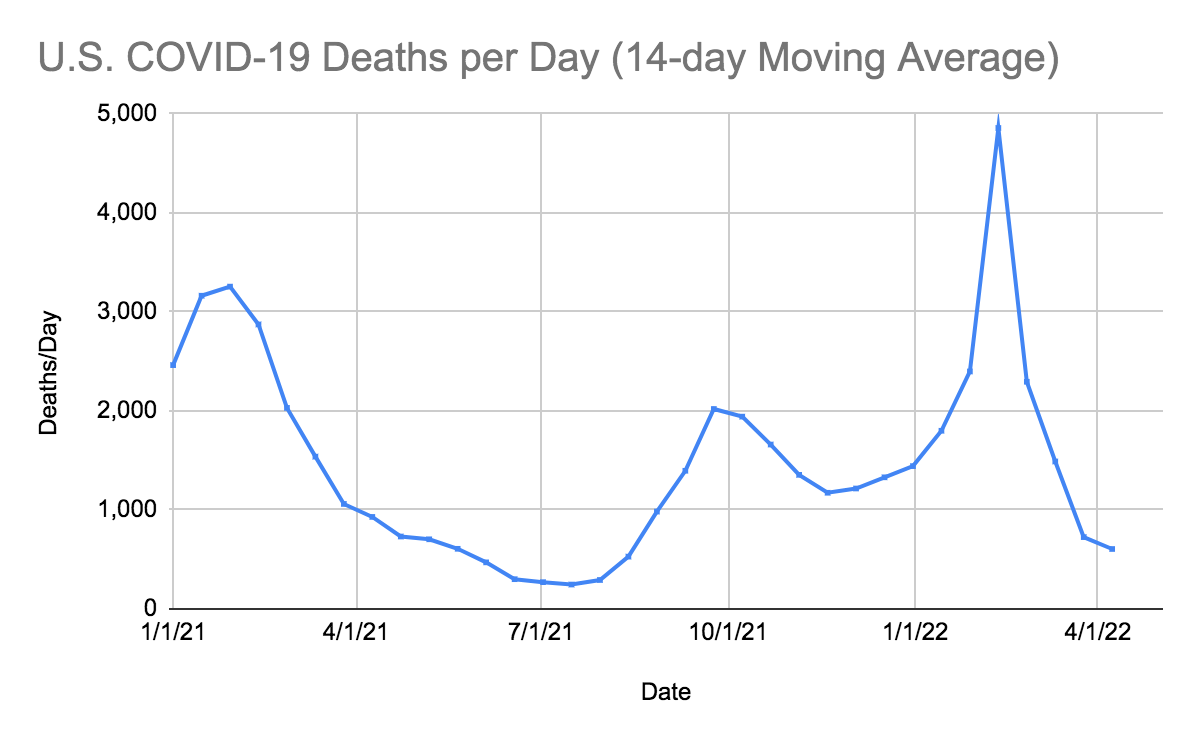
On 4/8/22, the United States had 35,285 new infections. There were also 404 deaths. In the United States the number of hospitalized patients has been decreasing in many areas, and now only 1,716 patients are seriously or critically ill; that number was 2,548 two weeks ago. The number of critically ill patients has decreased by 832 in the last 14 days, while at least 8,467 new deaths occurred (a decrease of 1,587 deaths from the previous 14 days). The number of critically ill patients has decreased for the sixth time in eighteen 14-day periods. Patients are still dying each day (average 605/day). Omicron BA.2 infections should continue to increase but critically ill patients, and deaths may continue to decrease in the next two weeks if Omicron BA.2 continues to cause less severe disease and does not infect large numbers of previously BA.1 infected patients. There have already been reports out of Israel of patients infected with BA.1 being later reinfected with BA.2.
As of 4/08/22, we have had 1,011,665 deaths and 82,034,738 SARS-CoV-2 infections in the United States. We have had 433,848 new infections in the last 14 days. We were adding an average of 266,924 infections every seven days. For the pandemic in the United States we are averaging one death for every 81.0 infections reported for each death or over 12,332 deaths for each one million infections. As of 4/8/22, thirty-six states have had greater than 500,000 total infections, and 36 states have had greater than 5,000 total deaths. Sixteen states (Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states (Florida, Texas, New York, and California) have had greater than 68,000 deaths. California and Texas have each had greater than 85,000 deaths.
On 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. On 11/20/21 in North Dakota, 9.18% of the population was infected (ranked #1), and in South Dakota, 8.03% of the population was infected (ranked #2). As of 4/8/22, in the United States, 24.52% of the population has had a documented SARS-CoV-2 infection. In the last 16 months, 21.83% of our country became infected with SARS-CoV-2. On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. In the last 16 months, there were 751,534 new deaths from SARS-CoV-2. For thirteen of those months, vaccines have been available to all adults. During these thirteen months, 440,568 people have died of SARS-CoV-2 infections. Most of the hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
As of 4/8/22, California was ranked 38th in infection percentage at 23.10%. In California 19.42% of Californians were infected in the last 16 months. As of 3/11/22 forty-three states have had greater than 20% of their population infected. Rhode Island was at 34.30% (ranked #1), Alaska was at 32.89% (ranked #2), North Dakota was at 31.50% (ranked #3), Tennessee was at 29.61% (ranked #4), Kentucky was at 29.52% (ranked #5), Utah was at 28.96% (ranked #6), South Carolina was at 28.54% (ranked #7), West Virginia was at 27.81% (ranked #8), Arizona was at 27.67% (ranked #9), Arkansas was at 27.61% (ranked #10) and Florida was at 27.51% (ranked #11) of their population infected. Forty-three states now have greater than 20% of their population infected.
The table below shows that if we rank the US states with the highest death rates per million population within the world rankings, we see that Mississippi, Arizona and Alabama had the eighth highest death rate, New Jersey and Arkansas have the ninth highest COVID-19 deaths per million in the world. Louisiana had the tenth, New York was at eleventh, Florida was at 12th and Rhode Island was at thirteenth. The United States as a whole ranks 18th in the world for deaths per million population (3,056 deaths per million). California ranks 39th in the USA (and 37th in the world). If we look at the death rates per million in South Korea (365), Iceland (296), Japan (227), and Israel (1,132), they suggest that treatment outcomes are somehow different in these four countries. The same phenomenon can be seen in Scandinavia, where the death rate in Sweden is 1,809 per million, compared to 485 per million in Norway and 600 per million in Finland. The United States should have taken a closer look at how countries with low death rates (like South Korea, Iceland, Japan, Finland, and Norway) were preventing COVID-19 infections and treating COVID-19 patients.
| State or Country | COVID-19 Deaths per million population | Rank in USA | Ranked within World |
| Mississippi | 4,171 | 1st | 8th tied |
| New Jersey | 3,748 | 6th | 9th tied |
| Louisiana | 3,695 | 8th | 10th |
| New York | 3,524 | 11th | 11th tied |
| Alabama | 3,952 | 3rd | 8th tied |
| Arizona | 4,078 | 2nd | 8th tied |
| Rhode Island | 3,327 | 19th | 13th |
| Arkansas | 3,745 | 7th | 9th tied |
| Florida | 3,424 | 17th | 12th |
| California | 2,264 | 39th | 37th |
| USA | 3,056 | 18th | |
| Peru | 6,288 | 1st | |
| Bosnia-Herzegovina | 4,848 | 3rd | |
| Hungary | 4,754 | 4th | |
| Montenegro | 4,308 | 6th | |
| Bulgaria | 5,351 | 2nd | |
| Czechia | 3,708 | 9th | |
| Brazil | 3,072 | 15th | |
| Georgia | 4,217 | 7th | |
| Sweden | 1,809 | 57th | |
| Israel | 1,132 | 85th | |
| Canada | 991 | 92nd | |
| Finland | 600 | 120th | |
| Norway | 485 | 127th | |
| Japan | 227 | 151st | |
| Iceland | 296 | 145th | |
| South Korea | 365 | 138th |
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Merck has developed the oral drug Molnupiravir, which induces RNA mutagenesis by viral RNA-dependent RNA polymerase of SARS-CoV-2 and other viruses. According to Kabinger et al, “Viral RNA-dependent RNA polymerase uses the active form of Molnupiravir, β-D-N4-hydroxycytidine triphosphate, as a substrate instead of cytidine triphosphate or uridine triphosphate. When the RNA-dependent RNA polymerase uses the resulting RNA as a template, β-D-N4-hydroxycytidine triphosphate directs incorporation of either guanine or adenine, leading to mutated (viral) RNA products. Analysis of RNA-dependent RNA polymerase–RNA complexes that contain mutagenesis products has demonstrated that β-D-N4-hydroxycytidine (the active form of Molnupiravir) can form stable base pairs with either guanine or adenine in RNA-dependent RNA polymerase explaining how the polymerase escapes proofreading and synthesizes mutated RNA” (quotation modified for clarity). The results of the phase 3 trial of Molnupiravir were published in the NEJM article “Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients” by Angélica Jayk Bernal, M.D. et al. (December 16, 2021 DOI: 10.1056/NEJMoa2116044). In this phase 3 study in the Molnupiravir group, 28 patients were hospitalized and one death occurred. In the placebo group, 53 patients were hospitalized and 9 died. Overall, 47% of hospitalizations and deaths were prevented by Molnupiravir. If you do a post hoc analysis and just look at deaths, Molnupiravir would prevent 89% of deaths. An Emergency Use Authorization by the FDA for Molnupiravir was approved on 12/24/21.The dose of Molnupiravir approved is four 200 mg capsules orally twice a day for five days. Diarrhea is reportedly a side effect in two percent of patients. I treated my first patient with Molnupiravir on 1/28/22. Currently more Molnupiravir is available weekly in the United States than PAXLOVID™ (see chart below; data from PHE.gov). Locally Molnupiravir is still available at CVS in Monterey (Fremont Blvd.; phone number: 831-375-5135) and CVS in Salinas (East Alisal Street; phone number 831-424-0026).




FDA-Approved Intravenous Monoclonal Antibody Treatment for Non-Hospitalized SARS-CoV-2 Patients
Sotrovimab is a human monoclonal antibody made by Vir Technology and Glaxo-SmithKline which received a FDA EUA approval on May 26,1921 for intravenous drug treatment for non-hospitalized SARS-CoV-2 infected patients. According to the FDA, “The data supporting this EUA for sotrovimab are based on an interim analysis from a phase 1/2/3 randomized, double-blind, placebo-controlled clinical trial in 583 non-hospitalized adults with mild-to-moderate COVID-19 symptoms and a positive SARS-CoV-2 test result. Of these patients, 291 received sotrovimab and 292 received a placebo within five days of onset of COVID-19 symptoms. The primary endpoint was progression of COVID-19 (defined as hospitalization for greater than 24 hours for acute management of any illness or death from any cause) through day 29. Hospitalization or death occurred in 21 (7%) patients who received placebo compared to 3 (1%) patients treated with sotrovimab, an 85% reduction.” Sotrovimab is given intravenously in a single 500 mg dose. Supplies of this drug are also very limited and currently are only available at hospitals. In order to get this drug, we will probably have to go through the same process outlined below for Evusheld. Sotrovimab is not effective against the BA.2 Omicron variant of SARS-CoV-2. On 3/25/22, the FDA revoked emergency use authorization for sotrovimab to treat COVID-19 infections in 8 states, Puerto Rico, and the Virgin Islands. They justified this decision with the reasoning that, according to the CDC, BA.2 accounts for more than 50% of cases in HH2 regions 1 and 2. We decided to look at data from Walgreens’ COVID-19 Index, which is updated every few days.
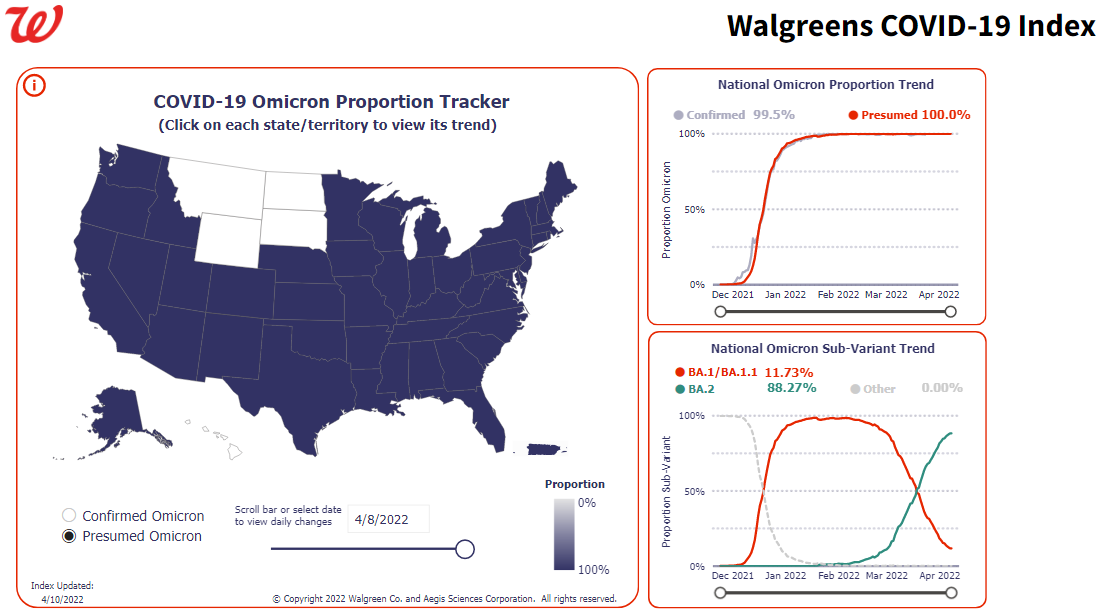
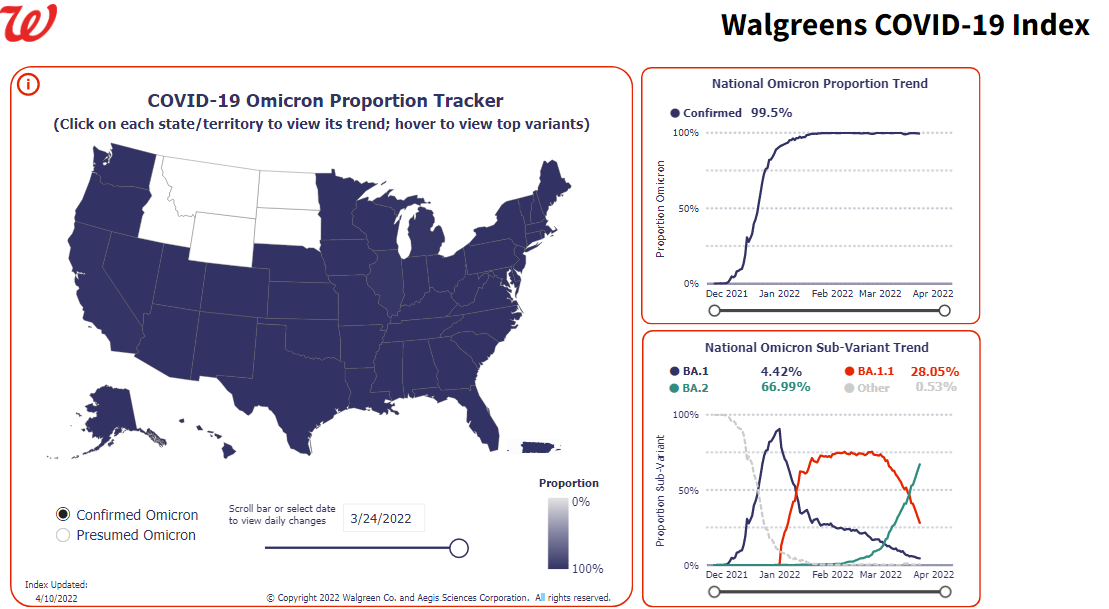
Omicron Subvariant Trends by State (from Walgreens COVID-19 Index) for 3/24/22 and 4/08/22


Bebtelovimab is a new monoclonal antibody treatment for mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death, and for whom alternative COVID-19 treatment options approved or authorized by FDA are not accessible or clinically appropriate. The authorized dose of bebtelovimab is 175 mg, given as an intravenous injection over at least 30 seconds. The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for this drug on 2/11/22. Bebtelovimab is a human antibody that demonstrates neutralization against the Omicron variants and is available in every state and many hospitals and some clinics. If you are planning on using a monoclonal antibody to treat a SARS-CoV-2 infection currently we think that bebtelovimab rather than sotrovimab should be used for SARS-CoV-2 in all states based on the above Walgreen data sets from 3/24/22 and 4/08/22.
FDA Approved Intramuscular Prophylaxis of SARS-CoV-2 Immunocompromised Patients
Evusheld (from AstraZeneca) contains two human monoclonal antibodies, Tixagevimab (150 mg in 1.5 mL) and Cilgavimab (150 mg in 1.5 mL), in separate vials. According to the manufacturer, “Tixagevimab and Cilgavimab are two recombinant human IgG1κ monoclonal antibodies with amino acid substitutions to extend antibody half-life (YTE), reduce antibody effector function, and minimize the potential risk of antibody-dependent enhancement of disease (TM). Tixagevimab and Cilgavimab can simultaneously bind to non-overlapping regions of the receptor binding domain (RBD) of SARS-CoV-2 spike protein. Tixagevimab, Cilgavimab, and their combination bind to spike protein with equilibrium dissociation constants of KD = 2.76 pM, 13.0 pM and 13.7 pM, respectively, blocking its interaction with human ACE2, the SARS-CoV-2 receptor, which is required for virus attachment. Tixagevimab, Cilgavimab, and their combination blocked RBD binding to human ACE2 with IC50 values of 0.32 nM (48 ng/mL), 0.53 nM (80 ng/mL), and 0.43 nM (65 ng/mL), respectively.” Each monoclonal antibody is administered intramuscularly to immunocompromised patients in two separate injections every six months. Evusheld availability in California is limited and has been rationed/distributed by our local Public Health Department only to hospitals. Physicians in Monterey County who want to receive a distribution (or redistribution) of Evusheld need to be added to the list of eligible facilities by the State Therapeutics group. The first step is for the Monterey County EMS Agency (phone: 831-755-5713) to make a request to the State Therapeutics group to have the facility added to the system for further verification. Due to extremely limited availability, evidently the State Therapeutics group is currently only considering additions on a case by case basis. Physicians who wish to submit their facility for consideration will need to provide the following information to the Monterey County EMS Agency:
- Facility/Provider Name for Registration
- Provider Type (Hospital, Pharmacy, Etc)
- Shipping Address
- Contact Name(s)
- Contact Email(s)
- Contact Phone Number(s)
As for my immunocompromised patients: We provided this information by email to the Monterey County EMS Agency on 1/26/22 and will update you when or if we become an eligible provider and receive our first doses of Evusheld.
On 2/24/22, the FDA revised its dosing guidance for Evusheld, doubling the dosage of its two components, Tixagevimab and Cilgavimab, from 150 mg each to 300 mg each. They explain, “Based on the most recent information and data available, Evusheld may be less active against certain Omicron subvariants. The dosing regimen was revised because available data indicate that a higher dose of Evusheld may be more likely to prevent infection by the COVID-19 Omicron subvariants BA.1 and BA.1.1 than the originally authorized Evusheld dose.” Patients who have already received their first administration of Evusheld intramuscularly will need to contact their healthcare provider to get a second 150 mg injection of Tixagevimab and Cilgavimab. If you have not received Evusheld yet, the correct dose is 3 mL/300 mg of each monoclonal antibody injected intramuscularly. This large volume necessitates administration of the antibodies in the gluteus, with two separate injections.
The Threat of SARS-CoV-2 Variants
In response to the need for “easy-to-pronounce and non-stigmatising labels,” at the end of May, the World Health Organization assigned a letter from the Greek alphabet to each SARS-CoV-2 variant. GISAID, Nextstrain, and Pango will continue to use the previously established nomenclature. For our purposes, we’ll be referring to each variant by both its Greek alphabet letter and the Pango nomenclature.
The WHO has sorted variants into two categories: Variants of Concern (VOC) and Variants of Interest (VOI). The criteria for Variants of Concern are as follows:
- Increase in transmissibility or detrimental change in COVID-19 epidemiology; or
- Increase in virulence or change in clinical disease presentation; or
- Decrease in effectiveness of public health and social measures or available diagnostics, vaccines, therapeutics.
The WHO categorizes the following five variants as Variants of Concern (VOC):
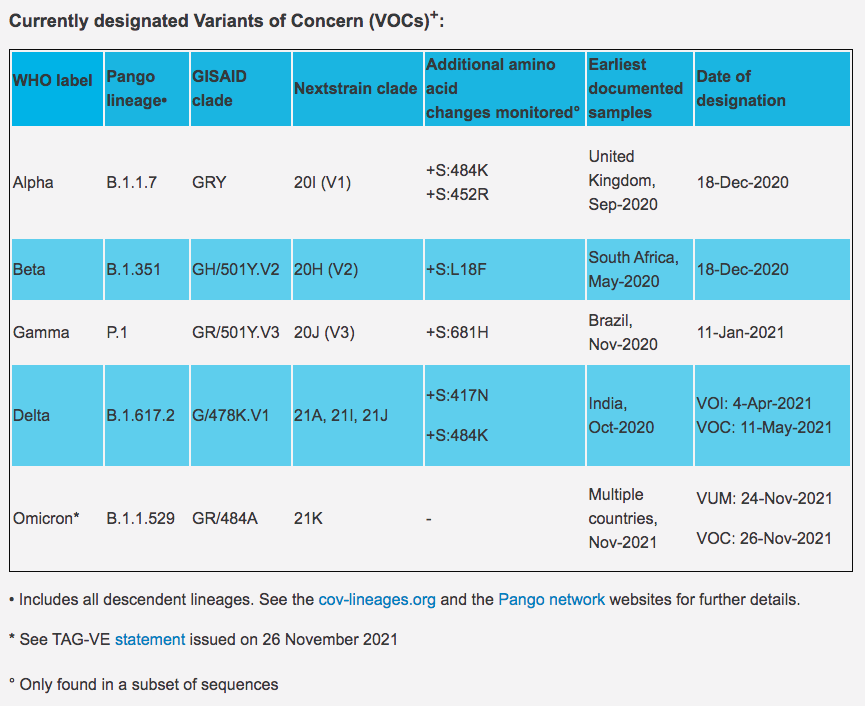
Source: World Health Organization
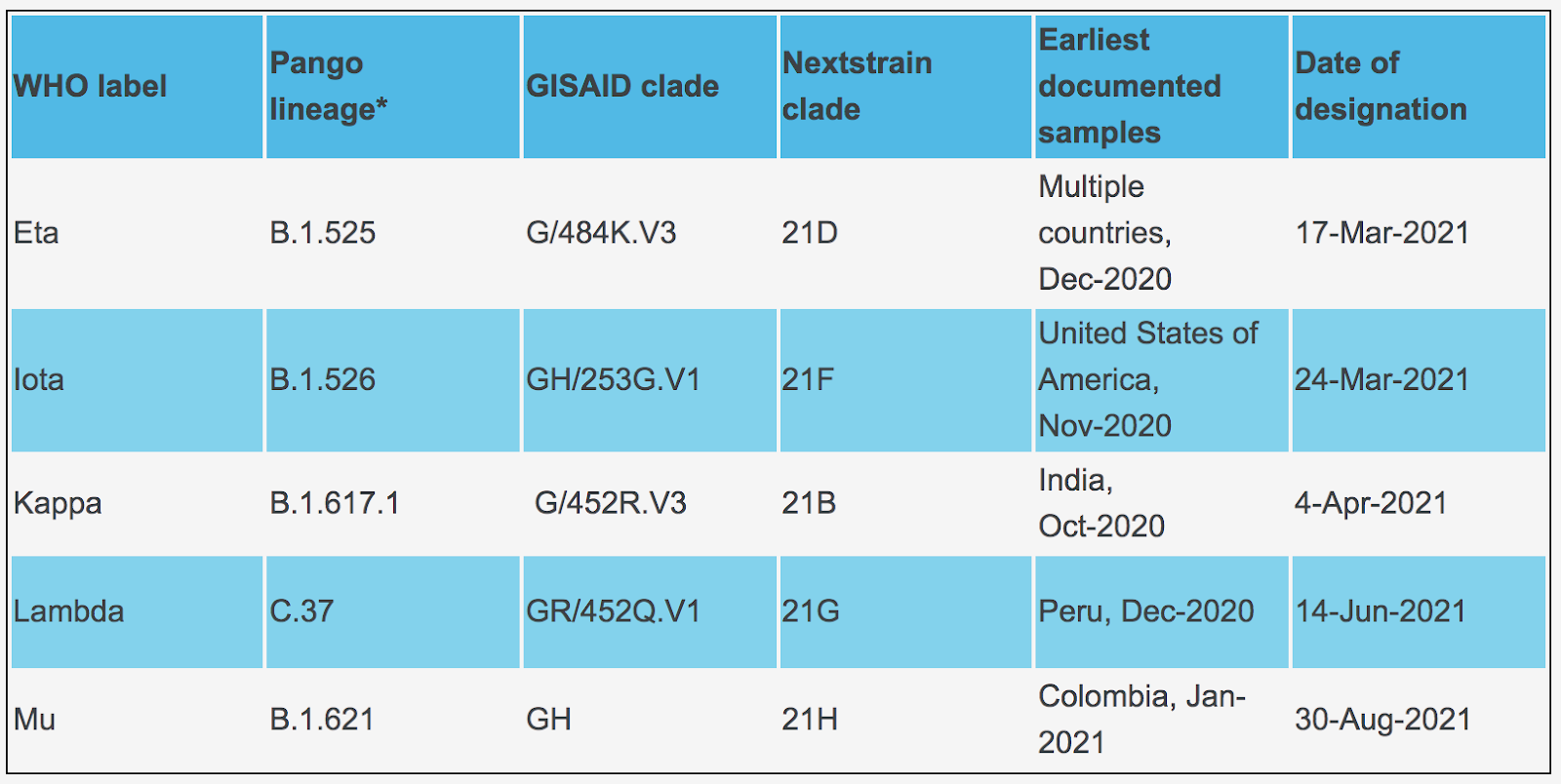
The criteria for Variants of Interest (VOI) are as follows:
- has been identified to cause community transmission/multiple COVID-19 cases/clusters, or has been detected in multiple countries; OR
- is otherwise assessed to be a VOI by WHO in consultation with the WHO SARS-CoV-2 Virus Evolution Working Group.
The WHO categorizes the following six variants as Variants of Interest (VOI):
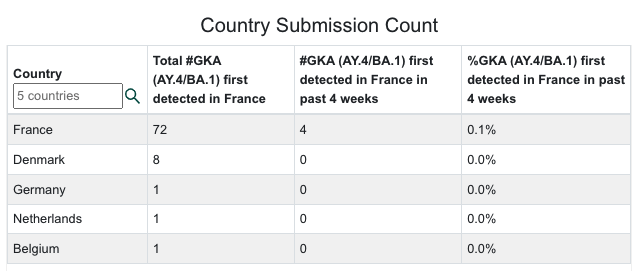
According to the UK Health Security Agency Technical Briefing from 2/25/22, “A putative Delta and Omicron recombinant has been identified in the UK, with likely parental lineages AY.4.2.2 and BA.1.1 and a breakpoint in non-structural protein 3 (nsp3). The presence of 34 genomes sampled between 7 January 2022 and 14 February 2022 suggest that this recombinant is able to transmit.” GISAID has also begun publishing data about a recombinant of Delta AY.4 and Omicron BA.1, first identified in France. According to GISAID data, this variant has also been detected in Denmark, Germany, the Netherlands, and the United States. Forbes
We will need to monitor for this Delta-Omicron recombinant variant in the United States as well.
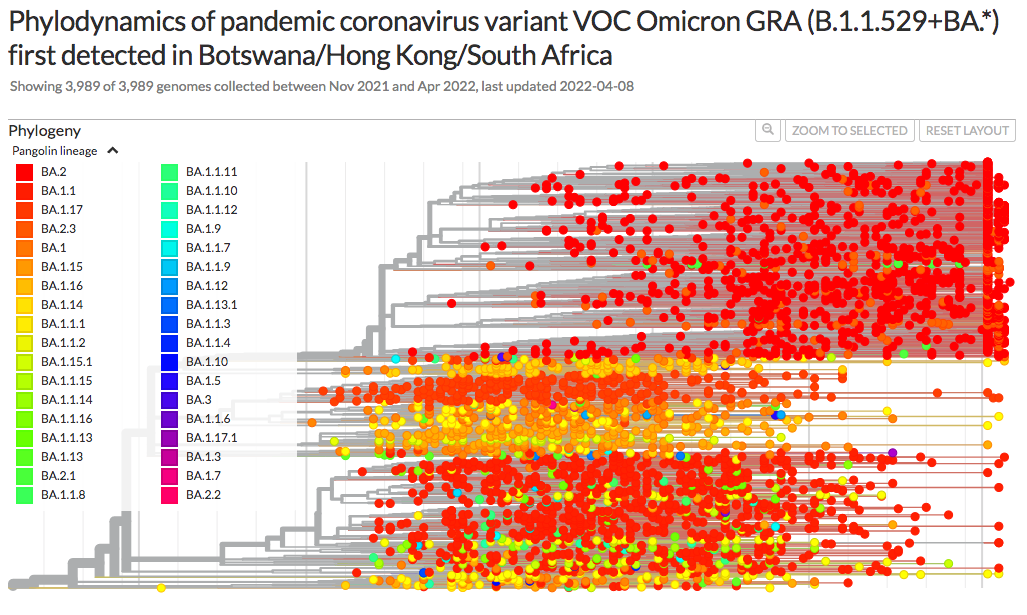
Omicron cases sequenced as of 4/10/22:
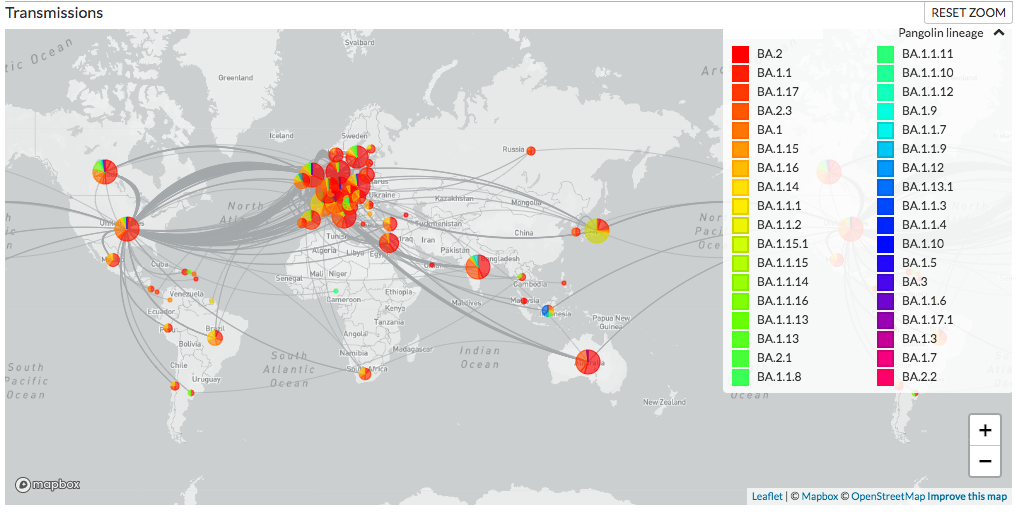
Map of Omicron sequenced transmissions:
Delta cases sequenced as of 4/10/22:
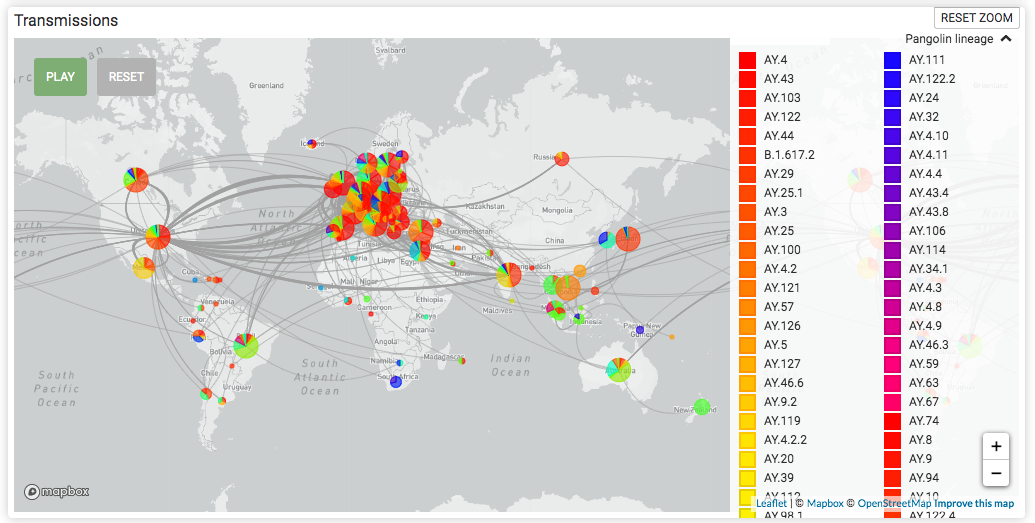
Map of Delta sequenced transmissions:
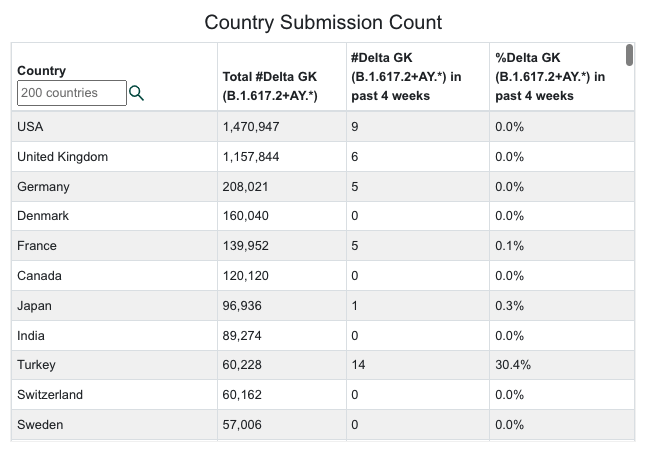
GKA (AY.4/BA.1) cases sequenced as of 4/10/22:
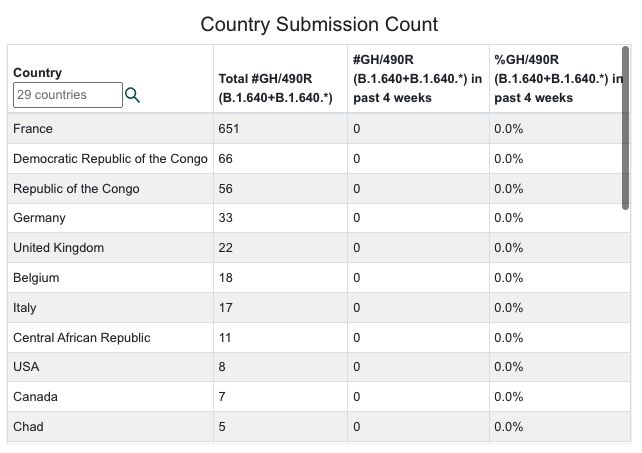
B.1.640 cases sequenced as of 4/10/22:
Watching World Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
| Location | Total Infections as of 4/8/22 | New Infections on 4/8/22 | Total Deaths | New Deaths on 4/8/22 | % of Pop.Infected | SARS-CoV-2 Isolates Currently Known in Location | National/ State Mask Mandate | Currently in Lockdown |
| World | 497,520,253(17,964,695 new infections in 14 days). | 1,087,730 | 6,198,662(56,243 new deaths in last 14 days) | 3,634 | 6.38% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22) | No | No |
| USA | 82,034,738(ranked #1) 433,848 new infections in the last 14 days. | 35,285(ranked #8) | 1,011,665(ranked #1)8,467 new deaths in the last 14 days. | 404 | 24.52% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21) | No | No |
| Brazil | 30,123,963(ranked #3) 497,143 new infections in the last 14 days. | 34,576 (ranked #11) | 658,626(ranked #2) | 259 | 13.85% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| India | 43,018,032(ranked #2); 321,706 new infections in 2 weeks. | 1,150 | 521,686(ranked #3) | 82 | 3.06% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| United Kingdom | 21,549,830(ranked #6; was #6 thirty weeks ago; 858,707 new infections in 2 weeks. | 25,305(ranked 11th in the world). | 169,759 (ranked #7 in world) | 347 | 31.45%(1.25% increase in the last 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinant | No | No |
| California, USA | 9,130,644(ranked #13 in the world; 44,240 new infections in the last 14 days). | 3,789 | 89,461 (ranked #20 in world) | 54 | 23.10%(0.14% increase in 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Mexico | 5,643,963(ranked #20) 71,541 new infections in 14 days). | 32,216 (ranked #9) | 323,508(ranked #5) | 105 | 4.79% | B2 lineageAlpha/B.1.1.7 (UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| South Africa | 3,730,066(ranked #29; 19,300 new infections in 14 days). | 1,377 | 100,084 (ranked #18) | 9 | 6.15% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Canada | 3,560,840(ranked #32, was 26th fourteen weeks ago; 285,094 new infections in 14 days). | 8,557 | 37,977(ranked #26) | 42 | 9.29% . | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Poland | 5,976,364(ranked #19; 43,262 new infections in 14 days). | 1,330 | 115,594 (ranked #15) | 58 | 15.82% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3 | No | No |
| Turkey | 14,946,379(ranked #10, 170,745 new infections in 14 days). | 7,120 | 98,342 (ranked #19) | 31 | 17.39% (0.20% of the country was infected in the last 14 days.) | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| Russia | 17,969,431(ranked #7), 254,031 new infections in 14 days). | 14,311 | 371,169(ranked #4 in world) | 280 | 12.30%; 0.17% of the country was infected in the last 14 days. | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)R1 (Japan) B.1.640.1 (Congo/France)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Argentina | 9,051,243(ranked #13; 27,431 new infections in 14 days). | 1,993 | 128,194 (ranked #14 in world) | 36 | 19.70% (0.05 % increase in two weeks). | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gama/P.1 (Brazil)Delta/B.1.617.2 (India)Lambda/C.37 (Peru)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Colombia | 6,087,443(ranked #17, 4,500 new infections in 14 days). | 320 | 139,703 (ranked #12 in the world) | 10 | 11.79% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Epsilon/B.1.427 + B.1.429 (USA)*Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Peru | 3,550,791(ranked #33, 6,453 new infections in 14 days). | 551 | 212,438(ranked #6) | 18 | 10.51%, a 0.02% increase in 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Indonesia | 6,030,168(ranked #18; 38,481 new infections in 14 days) | 1,755 | 155,556 (ranked #9) | 47 | 2.77% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Eta/B.1.525 (Nigeria/UK)Theta/P.3 (Philippines) Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)B.1.640.1 (Congo/France)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Iran | 7,186,992 39,585 new infections in last 14 days(ranked 15th; was 12th thirty weeks ago) | 3,184 | 140,528 (ranked #11) | 36 | 8.36% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Spain | 11,627,487(ranked 11th; 175,811 new infections in 14 days). | 16,278 | 103,104 (ranked #17) | 119 | 24.85%, a 0.38% increase in 14 days. | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| France | 26,698,031 (ranked #4; 1,918,149 new infections in the last 14 days). | 148,768 (ranked #3) | 143,141 (ranked #10) | 139 | 40.74%, a 2.93% increase in the last 14 days, a new pandemic record for 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant | No | No |
| Germany | 22,534,061(ranked #5; 2,515,596 new infections in 14 days.). | 169,454 (ranked #2) | 132,141 (ranked #13) | 336 | 26.74%, a 2.98% increase in the last 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Hungary | 1,868,007 (ranked #43; 27,649 new infections in 14 days). | 2,400 | 45,721 (ranked #23) | 37 | 19.42% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Romania | 2,870,486(ranked #38; 34,737 new infections in 14 days). | 1,709 | 65,179 (ranked#20) | 9 | 15.00% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| South Korea | 14,983,694 (ranked 9th) ; 3,821,462 new infections in 14 days). | 205,289(ranked#1) | 18,754 (ranked #44); 4,460 new deaths in 14 days, a new pandemic record for 14 days in South Korea). | 373 | 29.18%; a 7.45% increase in 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Ukraine | 4,982,249(ranked #21; 29,336 new infections in 14 days), | 2,025 | 108,818 (ranked #16) | 20 | 11.51% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Vietnam | 10,135,789(ranked #12; 1,319,338 new infections in 14 days). | 39,334(ranked #7) | 42,768 (ranked #24) | 35 | 10.25%, (a 1.34% increase in 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Netherlands | 7,971,855 (ranked #14; 271,140 new infections in 14 days). | 10,903 (ranked #10) | 22,080 (ranked #39) | 14 | 46.34%, (a 1.57% increase in 14 days). | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Denmark | 2,932,847, (ranked #37) 43,559 new infections in 14 days | 2,503 | 5,861 (ranked #84) | 24 | 50.32%, (a 0.74% increase in 14 days) | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
What Our Team Is Reading This Week
- China CDC shares latest COVID-19 data (GISAID) https://www.gisaid.org/resources/gisaid-in-the-news/china-shares-latest-11-apr-2022/#c920
- Persistent COVID-19 symptoms in a community study of 606,434 people in England (Nature) https://www.nature.com/articles/s41467-022-29521-z
- Brain Inflammation and Intracellular α-Synuclein Aggregates in Macaques after SARS-CoV-2 Infection (Viruses) https://www.mdpi.com/1999-4915/14/4/776
- Antibody Resistance of SARS-CoV-2 Omicron BA.1, BA.1.1, BA.2 and BA.3 Sub-lineages (Preprint) https://www.biorxiv.org/content/10.1101/2022.04.07.487489v1
- Infectious viral load in unvaccinated and vaccinated individuals infected with ancestral, Delta or Omicron SARS-CoV-2 (Nature Medicine) https://www.nature.com/articles/s41591-022-01816-0
- Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain (Preprint) https://www.biorxiv.org/content/10.1101/2022.01.07.475453v1
- Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: nationwide self-controlled cases series and matched cohort study (BMJ) https://www.bmj.com/content/377/bmj-2021-069590
- SARS-CoV-2 Infection Induces Ferroptosis of Sinoatrial Node Pacemaker Cells (Circulation Research) https://www.ahajournals.org/doi/10.1161/CIRCRESAHA.121.320518
- SARS-CoV-2 variants of concern and variants under investigation in England (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1063424/Tech-Briefing-39-25March2022_FINAL.pdf
- Neutralization of Omicron BA.1, BA.2, and BA.3 SARS-CoV-2 by 3 doses of BNT162b2 vaccine (Preprint) https://doi.org/10.1101/2022.03.24.485633
- COVID-19-Associated Encephalitis: Two Case Reports https://www.cureus.com/articles/86903-covid-19-associated-encephalitis-two-case-reports
- First evidence that an emerging mammalian alphacoronavirus is able to infect an avian species (Transboundary and Emerging Diseases) https://doi.org/10.1111/tbed.14535
- SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses (The Lancet) https://doi.org/10.1016/S0140-6736(22)00383-X
- Evidence for SARS-CoV-2 Delta and Omicron co-infections and recombination (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.09.22272113v1
- Culture and identification of a “Deltamicron” SARS-CoV-2 in a three cases cluster in southern France (Preprint) https://www.medrxiv.org/content/10.1101/2022.03.03.22271812v1.full
- Mandatory masking in schools reduced COVID-19 cases during Delta surge (NIH press release) https://www.nih.gov/news-events/news-releases/mandatory-masking-schools-reduced-covid-19-cases-during-delta-surge
- School Masking Policies and Secondary SARS-CoV-2 Transmission (Pediatrics) https://publications.aap.org/pediatrics/article/doi/10.1542/peds.2022-056687/185379/School-Masking-Policies-and-Secondary-SARS-CoV-2
- Transmission of SARS-CoV-2 delta variant (AY.127) from pet hamsters to humans, leading to onward human-to-human transmission: a case study (The Lancet) https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00326-9/fulltext
- COVID-19 Variant Dashboard – USA by Raj Rajnarayanan https://public.tableau.com/app/profile/raj.rajnarayanan/viz/USAVariantDB/VariantDashboard
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 38 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1060337/Technical-Briefing-38-11March2022.pdf
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 37 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1057359/Technical-Briefing-37-25February2022.pdf
- Engineered extracellular vesicles antagonize SARS-CoV-2 infection by inhibiting mTOR signaling (Biomaterials and Biosystems) https://www.sciencedirect.com/science/article/pii/S2666534422000046?via%3Dihub
- Severe Neuro-COVID is associated with peripheral immune signatures, autoimmunity and neurodegeneration: a prospective cross-sectional study (Preprint) https://doi.org/10.21203/rs.3.rs-1385593/v1
- Dynamics of the Delta and Omicron variants of SARS-CoV-2 in the United States: the battle of supremacy in the presence of vaccination, mask usage and antiviral treatment (Preprint) https://doi.org/10.21203/rs.3.rs-1420446/v1
- Virological characteristics of SARS-CoV-2 BA.2 variant (Preprint) https://www.biorxiv.org/content/10.1101/2022.02.14.480335v1
- Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: Evidence from Danish Households (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.28.22270044v1
- Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance — VISION Network, 10 States, August 2021–January 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7107e2.htm?s_cid=mm7107e2_e&ACSTrackingID=USCDC_921-DM75599&ACSTrackingLabel=MMWR%20Early%20Release%20-%20Vol.%2071%2C%20February%2011%2C%202022&deliveryName=USCDC_921-DM75599
- SARS-CoV-2 B.1.1.529 (Omicron) Variant Transmission Within Households — Four U.S. Jurisdictions, November 2021–February 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7109e1.htm?s_cid=mm7109e1_w
- Pediatric Emergency Department Visits Before and During the COVID-19 Pandemic — United States, January 2019–January 2022 (MMWR) https://www.cdc.gov/mmwr/volumes/71/wr/mm7108e1.htm?s_cid=mm7108e1_w#F2_down
- Birth Of The Omicron Family: BA.1, BA.2, BA.3. Each As Different As Alpha Is From Delta. (Forbes) https://www.forbes.com/sites/williamhaseltine/2022/01/26/birth-of-the-omicron-family-ba1-ba2-ba3-each-as-different-as-alpha-is-from-delta/?sh=403de4ee3da9
- Take a look at SARS-CoV-2’s family tree. It’s full of surprises (NPR) https://www.npr.org/sections/goatsandsoda/2022/02/09/1047616658/take-a-look-at-sars-cov-2s-family-tree-its-full-of-surprises
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 35 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1050999/Technical-Briefing-35-28January2022.pdf
- Memory B cell repertoire from triple vaccinees against diverse SARS-CoV-2 variants (Nature) https://www.nature.com/articles/s41586-022-04466-x_reference.pdf
- Dynamics of infection-elicited SARS-CoV-2 antibodies in children over time (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.14.22269235v1
- Syncytin, envelope protein of human endogenous retrovirus (HERV): no longer ‘fossil’ in human genome (Animal Cells and Systems) https://doi.org/10.1080/19768354.2021.2019109
- Host Chitinase 3-like-1 is a Universal Therapeutic Target for the Delta, Omicron and Other SARS-CoV-2 Viral Variants in COVID 19 (Preprint) https://www.biorxiv.org/content/10.1101/2022.01.21.477274v1
- COVID-19 reinfections among naturally infected and vaccinated individuals (Nature) https://www.nature.com/articles/s41598-022-05325-5
- Duration of Protection against Mild and Severe Disease by Covid-19 Vaccines (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMoa2115481
- Neutralizing immunity in vaccine breakthrough infections from the SARS-CoV-2 Omicron and Delta variants (Preprint) https://www.medrxiv.org/content/10.1101/2022.01.25.22269794v1
- COVID-19 and the Common Cold—Preexisting Coronavirus Antibodies May Hinder SARS-CoV-2 Immunity (JAMA) https://jamanetwork.com/journals/jama/fullarticle/2788621?guestAccessKey=0bbad800-e651-496b-8046-d124bbc63a5a&term=01262022&utm_source=silverchair&utm_medium=email&utm_campaign=article_alert-jama&utm_content=olf&utm_term=012622
- Viral dynamics and duration of PCR positivity of the SARS-CoV-2 Omicron variant https://dash.harvard.edu/handle/1/37370587
- Emergence in Southern France of a new SARS-CoV-2 variant of probably Cameroonian origin harbouring both substitutions N501Y and E484K in the spike protein (Preprint) https://doi.org/10.1101/2021.12.24.21268174
- A living WHO guideline on drugs for covid-19 (BMJ) https://doi.org/10.1136/bmj.m3379
- Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis (Science) https://doi.org/10.1126/science.abj8222
- Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection (Nature) https://www.nature.com/articles/s41590-021-01113-x
- An upper bound on one-to-one exposure to infectious human respiratory particles (PNAS) https://www.pnas.org/content/118/49/e2110117118
- Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies (Nature) https://doi.org/10.1038/d41586-021-03796-6
- Frequent Occurrence of SARS-CoV-2 Transmission among Non-close Contacts Exposed to COVID-19 Patients (Journal of Korean Medical Science) https://doi.org/10.3346/jkms.2021.36.e233
- Serial Screening for SARS-CoV-2 in Rectal Swabs of Symptomatic COVID-19 Patients (Journal of Korean Medical Science) https://doi.org/10.3346/jkms.2021.36.e301
- Saliva swabs are the preferred sample for Omicron detection (Preprint) https://doi.org/10.1101/2021.12.22.21268246
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing: Update on hospitalisation and vaccine effectiveness for Omicron VOC-21NOV-01 (B.1.1.529) 31 December 2021 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1044481/Technical-Briefing-31-Dec-2021-Omicron_severity_update.pdf
- Characteristics and Clinical Outcomes of Children and Adolescents Aged <18 Years Hospitalized with COVID-19 — Six Hospitals, United States, July–August 2021 (MMWR) https://www.cdc.gov/mmwr/volumes/70/wr/mm705152a3.htm
- The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry. (Preprint) https://drive.google.com/file/d/1vam2PVMWvfRBczqs_uZbnUixGja1QPZD/view
- Initial Assessment of SARS-CoV-2 Omicron Variant in Exhaled Breath Aerosol (Preprint) https://mfr.osf.io/render?url=https%3A%2F%2Fosf.io%2Fdscy3%2Fdownload
- Multisystem Involvement in Post-acute Sequelae of COVID-19 (PASC) (Annals of Neurology) https://doi.org/10.1002/ana.26286
- Taiwan rejects US CDC guidance on 5-day quarantine (Taiwan News) https://www.taiwannews.com.tw/en/news/4393548
- Risk assessment for SARS-CoV-2 variant: Omicron VOC-21NOV-01 (B.1.1.529) (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1041896/15-december-2021-risk-assessment-for-SARS_Omicron_VOC-21NOV-01_B.1.1.529.pdf
- HKUMed finds Omicron SARS-CoV-2 can infect faster and better than Delta in human bronchus but with less severe infection in lung https://www.med.hku.hk/en/news/press/20211215-omicron-sars-cov-2-infection
- mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant (Preprint) https://www.medrxiv.org/content/10.1101/2021.12.14.21267755v1/
- “Breakthrough” COVID-19 Hospitalizations Among Fully Vaccinated Patients Occur Most Often among Older Adults and Involve People with Chronic Health Conditions (KFF) https://www.kff.org/coronavirus-covid-19/press-release/breakthrough-covid-19-hospitalizations-among-fully-vaccinated-patients-occur-most-often-among-older-adults-and-involve-people-with-chronic-health-conditions/

You must be logged in to post a comment.