
In this post:
- The United States still leads the world in COVID-19 cases and deaths.
- We have no effective available oral treatment or preventative drugs, vaccines or hyperimmune intravenous immunoglobulin for COVID-19. Potential therapies are probably 6 to 9 months away.
- Despite the data, in the United States our political leaders , federal agencies, and many state public health officials have decided to open back up our country.
- In California, although ICU numbers have been stable the last 7 days, COVID-19 cases and deaths are still on the rise. The majority of reported cases (50.8%) are in the 18-49 age group.
- We examine the 1918 flu pandemic’s impact on different age groups and compare it with this year’s COVID-19 data in California, concluding that closing schools early was wise and reopening in August would be deadly.
- We continue to recommend staying home whenever possible, wearing a mask in public, and staying 6 feet apart from people outside your household. We outline suggestions for businesses and organizations seeking to reopen more safely, highlighting the dangers of congregating in buildings with poor ventilation (which is most buildings).
- In Monterey County, agricultural workers, health care workers, and first responders are among the occupations most impacted by COVID-19. More than half of COVID-19 patients in the county have no known pre-existing medical condition.
- The incomplete nature of the data collected from California’s skilled nursing homes is problematic.
- Based on our modeling, we expect to have 2 million COVID-19 infections and 115,357 deaths in the United States by June 7.
- By August 4, 2020, at our current rate of new COVID-19 infections and deaths, we anticipate 3,337,190 COVID-19 infected patients and a total of 192,613 deaths.
By our way of counting, this is Day 145 of the COVID-19 pandemic. To date, we have neither a vaccine nor a widely-available drug to effectively treat or prevent this infection. Our first USA case was identified in Washington State on Day 21 of the pandemic. In those next 124 days (17.7 weeks) the United States, as of 5/22/20, had 1,645,099 known COVID-19 PCR positive infected patients and 97,647 deaths, giving us a still rising death rate of 5.94%. We had 24,197 new cases and 17,109 people in serious or critical condition on that day. That was the fourth day in a row that we’ve had over 17,000 people in serious or critical condition in the United States. We have 1,314,204 more COVID-19 positive infected patients than any other country in the world. The five countries other than the US with the most cases (Brazil, Russia, Spain, the United Kingdom, and Italy) have a total of 1,422,095 cases combined, which is 223,004 fewer cases than in the United States.
Four rapidly expanding “hot spot” countries are India with 118,226 infections and 6,198 new infections on 5/21/20, Peru with 108,769 infections and 4,749 new infections, Russia had 317,554 infections and 8,849 new infections on 5/21/20, and Brazil had 310,921 infections and 17,564 new infections. Today we’ll focus our discussion on the State of California and Monterey County.
State of California
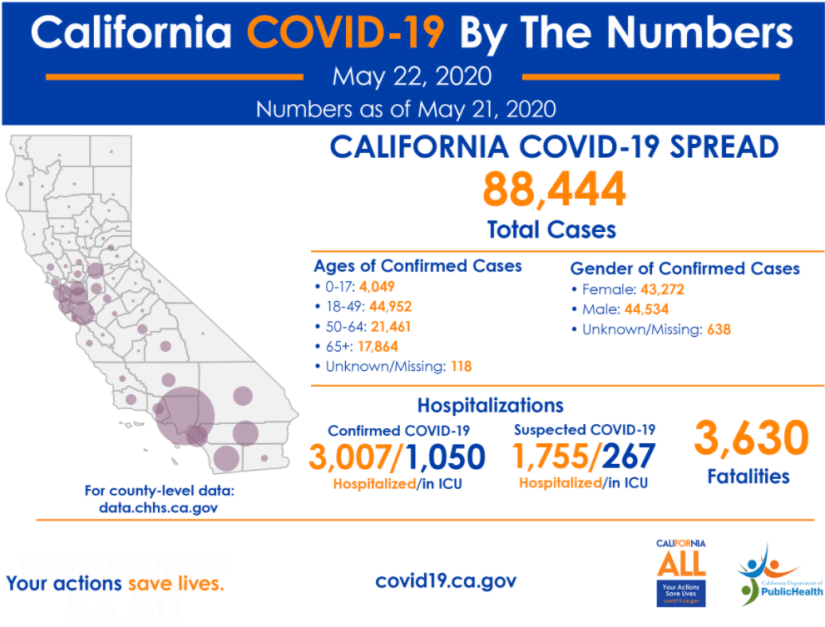
As of 5/21/20, the State of California has 88,488 total infections, 3,624 new infections, 3,624 total deaths and 110 new deaths. On 5/21/20, California had more new deaths than any other state, with the exception of New York and was 7th in total deaths in the United States, having just surpassed Connecticut’s deaths. On 5/21/20, California reported 4,735 hospitalized COVID-19 patients (on that day) and 1,310 patients in the ICU. If California were a country, it would rank 13th in total number of cases in the world (above China) and 17th in total deaths (between Russia and India). It would rank 10th in new deaths in the world on 5/21/20. It would rank 7th in the world in ICU patients (between Spain and the UK). As of 5/21/20, California reported conducting 1,421,127 COVID-19 tests, which represents 3.57% of California’s population of 39.78 million. However, we know that some people have been tested more than once, so in fact, less that 3.57% of the population has been tested for COVID-19.
So what can these numbers suggest to us about what public policies would be prudent at this time for California? Here’s what we think:
Keep School Buildings Closed to Protect Youth and the Elderly
From the beginning of the pandemic, it was messaged to us by public health officials and politicians alike that COVID-19 disproportionately affects folks 65 and over and those with underlying health conditions, leading young healthy folks to believe that they would not be infected or become seriously ill. This made it more difficult for young working people to accept the stay-at-home order as the new way of life, and many are counting down the days, hours, and minutes until they can return to work in person, get their hair and nails done, and return to their local bars, restaurants, gyms, and sporting events.
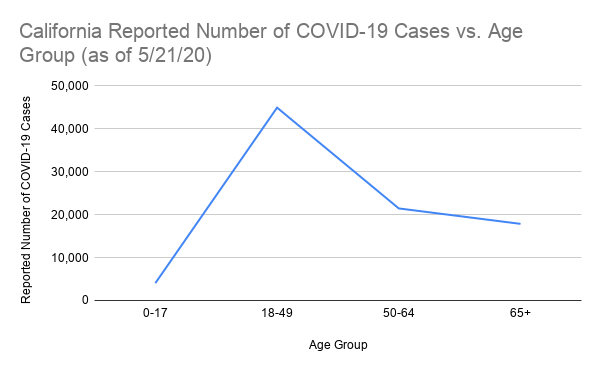
However, if we look at the data on which age groups are most affected by COVID-19, we see a much different picture. In California, as of 5/21/20, the age group with the largest number of confirmed infections is people 18-49 years of age, with 44,953 infections, compared to 21,461 people 50-64 and 17,864 people 65 and up. The 0-17 age group has 4,049 cases. (Incidentally, the 0-17 age group is also the least-tested group.) We know that 7,908 of those 65+ folks are residents in skilled nursing facilities are infected with COVID-19, so when you take those folks out of the equation, there are only 9,956 other people over the age of 65 infected in California. Deaths in skilled nursing facilities make up 39.5% of the COVID-19 deaths in California. The point is that people over 65 who are not in skilled nursing facilities are not getting infected at the same rate as younger people. Now, it might be a coincidence, but we can’t help noticing that the two age groups that we have essentially mandated stay home since mid-March (school-aged children and senior citizens) have the lowest numbers of infections. Perhaps preventing infections is not as complicated as folks are making it out to be.
A standard Influenza respiratory epidemic has a U-shaped death curve (see dotted line 1911-1917 curve below), meaning that you have very young and very old people dying. What happened in the 1918 Influenza pandemic is that they had a W-shaped curve (see solid line below). The peak in the middle happened to be people between the ages of 20 and 40.
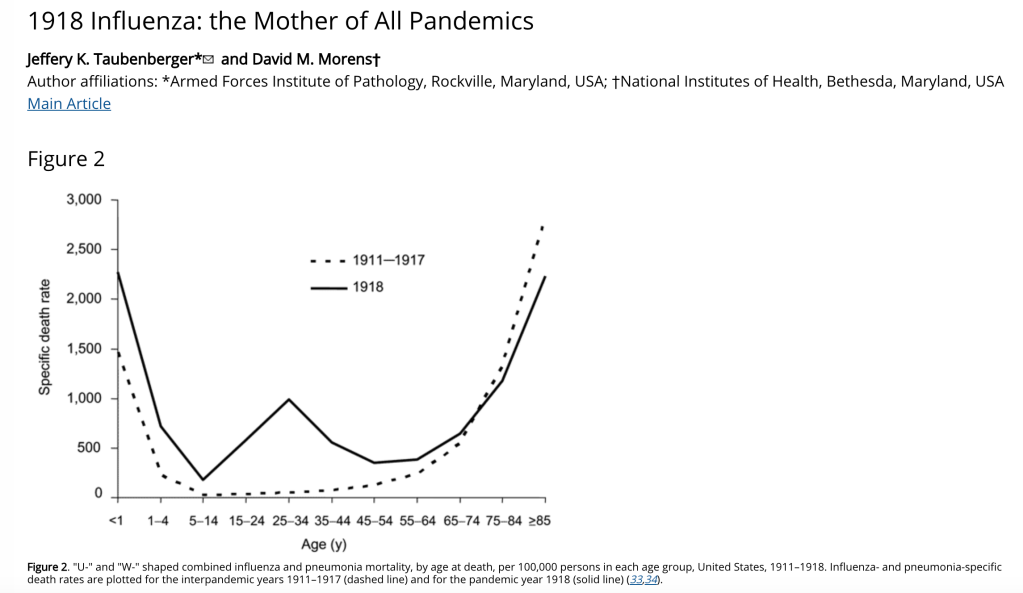
If we look at the data from the 2020 COVID-19 pandemic in California, plotted by age group, we can see some similarities and some key differences from the 1918 pandemic. By closing schools and telling older people to stay home in California, we’ve decreased the number of COVID-19 cases in both groups, effectively losing the left arm of the W and flattening out the right arm from the 1918 Influenza graph.
Thanks to early implementation in California of non-essential business closures, school closures, stay-at-home policies, social distancing, and use of masks, we’ve been able to avoid some of the hardships that folks experienced in the 1918 Influenza pandemic.
However, social distancing is not possible in schools–period. Getting children to wear masks safely and wash their hands with soap and warm water before touching their faces, their food, or their classmates is impossible. We won’t even go into how difficult it would be to keep student bathrooms sanitary. Moreover, large class sizes and inadequate ventilation systems (both of which are the norm in California public schools) are not conducive to safe social distancing. In order to make classrooms workable for social distancing, California schools would likely have to triple their teaching staffs, expand facilities, and spend millions of dollars updating air conditioning systems and adding HEPA filter systems. Furthermore, we’ve already been told that school budget cuts are inevitable at this point. Therefore, from our perspective, the only solution for safely educating our children during the next two years of this epidemic would be distance learning. Many school districts are currently surveying parents to collect their input on plans for the upcoming school year. Parents would be prudent to request that their districts offer distance learning for students of all ages.
Wear a Mask in Public
All people should wear masks in public at all times. There is very compelling scientific evidence that masks decrease the incidence of respiratory infections by preventing people’s respiratory droplets from circulating in shared air. We can see correlations between mandated mask-wearing policies and lower numbers of COVID-19 infections and deaths in countries across Asia like Japan, Vietnam, and Taiwan. There are certainly other factors in play that have helped these nations control the spread of COVID-19, like having more socially-distant ways of greeting people, better early education campaigns for COVID-19, prior experience with the SARS epidemic, increased travel restrictions, experimental pharmaceutical interventions (like Japan’s favipiravir) and better contact tracing. However, it’s worth noting that in some countries where most of these factors were not present, masks have been a game-changer, keeping cases and deaths relatively low. Take, for example, the Czech Republic, which mandated face masks in public in late March (along with closing borders, prohibiting public gatherings, and shuttering non-essential businesses). With a population of approximately 10 million, as of 5/23/20, Czechia (as it is also known) had 8,890 total reported cases of COVID-19 and just 314 total deaths. That’s 830 cases per million people and 29 deaths per million, and constitutes a death rate of about 3.5%. In Portugal, whose population is also around 10 million, masks in public were recommended but not required back in April. As of 5/23/20, Portugal had 30,471 total reported cases and 1,302 total deaths. That’s 2,987 cases per million people and 128 deaths per million, for a death rate of 4.3%. Even if we rewind to May 1, before Portugal began partially reopening businesses, we see it had a total of 24,987 cases and 1,007 deaths (death rate 4%), which is 2,450 cases per million and 99 deaths per million. Compare this to Czechia on May 1 with 7,737 total cases and 240 deaths (death rate 3.1%) That’s 722 cases per million and 22 deaths per million. This is not to say we think that mandated mask wearing is solely responsible for the differences in Portugal and Czechia’s numbers, but it certainly couldn’t hurt.
Avoid Gathering in Enclosed Spaces, Regardless of Restriction Easing
Biologist Erin Bromage from the University of Massachusetts Dartmouth makes some valid points about infection risk in her blog post published on May 6, which was inspired by Jonathan Kay’s April 23 piece in Quillette on COVID-19 superspreader events. We won’t go into detail on the specifics of superspreader events in our post today, but we do have a few things to say about what you can do to stay safe as cities begin to reopen selected businesses and public spaces.
The keys to preventing transmission of infection are personal protective equipment, washing hands with soap and warm water, and adequate ventilation. Unfortunately, most businesses and public buildings, like schools (see above), restaurants, bars, gyms, and salons (and even many doctor’s offices and hospitals) do not have the HEPA filtered air systems that are required to prevent the spread of COVID-19 and other viruses like influenza. Sanitizing surfaces, erecting barriers, setting up fans, and opening windows will not resolve the air issues in these locations. The reality is, there are few safe buildings when it comes to COVID-19.
So what are our recommendations for folks who are determined to dine out, get a haircut, join a yoga class, or attend a religious service as soon as their local governments allow it?
Small businesses need to rethink how they provide services to their patrons. Restaurants, rather than looking for ways to make poorly-ventilated indoor dining rooms safer, should be focused on offering outdoor dining. Hairdressers, barbers, and nail technicians should consider making use of their parking lots to provide their services in the open air, or performing services for their clients in their backyards. Gym owners, likewise, could look for opportunities to move classes outdoors.
Places of worship should continue to offer services online and should consider outdoor services, where people should wear masks and stay six feet apart. Drive-in services might also be possible for churches with large parking lots, leaving at least one parking space vacant between cars. Of course, some practices, like the distribution of wafers and grape juice or wine for communion, would remain high-risk, whether conducted indoors or outdoors. The bottom line is it’s not safe to be in a public place near people from outside your household who are eating, talking, or singing without wearing masks.
If you’re going to be around people from outside your household and have the choice to do so outdoors rather than indoors, outdoors would be a significantly safer choice. This is not to say that it’s prudent to have a large backyard barbecue or any large gathering of people outdoors. It’s still best to limit gatherings to no more than 10 people. Stick to video chatting with friends and family who have high risk for exposure to COVID-19 (like essential workers).
Monterey County
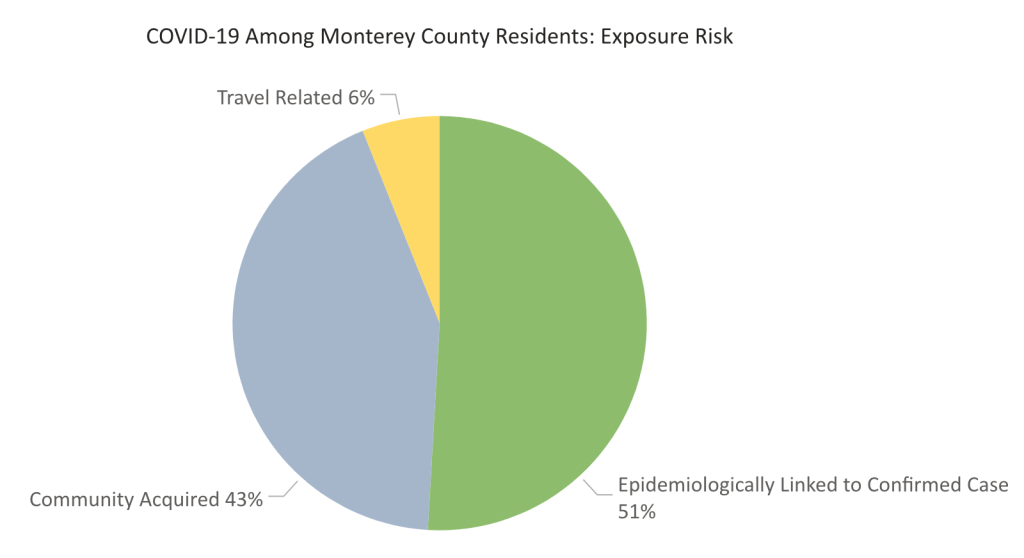
In Monterey County, 40% of the infections are in folks who work in agriculture and 9% of infections are in health care workers and first responders. In 210 (57%) of the cases, patients had no known pre-existing medical conditions. How are people getting infected? In Monterey County, 51% of reported cases are epidemiologically linked to a confirmed case, 43% of cases are community acquired, and 6% are travel-related. In theory, if a county is doing an excellent job of contact tracing, the percentage of community acquired cases would be very low–because cases would be quickly identified and folks could be quarantined before infecting others. The fact that 43% of the cases in our county are community acquired suggests we should be doing better case contact tracing and increase testing for everyone, but especially for essential workers, particularly those who come in close contact with the public. We ought to be testing all agricultural workers, health care workers, and first responders.

In California, the state public health department reports infections and deaths in skilled nursing facilities. It’s worth noting that since April 23, on any given day, only between 81% and 95% of California’s skilled nursing facilities have reported their COVID-19 cases and deaths to the state health department. On its website, California Department of Health lists data for COVID-19 infections and deaths for 16 of Monterey County’s skilled nursing facilities. Based on this data, one 103-bed facility, Windsor The Ridge Rehabilitation Center in Salinas (zip code 93906) has reported cases in health care workers and patients. They are also listed as having patient deaths. Because the state of California does not report specific numbers of deaths and cases in skilled nursing facilities unless the number is greater than 11, we do not know how many of the cases and deaths in our county are associated with this facility–the report says fewer than 11. We also reviewed the California Department of Health skilled nursing COVID-19 data base (May11, 2020) and found a total of nine Windsor facilities in California with COVID-19 cases. The site with the most infections was in Solano County where 25 healthcare workers and 60 patients were infected with fewer than 11 deaths. The Monterey County Health Department has not disclosed the number of cases or deaths in the Salinas skilled nursing facility in our county. This data should be made available to the public. In addition, if it has not already been done, all staff and patients at this facility should be tested for COVID-19 by PCR on a routine basis. The state of New York has mandated that each nursing home will test each healthcare provider twice a week for COVID-19. This seems a reasonable approach to any facility with any healthcare provider or patient infection. A more proactive approach would be to test all healthcare providers and patients in skilled nursing facilities.
Our Updated COVID-19 Projections
The University of Washington’s Institute of Health Metrics (IHME) said on 4/28/20 that we would have a total of 74,000 deaths in the USA by August 5, 2020. In contrast to this, we analyzed the case and death data using our two methods again on 5/22/20. We estimated that we will reach 2,000,000 infected patients by June 7th (in 15.4 days, 369 hours or 2.2 weeks) and have between 17,710 and 20,513 new deaths for a total number of deaths between 115,357 and 118,156.
All of our predictions from 4/28/20, 5/03/20, 5/08/20 and 5/22/20 for time to reach 2,000,000 infections and the estimate of the number of deaths are listed in the following chart:

A few weeks ago, the University of Washington re-projected the number of deaths by August 4, 2020 to be 134,475. When we checked their website on 5/23/20, they had revised this number to 143,357. (Musical chairs, anyone?)
We don’t usually project out 2 months for total infections and deaths, but if we did, using our methodologies, we would predict that by August 4, 2020 in the United States we will have 3,337,190 COVID-19 infected patients and a total of between 192,613 and 199,229 deaths. If the death rate (now 5.94%) increases, these estimates of the number of deaths will be too low.
On 5/01/20, the FDA finally approved Gilead’s Remdesivir for intravenous treatment of COVID-19 infected patients. Since we initially recommended approval of this drug, another 97,600 Americans have died. Gilead is donating a large amount of drug for free. Unfortunately, it now appears that the government will be involved in the distribution of the drug, which means that university medical centers, hospitals in rural counties, and outpatient clinics like ours will probably not have the opportunity to treat our patients with Remdesivir. If it were up to us, this drug would be sold through normal drug distribution channels. Hopefully use of Remdesivir and/or plasma therapy will alter reported deaths in the next two months. We’re not optimistic based on the United States government’s performance during the first 145 days of the COVID-19 pandemic.
We have no effective available oral treatment or preventative drugs, vaccines or hyperimmune intravenous immunoglobulin for COVID-19. Potential therapies are probably 6 to 9 months away. In the United States our political leaders (the President and most Governors) and federal agencies (HHS, CDC) and many state public health officials have decided to open back up our country. Viruses (COVID-19, Influenza and perhaps measles) will have many more potential victims this year.
Please think globally and act locally.
Recommended Reading
We Cannot Return to Campus This Fall https://thebolditalic.com/we-cannot-return-to-campus-this-fall-1ad91b8a65e0
1918 Influenza: the Mother of All Pandemics (Emerging Infectious Diseases) https://wwwnc.cdc.gov/eid/article/12/1/05-0979_article
American Pandemic: The Lost Worlds of the 1918 Influenza Epidemic by Nancy K. Bristow https://www.goodreads.com/book/show/13540533-american-pandemic
The Great Influenza: The Story of the Deadliest Pandemic in History by John M. Barry https://www.goodreads.com/book/show/29036.The_Great_Influenza?ac=1&from_search=true&qid=9DWUInOM10&rank=1
The Complex Question of Reopening Schools (The New Yorker) https://www.newyorker.com/magazine/2020/06/01/the-complex-question-of-reopening-schools
Public Health Experts Say Many States Are Opening Too Soon To Do So Safely (NPR) https://www.npr.org/2020/05/09/853052174/public-health-experts-say-many-states-are-opening-too-soon-to-do-so-safely
This Japanese Island Lifted Its Coronavirus Lockdown Too Soon and Became a Warning to the World (Time) https://time.com/5826918/hokkaido-coronavirus-lockdown/
Tired Of Wearing A Face Mask In Public? New Research Underscores Why You Still Need To (Forbes) https://www.forbes.com/sites/brucelee/2020/05/14/here-is-more-evidence-for-face-mask-use-with-covid-19-coronavirus/#30c0654b1060
The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission (PNAS) https://www.pnas.org/content/early/2020/05/12/2006874117
Hearts and masks: Czech-Vietnamese solidarity during coronavirus https://www.aljazeera.com/indepth/features/hearts-masks-czech-vietnamese-solidarity-coronavirus-200407101254028.html
California is publicly sharing incomplete data on coronavirus outbreaks at nursing homes (SF Chronicle) https://www.sfchronicle.com/bayarea/article/California-s-method-of-reporting-coronavirus-15258007.php
2019 Novel Coronavirus (2019-NCoV) – Local Data (Monterey County Public Health) https://www.co.monterey.ca.us/government/departments-a-h/health/diseases/2019-novel-coronavirus-covid-19/2019-novel-coronavirus-2019-ncov-local-data-10219

You must be logged in to post a comment.