
The Omicron variant of SARS-CoV-2, the virus that causes COVID-19, was first identified in South Africa and was classified as a Variant of Concern by both WHO and CDC in November 2021. The first Omicron case to be sequenced in the US was identified in California on December 1 and the first reported death due to Omicron in the US was on December 20 in Texas. According to GISAID, in the last 30 days, the United States only sequenced about 2.56% of COVID cases (compare this to 9.8% in the UK, 6% in Australia, 18% in Denmark, and 17% in Israel), which would explain why we’re late to the game in addressing Omicron.
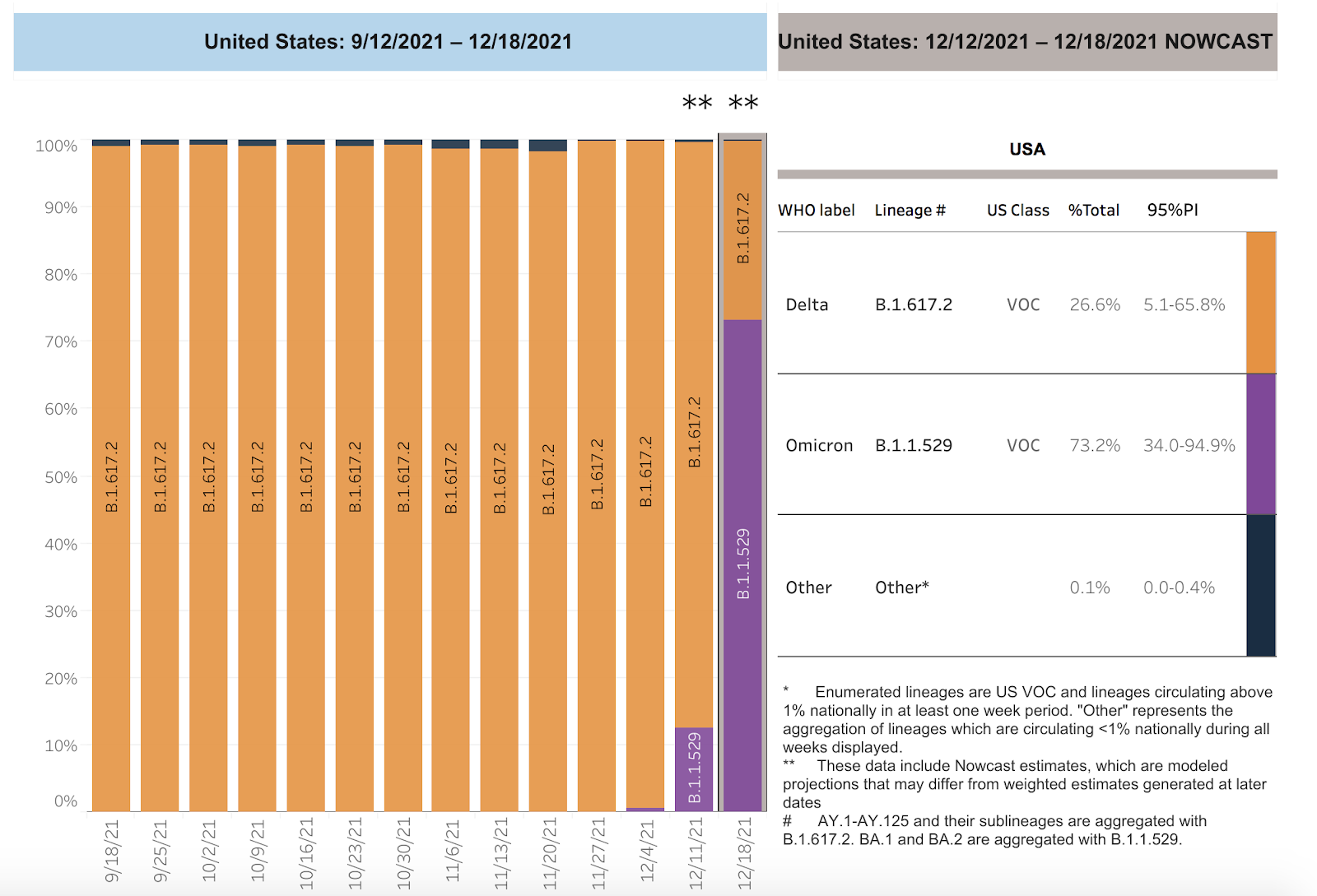
In under three weeks, Omicron has become the dominant variant in the US.
In the US, Omicron went from making up 12.6% of new COVID cases two weeks ago (week ending 12/11/32) to making up 73% of cases last week (reported 12/18/21). That’s an increase of more than 400% in one week. By comparison, the Delta doubled about once a week, going from around 3% of cases in mid-June to 41% of cases by early July and 62% of cases by mid-July. Omicron became the dominant variant in the US in less than half the amount of time that Delta did.
In Los Angeles County, new COVID infections per day (8,000+) are now over triple what they were a week ago.


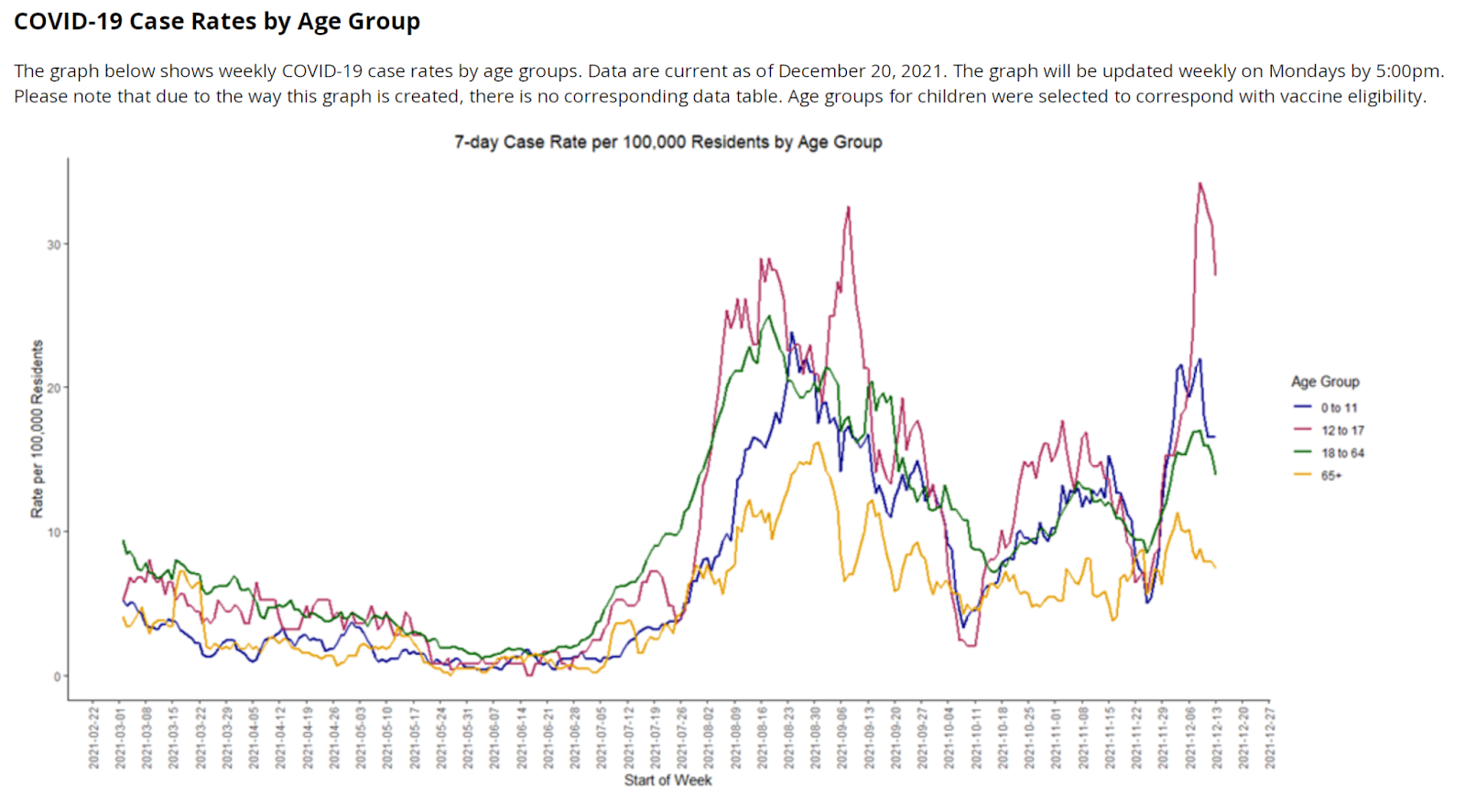
In December, Monterey County has seen a spike in cases for all age groups, but especially for children 12-17.
Statewide, this past weekend, California averaged 2,456 more new cases per day than the previous weekend.
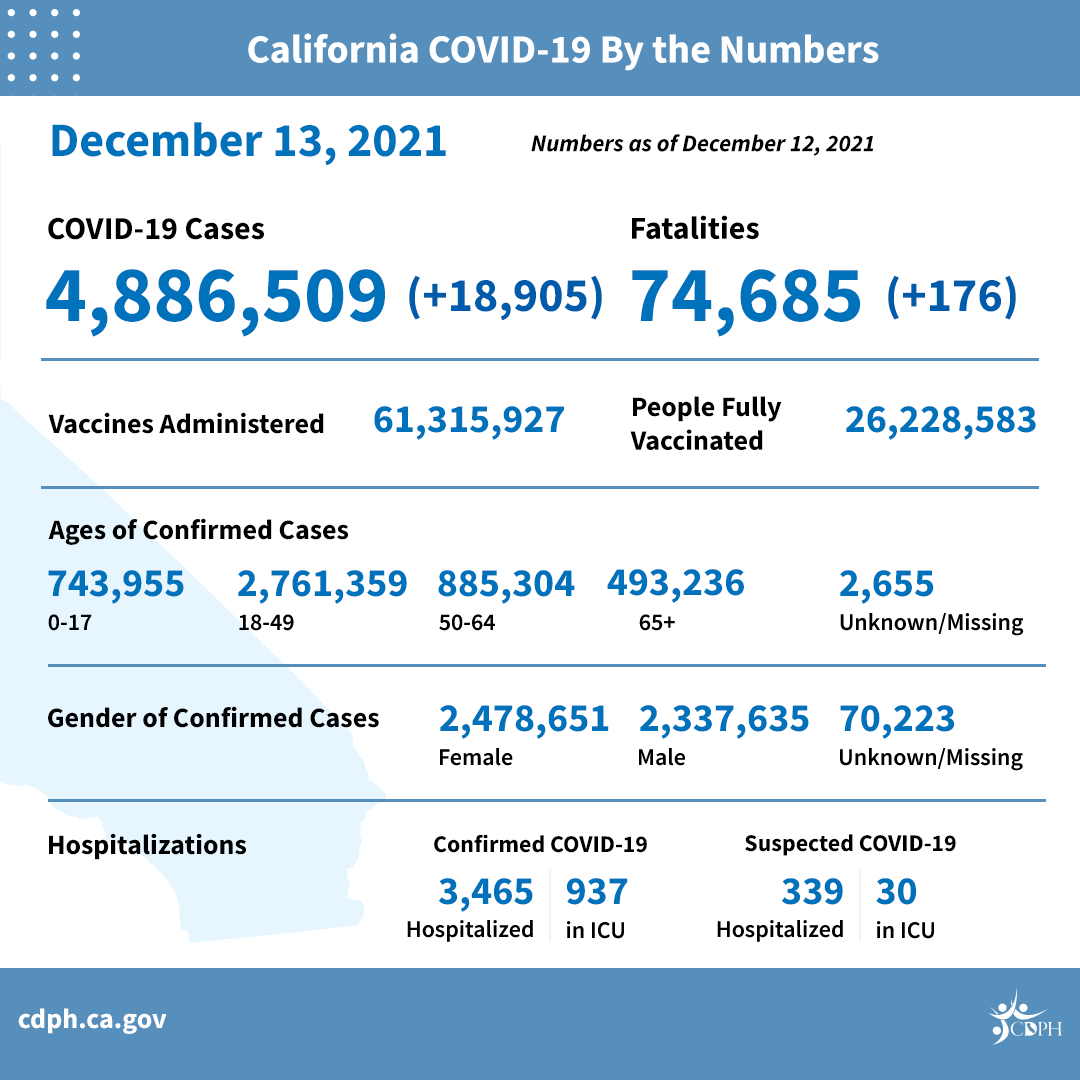
*Includes weekend cases—average 6,301 new cases per day. Source: https://www.cdph.ca.gov/Programs/OPA/Pages/NR21-360.aspx
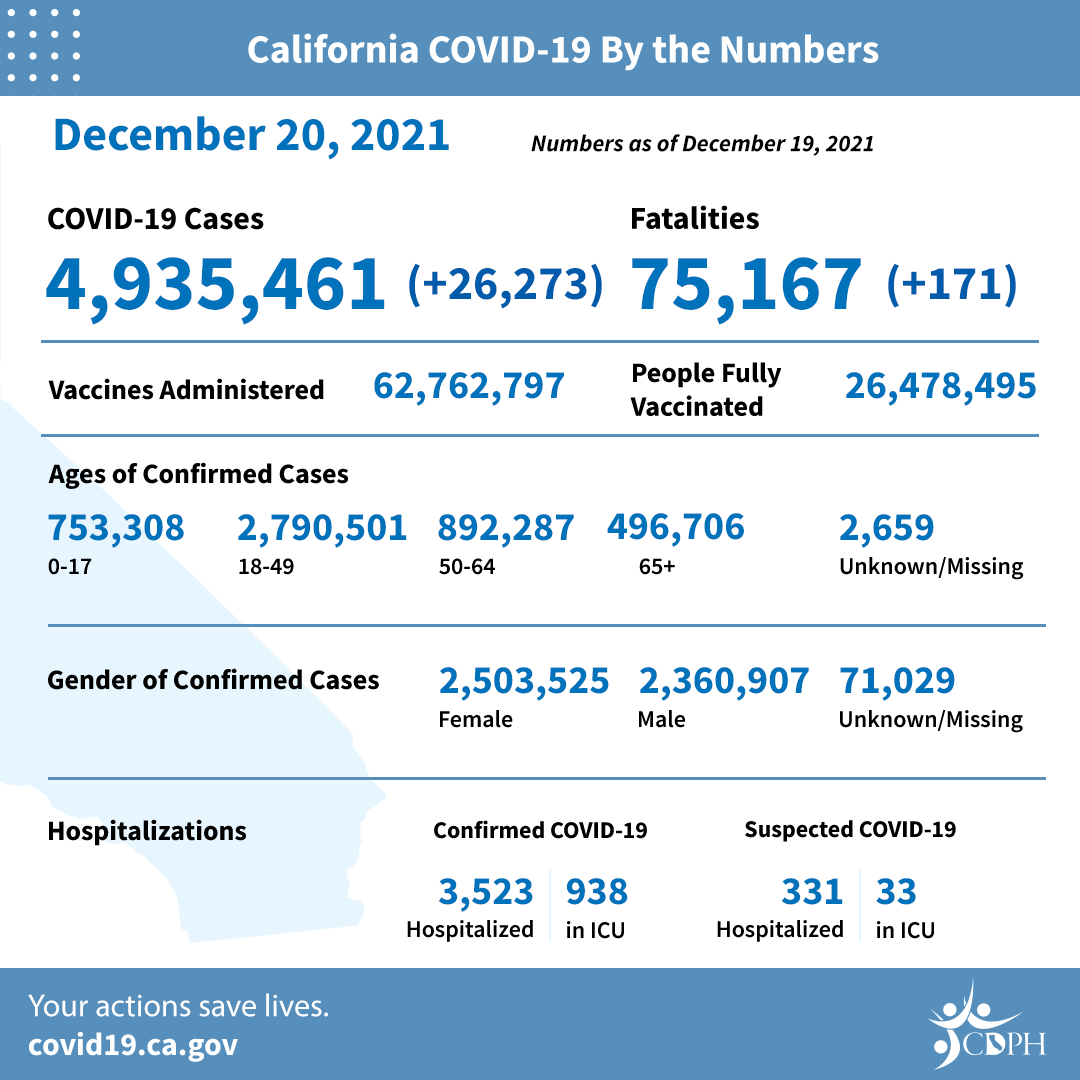
*Includes weekend cases—average 8,757 new cases per day, an increase of 2,456. Source: https://www.cdph.ca.gov/Programs/OPA/Pages/NR21-351.aspx
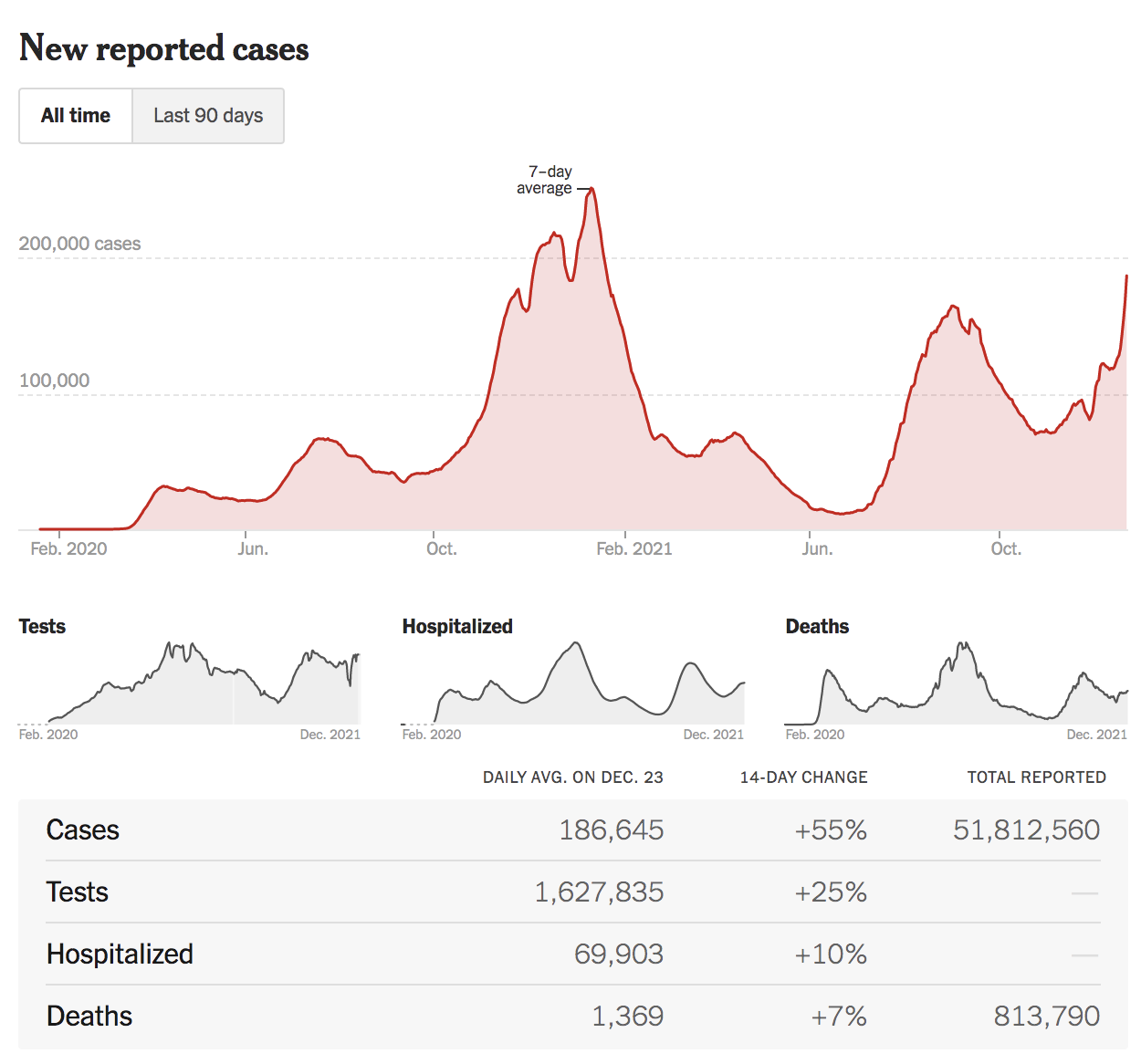
In the United States, as of 12/23/21, cases, deaths, and hospitalizations are trending upward.
Cases are up 55% over the last 14 days, deaths are up 7%, and hospitalizations are up 10%.
Nearly everyone (vaccinated or not, previously infected or not) who is exposed to Omicron is likely to become infected; vaccines will still prevent many infections, hospitalizations, and deaths, just not as many as with previous variants.
A study in South Africa found that during the current Omicron wave, two doses of the Pfizer vaccine provided “70% protection against severe complications of COVID-19 requiring hospitalisation, and 33% protection against COVID-19 infection.” In addition, researchers at Imperial College London estimate that the reinfection risk for Omicron is 5.4 times higher than for Delta, meaning that folks with previous COVID infections are likely to have limited protection.
Monoclonal antibody treatment (MAB) has saved the lives of many patients infected with other variants; it appears to be less effective against Omicron.
Two preprints, one published by German researchers on December 7, and another, a collaboration between American, Italian, Swiss, and Australian researchers, published on December 14, both suggest that due to Omicron’s 37 mutations in the Spike protein, 15 of which are in the receptor binding domain (RBD), it is able to evade our currently-available monoclonal antibody drugs. As William Haseltine explains in his write-up of the December 14 preprint: “Of the eight approved or authorized antibodies, all but sotrovimab completely or almost completely lost their neutralizing activity against the Omicron pseudovirus,” and “sotrovimab…retained neutralizing activity, but at a significant reduction.”
Omicron spreads more easily in households than Delta does, making it more likely that people will infect their loved ones this winter.
Data collected in UK households suggests that the secondary attack rate (chance that an index case in a household will infect someone else) for Omicron is 21.6%, compared to 10.8% for Delta.
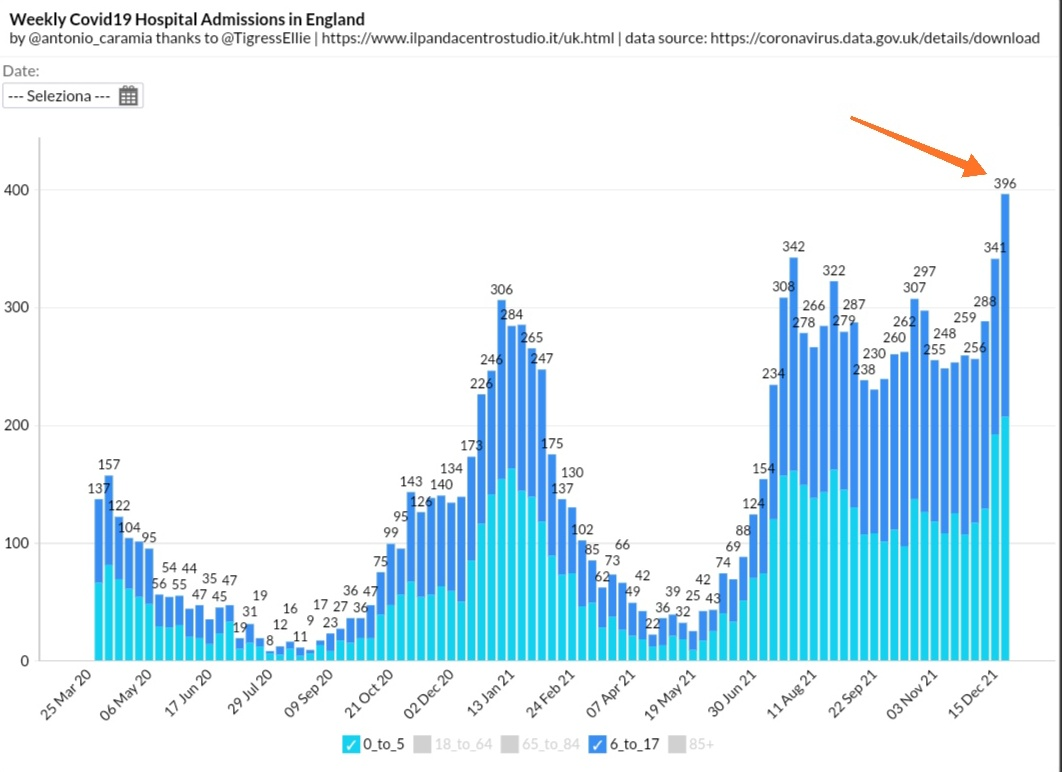
Children may be at higher risk of contracting Omicron and being hospitalized, compared to previous variants.
A South African study found that “Despite very low absolute incidence, preliminary data suggests that children have a 20% higher risk of hospital admission in Omicron-led fourth wave in South Africa, relative to the D614G-led first wave.” And in England, hospital admissions for children over the last week are at an all-time high of 396.
This morning, the Washington Post reported that pediatric hospitals around the country are filling up; over the past three days, approximately 800 children per day were admitted for COVID infections.
Even mild infections can have severe consequences, like Long COVID and MIS-C. Those infected with Omicron who develop mild infections may still face long-term health complications due to Long COVID and/or MIS-C, and many of these patients in the US will go without proper diagnosis and treatment. Ed Yong has documented for The Atlantic how even health care workers have been dismissed and denied treatment for Long COVID. And yes, children also get Long COVID.
Now that you know more about Omicron, what should you do?
- Wear a highly-protective mask, like an N95 or KN95. Beware of fakes. Do not order from a website like Amazon, which does not vet its suppliers. Project N95 is a trustworthy supplier of masks. For more on how to buy a quality mask online, see this NY Times piece and also this one. If you are not able to purchase an N95 or KN95 mask, layer a cloth mask over a surgical mask for a tight fit. Always make sure your mask covers your nose, mouth, and chin, with no gaps at the top or around the sides.
- Get your booster vaccine as soon as possible. Per CDC, everyone 16+ should receive a booster shot. If you are not yet fully vaccinated, get vaccinated, and encourage friends and family to do the same. Everyone age 5+ can be vaccinated. LA County residents can go here to find information on where to get vaccinated. US residents can text your ZIP code to 438829 or call 1-800-232-0233 to find vaccine locations near you.
- Gather outdoors and keep distance between you and people from outside your household. Because COVID is airborne, when people gather indoors, the virus builds up in the air, making it more likely for people to get infected. Think about it like cigarette smoke. If you allowed someone to smoke inside your house, the smoke would stay in the air, even hours later, making your indoor air unsafe to breathe. If you had a backyard barbecue and the same person went to the far corner of your yard (away from other people) to smoke, the chances of you breathing that smoke would be significantly lower.
- If you must gather indoors, make sure everyone masks and that the space is well-ventilated. Open windows and use HEPA air purifiers whenever possible. Don’t have an air purifier? You can make a simple but effective one using HVAC filters and a box fan.
- Test before and after you gather. If hosting a gathering, you can ask your guests to take a rapid antigen test at home on the day of the event. These tests, like Abbott’s Binax and Quidel’s Quickvue, don’t catch 100% of infections, but they will catch many. There are some tests (made by Applied DNA Sciences, Meridian Bioscience and Tide Laboratories) that the FDA has said cannot identify the Omicron variant, so take care to avoid those.
- Avoid gathering with unvaccinated people. Make it clear to friends and family that gathering with you is a privilege, not a right. Vaccine-hesitant loved ones may find the motivation they need to get vaccinated if they realize that’s the only way that they’ll be seeing you.
- Get your flu shot. COVID isn’t the only thing putting people in the hospital this winter, and it’s possible to be infected with both flu and COVID. A flu shot is the best defense against the flu.
- If you develop COVID symptoms or flu-like symptoms: get tested for COVID-19. If you test negative for COVID, you may have the flu. If you believe you have the flu and have tested negative for COVID, you should request a prescription from your doctor for Tamiflu within the first 72 hours.

