
It’s time for our next 14-day moving average determinations for SARS-CoV-2 for the United States and my thoughts on vaccines, SARS-CoV-2 therapeutic agents and mutant viruses. We use the WORLDOMETERS aggregators data set to make any projections since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.



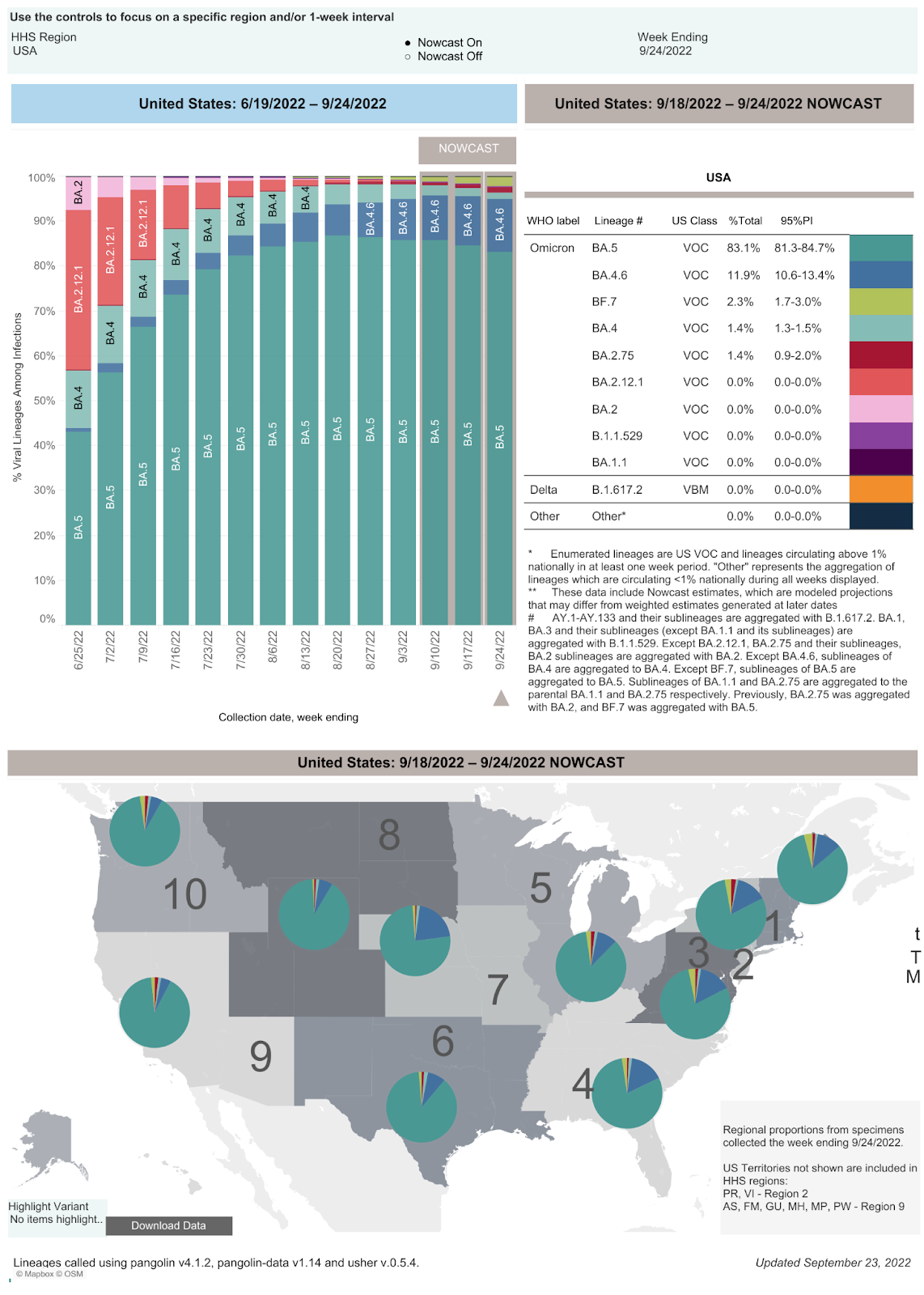
SARS-CoV-2 infections per day in the United States have decreased for the second time in four weeks; however, there is still widespread underreporting by states, a failure to capture positive home tests, and a decreased PCR screening program in most states. Deaths per day in the United States have decreased by 14 deaths per day. The number of infections per day has decreased by 19,313. The CDC estimates that BA.5 accounted for 83.1%, BA.4.6 accounted for 11.9%, BF.7 accounted for 2.3%, BA.4 accounted for 1.4%, BA.2.12.1 accounted for 0.0% of isolates, BA.2 accounted for 0.0%, BA.1.1 accounted for 0.0%, and B.1.1.529 accounted for 0% in the week ending September 10. The rise in BA.4.6 cases is especially concerning because the September 9 UK Security Agency Technical Briefing says that, “Pseudoviral neutralisation assays performed on BA.4.6 show that titres are reduced 2-fold, compared to neutralisation of BA.4 or BA.5 using sera from triple dosed recipients of the Pfizer BNT162b2 vaccine.” The same briefing also states that BA.4.6 has a growth advantage relative to BA.5.
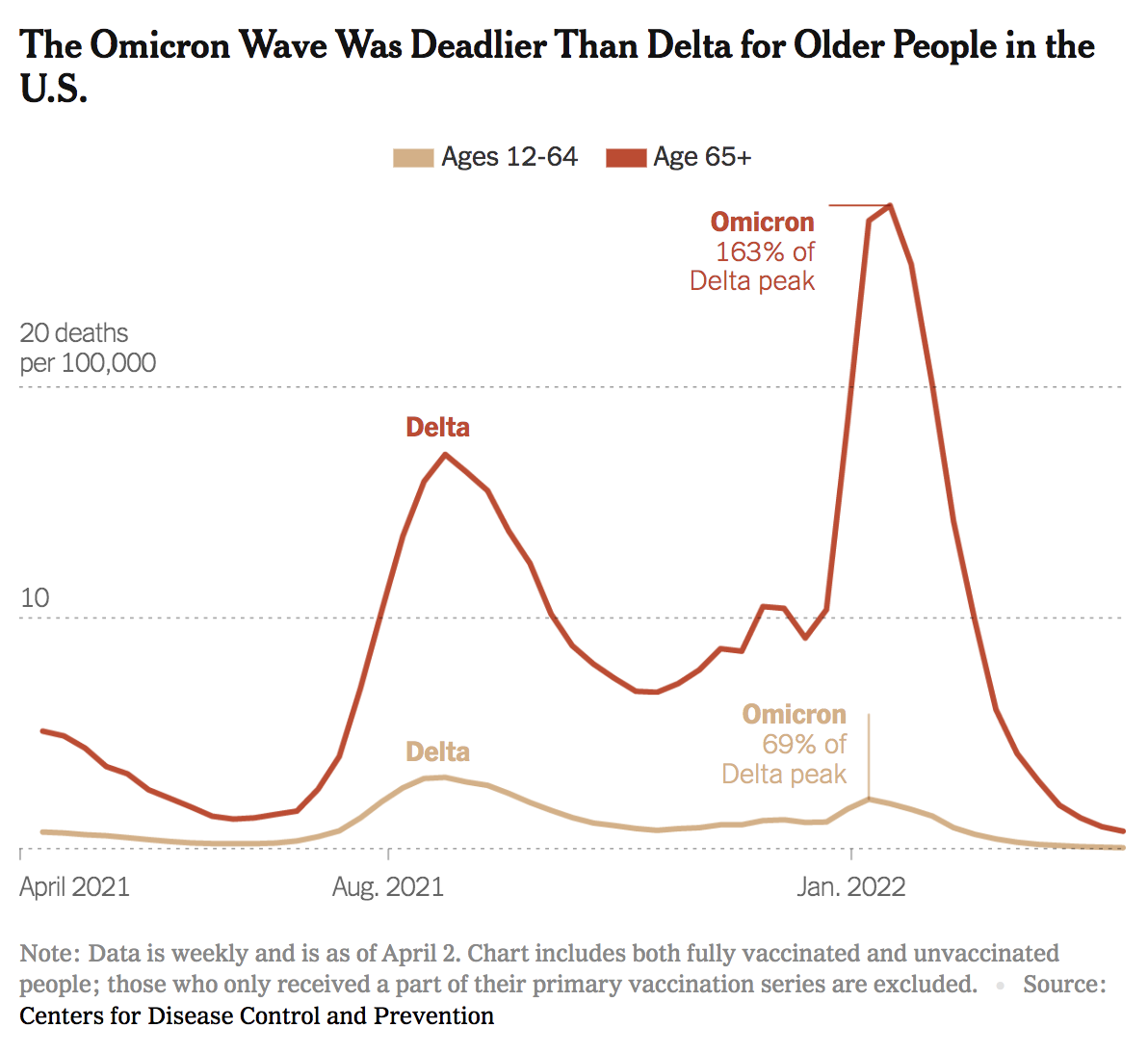
We frequently hear messaging from health officials and politicians that Omicron is “mild,” especially compared to the Delta variant, and as a result, many of our patients believe that they no longer need to wear their masks. This is a dangerous misconception. SARS-CoV-2 still remains a highly transmissible, airborne virus. The following graph, based on CDC data from April 2, 2022, shows that Omicron deaths in people over 65 are much higher than Delta deaths in the same age group. In fact, the peak of Omicron deaths in people over 65 years of age is 163% higher than the Delta peak. The death rate from Omicron is only lower than Delta in the populations between 12 and 64 years of age. Until we have more data on these newer mutants of SARS-CoV-2, we will not know the lethality of each variant. It may take months to measure objective differences in the death rates of new circulating variants. We recommend that all of our patients and family members continue to wear N95 masks in all enclosed spaces.
In patients treated with Paxlovid for five days who have persistent symptoms and continued positivity, we feel that clinicians should consider giving a second course of Paxlovid for five days. Boucau et al have demonstrated that in a study of seven patients with recurrent symptoms, “High viral loads (median 6.1 log10 copies/mL) were detected after rebound for a median of 17 days after initial diagnosis. Three had culturable virus for up to 16 days after initial diagnosis.” This was not due to resistance-associated mutations of the virus, suggesting that the course of therapy may be inadequate in this group of persistently infected patients.
The Omicron variant has continued to mutate just like Delta. The list of variants was not updated in the last four weeks, but as of six weeks ago, there are now 276 Omicron sub-variants that have been assigned Pango lineages, including 123 sub-lineages of BA.2, one sub-lineage of BA.3, 15 sub-lineages of BA.4, and 45 sub-lineages of BA.5. The BF lineage (new fourteen weeks ago) now has 21 sublineages.. The BE lineage (also new fourteen weeks ago), with BE.1 first detected in South Africa, Austria and England, now has 7 sublineages. There are also new lineages from fourteen weeks ago: BC.1 (Japan), BC.2 (Peru), BD.1 (UK), BG.1 (Peru), BG.2 (US, Denmark, Canada), BG.3 (Peru), BG.4 (Israel). In the last six weeks, the BG lineage has expanded to include BG.5 (USA) and BG.6 (Peru). Lastly, two new sublineages were added in the past six weeks: BH.1 (India) and BK.1 (USA and Canada).
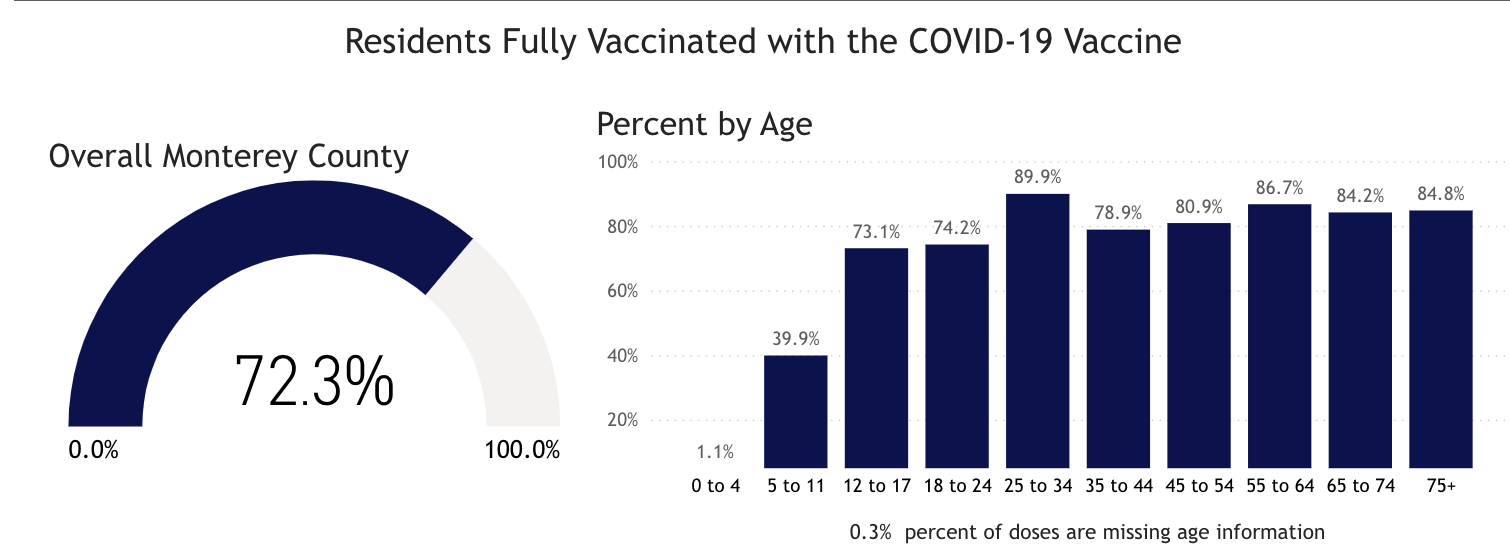
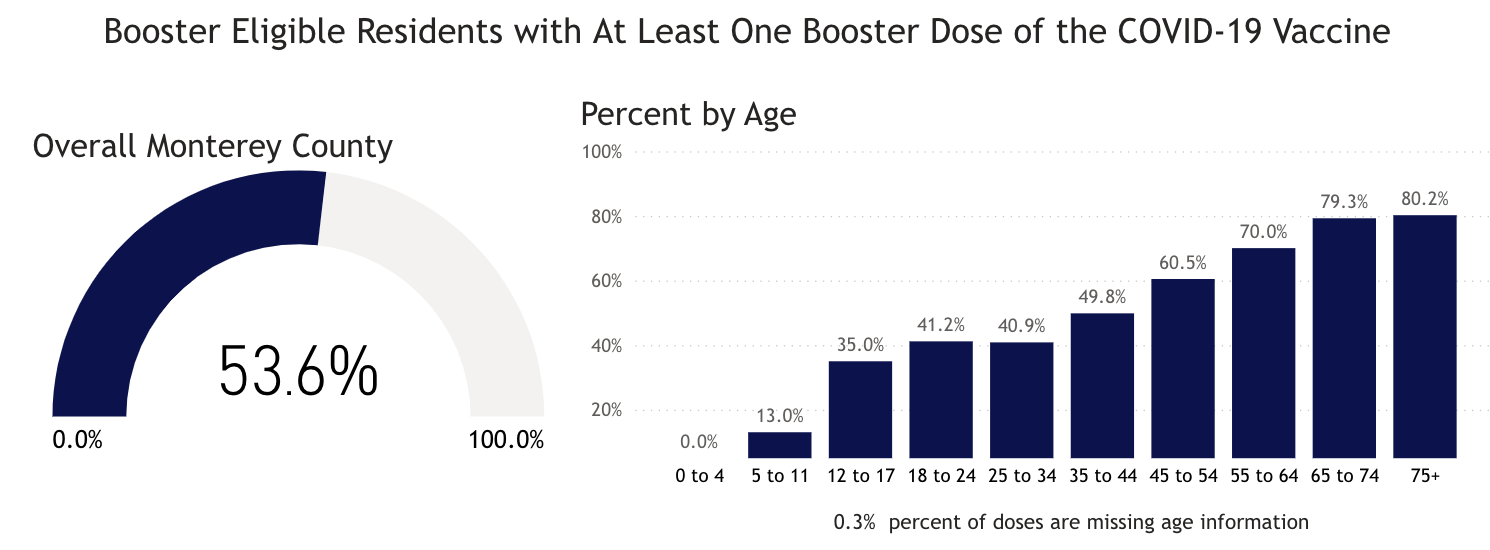
In Monterey County, as of 9/24/22, 1.1% of 0-4 year-olds and 39.9% of 5-11 year-olds have received the first two doses of vaccine, while 73.1% of 12-17 year-olds have received two doses. Only 53.6% of Monterey County residents have received a third dose of the vaccine. On June 17, The FDA authorized both the Pfizer and Moderna vaccines for use in children ages 6 months to four years. We believe children under 5 should be vaccinated as soon as possible. All Monterey County residents should get up to date on COVID-19 vaccinations as soon as possible.
On 9/23/22, the United States had 33,238 documented new infections. There were also 259 deaths. Twenty-six states did not report their infections, and 30 states didn’t report their deaths. In the United States the number of hospitalized patients has decreased slightly in many areas and was 30,273 on September 24, a decrease of 6,417 hospitalizations compared to the previous 14 days. On 9/14/22 there are 3,176 patients who are seriously or critically ill; that number was 3,829 two weeks ago. The number of critically ill patients has decreased by 653 in the last 14 days, while at least 5,228 new deaths occurred. The number of critically ill patients has decreased for the fourth time in twenty-eight 14-day periods. Patients are still dying each day (average 375/day). Omicron BA.4, BA.4.6 and BA.5 variants are still causing infections. Past infections with a BA.1 or BA.2 variant will not prevent infections with BA.4, BA.4.6 or BA.5. Evusheld may not prevent BA.4.6 infections.
As of 9/23/22, we have had 1,081,566 deaths and 97,880,451 SARS-CoV-2 infections in the United States. We have had 854,450 new infections in the last 14 days. We are adding an average of 427,225 new infections every seven days. For the pandemic in the United States we are averaging one death for every 90.48 infections or over 11,050 deaths for each one million infections. As of 9/23/22, thirty-eight states have had greater than 500,000 total infections, and 38 states have had greater than 5,000 total deaths. Forty-six states have had greater than 2,000 deaths, and 43 states have greater than 2,000 deaths per million population. Vermont, at 1,152 deaths per million, and Hawaii, 1,186 deaths per million, are the states with the lowest death rates. Six states have over 4,000 deaths per million population: Mississippi (4,327), Arizona (4,304), Alabama (4,160), West Virginia (4,119), New Mexico (4,079) and Tennessee (4,057). Eighteen states (Alabama, Virginia, Missouri, North Carolina, Indiana, Tennessee, Massachusetts, Ohio, Michigan, Georgia, Illinois, New Jersey, Pennsylvania, Florida, Texas, New York, Arizona and California) have had greater than 20,000 deaths. Four states have had greater than 70,000 deaths: Florida (81,139 deaths), Texas (91,159 deaths), New York (72,058 deaths), and California (95,970 deaths, 20th most deaths in the world).
On 11/20/20, there were 260,331 (cumulative) deaths in the US from SARS-CoV-2. Since 11/20/20 (22 months), there were 820,435 new deaths from SARS-CoV-2. For eighteen of those months, vaccines have been available to all adults. During these eighteen months, 509,469 people have died of SARS-CoV-2 infections. Most of the hospitalizations and deaths could have been prevented by vaccination, proper masking, and social distancing.
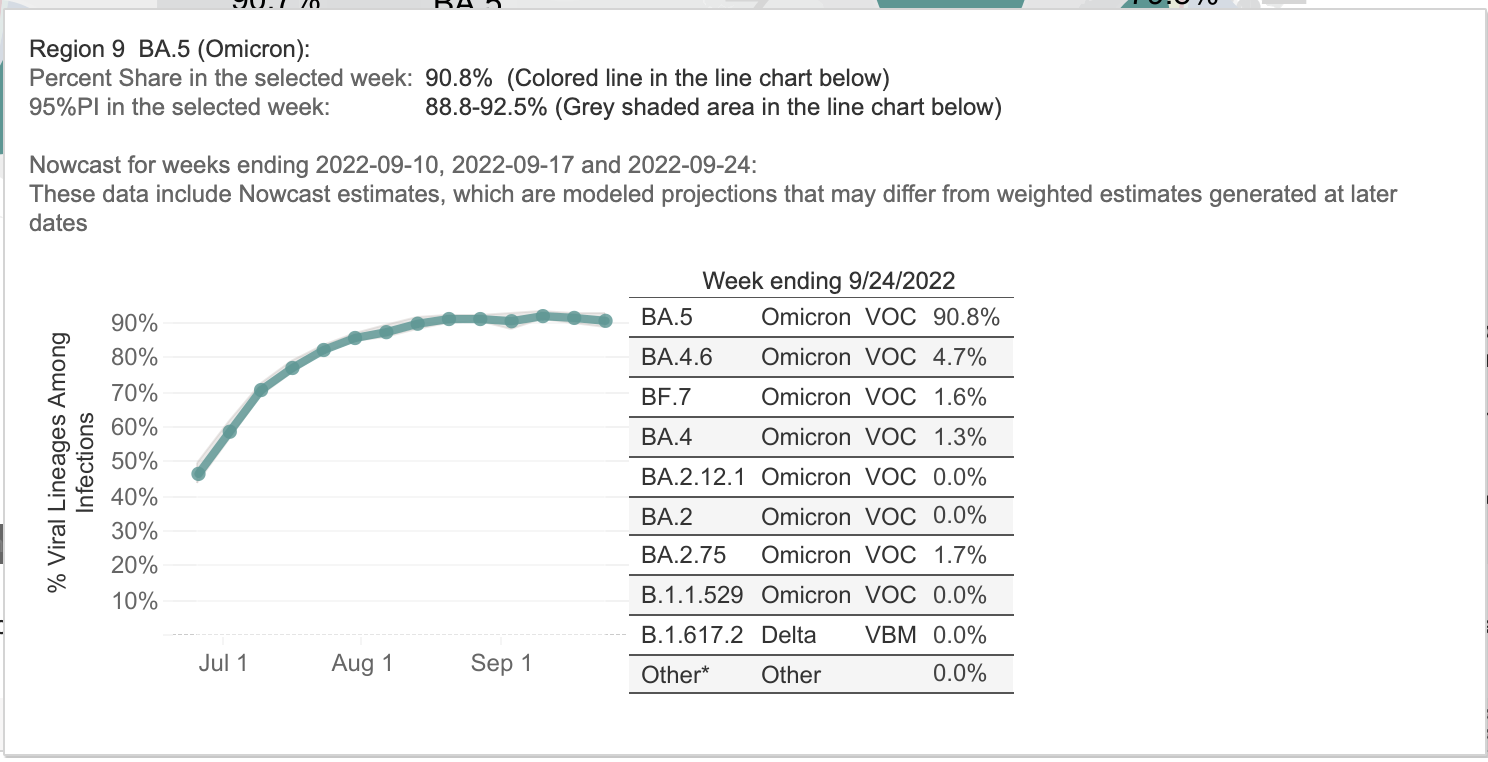
As of 9/23/22, California was ranked 32nd in the USA in infection percentage at 28.40%. In California, 24.43% of people were infected in the last 19 months. As of 9/23/22, 43 states have had greater than 25% of their population infected. No state has less than 20% of their population infected. Below are the variant proportions for Region 9, which includes California, Nevada, and Arizona.
Worldwide, average deaths per day are 1,737 for the last 14 days, which is a 340 deaths-per-day decrease over the previous 14 days. The United States accounts for 21.58% (375 per day) of all deaths per day in the world over the last two weeks. Worldwide infections per day were 474,827. The United States accounts for 12.854% of those infections (or 61,032 infections per day).
FDA-Approved Oral Drug Treatments for SARS-CoV-2
Pfizer has developed PAXLOVID™, an oral reversible inhibitor of C3-like protease of SARS-CoV-2. The drug inhibits this key enzyme that is crucial for virus production. The compound, also called Compound 6 (PF-07321332), is part of the drug combination PAXLOVID™ (PF-07321332; ritonavir), which just successfully completed a Phase 2-3 trial in humans in multiple countries. The preliminary results were announced on 11/5/21 by Pfizer. The results show that 89% of the hospitalizations and deaths were prevented in the drug treatment arm. The drug was administered twice a day for five days. No deaths occurred in the treatment group, and ten deaths occurred in the placebo group. The study was stopped by an independent data safety monitoring board, and the FDA concurred with this decision. Pfizer applied for an Emergency Use Authorization for this drug on 11/15/21. This drug was approved on 12/23/21. We have only been able to obtain PAXLOVID™ for two patients who we successfully treated with this drug obtained from CVS in Salinas (East Alisal Street; phone number 831-424-0026). They were expecting another shipment on 1/28/22. In my opinion, this agent, if more widely available, could markedly alter the course of every coronavirus infection throughout the world.
Merck has developed the oral drug Molnupiravir, which induces RNA mutagenesis by viral RNA-dependent RNA polymerase of SARS-CoV-2 and other viruses. According to Kabinger et al, “Viral RNA-dependent RNA polymerase uses the active form of Molnupiravir, β-D-N4-hydroxycytidine triphosphate, as a substrate instead of cytidine triphosphate or uridine triphosphate. When the RNA-dependent RNA polymerase uses the resulting RNA as a template, β-D-N4-hydroxycytidine triphosphate directs incorporation of either guanine or adenine, leading to mutated (viral) RNA products. Analysis of RNA-dependent RNA polymerase–RNA complexes that contain mutagenesis products has demonstrated that β-D-N4-hydroxycytidine (the active form of Molnupiravir) can form stable base pairs with either guanine or adenine in RNA-dependent RNA polymerase explaining how the polymerase escapes proofreading and synthesizes mutated RNA” (quotation modified for clarity). The results of the phase 3 trial of Molnupiravir were published in the NEJM article “Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients” by Angélica Jayk Bernal, M.D. et al. (December 16, 2021 DOI: 10.1056/NEJMoa2116044). In this phase 3 study in the Molnupiravir group, 28 patients were hospitalized and one death occurred. In the placebo group, 53 patients were hospitalized and 9 died. Overall, 47% of hospitalizations and deaths were prevented by Molnupiravir. If you do a post hoc analysis and just look at deaths, Molnupiravir would prevent 89% of deaths. An Emergency Use Authorization by the FDA for Molnupiravir was approved on 12/24/21.The dose of Molnupiravir approved is four 200 mg capsules orally twice a day for five days. Diarrhea is reportedly a side effect in two percent of patients. I treated my first patient with Molnupiravir on 1/28/22. Currently more Molnupiravir is available weekly in the United States than PAXLOVID™ (see chart below; data from PHE.gov). Locally Molnupiravir is still available at CVS in Monterey (Fremont Blvd.; phone number: 831-375-5135) and CVS in Salinas (East Alisal Street; phone number 831-424-0026).
FDA-Approved Intravenous Monoclonal Antibody Treatment for Non-Hospitalized SARS-CoV-2 Patients
Bebtelovimab is a monoclonal antibody treatment for mild-to-moderate COVID-19 in adults and pediatric patients (12 years of age and older weighing at least 40 kg) with positive results of direct SARS-CoV-2 viral testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death, and for whom alternative COVID-19 treatment options approved or authorized by FDA are not accessible or clinically appropriate. The authorized dose of bebtelovimab is 175 mg, given as an intravenous injection over at least 30 seconds. The U.S. Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for this drug on 2/11/22. Bebtelovimab is a human antibody that demonstrates neutralization against the Omicron variants and is available in every state and many hospitals and some clinics. If you are planning on using a monoclonal antibody to treat a SARS-CoV-2 infection, currently only bebtelovimab has activity against all Omicron variants, including BA.4.6. Researchers at Columbia University recently reported that “The loss of activity of tixagevimab and cilgavimab [components of Evusheld] against BA.4.6 leaves us with bebtelovimab as the only therapeutic mAb that has retained potent activity against all circulating forms of SARS-CoV-2.” For this reason, we no longer recommend Evusheld for immunocompromised patients with Omicron infections.

An examination of the three variants that Wang et al identified as capable of immune escape in patients who receive the two monoclonal antibodies that are contained in Evusheld reveals that all three variants have a mutation in the spike protein at position 346. The changes substitute an uncharged amino acid— threonine (T), serine (S), or isoleucine (I)—for a positively-charged amino acid, arginine. This just goes to show that a single point mutation in the spike protein can render a monoclonal antibody treatment ineffective. Policy makers should keep in mind that the only way to prevent new drug-resistant variants like BA.4.6 from emerging is to prevent transmission of SARS-CoV-2 in the first place, using non-pharmaceutical interventions. The lack of use of N95 masks, with impending winter and influenza outbreaks, on top of COVID-19, is not wise public health and infectious disease policy. If we don’t make effective use of the non-pharmaceutical interventions available to us (masks, ventilation, social distancing), then the pharmaceutical interventions we have will all eventually be useless.
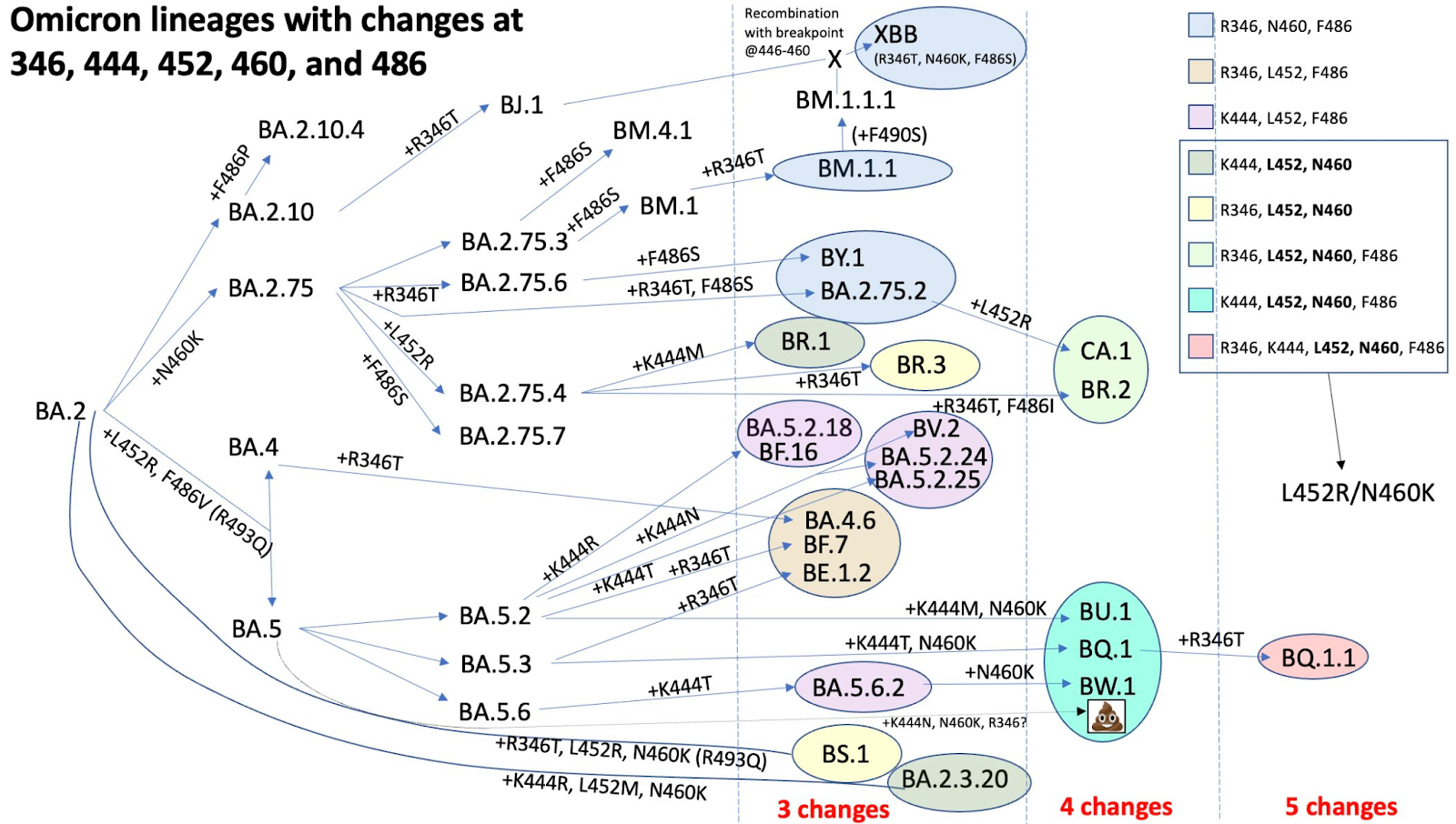
Two virologists collaborated on Twitter to create the figure below, which Professor Johnson titled “Convergent Evolution on Steroids.” It shows the key mutations present in many of the currently-circulating Omicron subvariants and demonstrates that mutation at site 346 is becoming more and more common. This means that even if prevalence of BA.4.6 wanes, we are still likely to have drug resistance issues with other newer variants.
Watching World Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments. Data on infections, deaths, and percent of population infected was compiled from Worldometers. Data for this table for SARS-CoV-2 Isolates Currently Known in Location was compiled from GISAID and the CDC. It’s worth noting that GISAID provided more data than the CDC.
| Location | Total Infections as of 9/23/22 | New Infections on 9/23/22 | Total Deaths | New Deaths on 9/23/22 | % of Pop.Infected | SARS-CoV-2 Isolates Currently Known in Location | National/ State Mask Mandate | Currently in Lockdown |
| World | 619,585,969(6,647,575 new infections in 14 days). | 410,558 | 6,538,850(24,324 new deaths in last 14 days) | 1,312 | 7.94% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)A lineage isolateV01.V2 (Tanzania)APTK India VOC 32421Delta/B.1.617.2 (India)BV-1 (Texas, USA)Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Theta/P.3 (Philippines) Mu/B.1.621 (Colombia)C.1.2 (South Africa 2% of isolates in July 2021)R1 (Japan)Omicron/B.1.1.529 + BA.1 + BA.2 + BA.3 (South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)Four new recombinants 12/31 to 3/22)BA.2.12.1 (USA)BA.4 (South Africa)BA.5 (South Africa)BA.2.75 (India 7/22)BA.4.6 (USA 7/22) | No | No |
| USA | 97,880,451(ranked #1) 854,450 new infections in the last 14 days. | 33,238(ranked #5) 26 states failed to report infections on 9/23/22. | 1,081,566(ranked #1) 5,228 new deaths reported in the last 14 days. | 259 30 states failed to report deaths on 9/23/22. | 29.57% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)BV-1 (Texas, USA)Theta/P.3 (Philippines) Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)R1(Japan) Omicron/B.1.1.529 + BA.1 + BA.2 (South Africa November 2021)B.1.640.1 (Congo/France)Recombinant Delta AY.119.2- Omicron BA.1.1 (Tennessee, USA 12/31/21)\BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22)BA.4.6 (USA 7/22) | No | No |
| Brazil | 34,666,387(ranked #4) 129,467 new infections in the last 14 days. | 6,861 | 685,816(ranked #2; 950 new deaths in 14 days) | 91 | 16.05% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Zeta/P.2 (Brazil)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21) | No | No |
| India | 44,563,337(ranked #2); 73,054 new infections in 2 weeks. | 4,912 | 528,487(ranked #3) 348 new deaths in 2 weeks. | 38 | 3.16% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)APTK India VOI 32421Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India)Iota/B.1.526 (USA-NYC) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India) | No | No |
| United Kingdom | 23,621,952(ranked #7) 67,433 new infections in 2 weeks. | – | 189,919 (ranked #7) 893 new deaths in 2 weeks | – | 34.39% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Epsilon/B.1.427 + B.1.429 (USA)*Gamma/P.1 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)C.1.2 (South Africa)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)XD (AY.4/BA.1) recombinantXF (Delta/BA.1) recombinantXE (BA.1/BA.2) recombinantBA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22) | No | No |
| California, USA | 11,228,790(ranked #14 in the world; 100,708 new infections in the last 14 days). | 1,619 | 95,970 (ranked #20 in world) 616 new deaths in the last 14 days | 13 | 28.40% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Zeta/P.2 (Brazil)Delta/B.1.617.2 (India)Theta/P.3 (Philippines) Kappa/B.1.617.1 (India)Lambda/C.37 (Peru) Mu/B.1.621 (Colombia) Omicron/B.1.1.529 + BA.1 (South Africa November 2021)BA.2BA.2.12.1 (United States)BA.4 (South Africa 11/21)BA.5 (South Africa 11/21)BA.2.75 (India 7/22) | No | No |
| Mexico | 7,080,152(ranked #18) 27,224 new infections in 14 days). | 4,147 | 330,017(ranked #5)312 new deaths in 14 days) | 68 | 5.36% | No | No | |
| South Africa | 4,017,163(ranked #37; 3,113 new infections in 14 days). | 152 | 102,169 (ranked #18) 40 new deaths in 14 days) | – | 6.58% | B2 lineageAlpha/B.1.1.7 (UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Kappa/B.1.617.1 (India) C.1.2 (South Africa, July 2021)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France)BA.2BA.4 (South Africa 11/21)BA.5 (South Africa 11/21) | No | No |
| Canada | 4,233,468(ranked #33) 35,767 new infections in 14 days). | 2,477 | 44,992(ranked #24) 618new deaths in the last 14 days | 36 | 11.60% | No | No | |
| Poland | 6,268,049 (ranked #21; 61,157 new infections in 14 days). | 4,438 | 117,431 (ranked #15) | 19 | 16.60% | B2 lineageAlpha/B.1.1.7 (UK)Eta/B.1.525 (Nigeria/UK)Beta/B.1.351 (SA)Delta/B.1.617.2 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 + (South Africa November 2021),Omicron/B.1.1.529 +BA.3 | No | No |
| Russia | 20,694,894(ranked #10), 734,599 new infections in 14 days). | 53,335 (ranked #2) | 386,551(ranked #4)1,386 new deaths in 14 days | 104 | 14,16% | No | No | |
| Peru | 4,140,129(ranked #34, 16,694 new infections in 14 days). | 1,150 | 216,446(ranked #6) | 17 | 12.17% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Gamma/P.1 (Brazil)Iota/B.1.526 (USA-NYC)Lambda/C.37 (Peru)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Iran | 7,546,276(ranked #17; 8,495 new infections in last 14 days) | 421 | 144,367(ranked #12) | – | 8.73% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Omicron/B.1.1.529 + BA.1 (South Africa November 2021) | No | No |
| Spain | 13,393,196(ranked #12; 34,671 new infections in 14 days). | -(ranked #18) | 113,845(ranked #16)676 new deaths in 14 days | – | 28.61% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India)Beta/B.1.351 (SA)Gamma/P.1 (Brazil)Epsilon/B.1.427 + B.1.429 (USA)*Eta/B.1.525 (Nigeria/UK)Iota/B.1.526 (USA-NYC)Kappa/B.1.617.1 (India)Mu/B.1.621 (Colombia)Omicron/B.1.1.529 + BA.1 (South Africa November 2021)B.1.640.1 (Congo/France) | No | No |
| France | 35,050,133 (ranked #3; 367,940 new infections in the last 14 days). | 38,464 (ranked #6) | 154,854 (ranked #10) 386 new deaths in 14 days | 30 | 53.44% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)B.1.640.1 (Congo/France)B.1.640.2 (Cameroon/France)GKA (AY.4/BA.1) recombinant | No | No |
| Germany | 32,905,086(ranked #5; 452,824 new infections in 14 days.). | 50,800 (ranked #3) | 149,368 (ranked #11) 1,139 new deaths in 14 days | 93 | 39.22% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| South Korea | 24,535,940 (ranked #6 601,906 new infections in 14 days). | 39,972(ranked #8) | 28,009 (ranked #37) 628 new deaths in 14 days | 59 | 47.80% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Vietnam | 11,467,619 (ranked #13; 32,147 new infections in 14 days). | 1,928 | 43,146 (ranked #26) | – | 11.58% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Netherlands | 8,413,532 (ranked #16; 16,553 new infections in 14 days). | 1,756 | 22,633 (ranked #41) | 1 | 48.98% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Denmark | 3,097,088 (ranked #40) 7,517 new infections in 14 days | 640 | 7,021 (ranked #79) | 53.22% | 53.07% | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)GKA (AY.4/BA.1) recombinant | No | No |
| Taiwan | 6,132,744(ranked #22) 518,546 new infections in 14 days | 42,420 (ranked #4) | 10,702 (ranked #63) | 59 | 25.67% 2.17% of population has been infected in the last 14 days | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021) | No | No |
| Japan | 20,840,785(ranked #9) 958,392 new infections in the last 14 days | 61,478(ranked #1) | 44,071(ranked #25) 1,970 new deaths in the last 14 days | 120 | 16.59% 0.76% of population has been infected in the last 14 days | B2 lineageAlpha/B.1.1.7 (UK)Delta/B.1.617.2 (India) Delta/B.1.617.2 (India) Omicron/B.1.1.529 South Africa November 2021)BA.2*BA.5* | No | No |
What Our Team Is Reading This Week
- Imprinted SARS-CoV-2 humoral immunity induces converging Omicron RBD evolution (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.15.507787v2
- Note: This is a frightening paper, and if the conclusions are accurate, humans in general are in trouble. From other papers, the fact that HERV-M and EBV are activated by SARS-CoV-2 infection does not bode well for humans moving forward.
- SARS-CoV-2 Omicron boosting induces de novo B cell response in humans (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.22.509040v1
- Evolution of antibody immunity following Omicron BA.1 breakthrough infection (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.21.508922v1
- SARS-CoV-2 Spike protein promotes vWF secretion and thrombosis via endothelial cytoskeleton-associated protein 4 (CKAP4) (Signal Transduction and Targeted Therapy) https://www.nature.com/articles/s41392-022-01183-9
- Long-term neurologic outcomes of COVID-19 (Nature Medicine) https://www.nature.com/articles/s41591-022-02001-z
- Pulmonary Dysfunction after Pediatric COVID-19 (Radiology) https://pubs.rsna.org/doi/10.1148/radiol.221250
- Severe Respiratory Illnesses Associated with Rhinoviruses and/or Enteroviruses Including EV-D68 – Multistate, 2022 (CDC) https://emergency.cdc.gov/han/2022/han00474.asp
- VACCINE INFORMATION FACT SHEET FOR RECIPIENTS AND CAREGIVERS ABOUT COMIRNATY (COVID-19 VACCINE, mRNA), THE PFIZER-BIONTECH COVID-19 VACCINE, AND THE PFIZER-BIONTECH COVID-19 VACCINE BIVALENT (ORIGINAL AND OMICRON BA.4/BA.5) TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19) FOR USE IN INDIVIDUALS 12 YEARS OF AGE AND OLDER https://labeling.pfizer.com/ShowLabeling.aspx?id=14472
- Pfizer/BioNTech COVID-19 Omicron-Modified Bivalent Vaccine https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2022-09-01/07-covid-swanson-508.pdf
- Coronavirus (COVID-19) Update: FDA Authorizes Moderna, Pfizer-BioNTech Bivalent COVID-19 Vaccines for Use as a Booster Dose (FDA) https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-pfizer-biontech-bivalent-covid-19-vaccines-use
- Resistance of SARS-CoV-2 Omicron Subvariant BA.4.6 to Antibody Neutralization (Preprint) https://www.biorxiv.org/content/10.1101/2022.09.05.506628v1.full
- SARS-CoV-2 variants of concern and variants under investigation in England Technical briefing 45, 9 September 2022 (UK Health Security Agency) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1103869/Technical-Briefing-45-9September2022.pdf
- SARS CoV-2 detected in neonatal stool remote from maternal COVID-19 during pregnancy (Pediatric Research) https://doi.org/10.1038/s41390-022-02266-7
- SARS-CoV-2 variants of concern: spike protein mutational analysis and epitope for broad neutralization (Nature Communications) https://doi.org/10.1038/s41467-022-32262-8
- Is SARS-CoV-2 an oncogenic virus? (Journal of Infection) https://doi.org/10.1016/j.jinf.2022.08.005
- Emergence of immune escape at dominant SARS-CoV-2 killer T cell epitope (Cell) https://doi.org/10.1016/j.cell.2022.07.002
- Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients (The Lancet Psychiatry) https://doi.org/10.1016/S2215-0366(22)00260-7
- An Antibody from Single Human VH-rearranging Mouse Neutralizes All SARS-CoV-2 Variants Through BA.5 by Inhibiting Membrane Fusion (Science Immunology) https://doi.org/10.1126/sciimmunol.add5446
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is common in post-acute sequelae of SARS-CoV-2 infection (PASC): Results from a post-COVID-19 multidisciplinary clinic (Preprint) https://doi.org/10.1101/2022.08.03.22278363
- Evaluation of publication bias for 12 clinical trials of molnupiravir to treat SARS-CoV-2 infection in 13,694 patients (Preprint) https://www.researchsquare.com/article/rs-1913200/v1
- Anti-neuronal antibodies against brainstem antigens are associated with COVID-19 (eBioMedicine) https://doi.org/10.1016/j.ebiom.2022.104211
- Risk of SARS-CoV-2 Acquisition in Health Care Workers According to Cumulative Patient Exposure and Preferred Mask Type (JAMA Infectious Diseases) http://jamanetwork.com/article.aspx?doi=10.1001/jamanetworkopen.2022.26816
- Coronavirus spike protein activated natural immune response, damaged heart muscle cells (AHA Basic Cardiovascular Sciences Meeting) https://newsroom.heart.org/news/coronavirus-spike-protein-activated-natural-immune-response-damaged-heart-muscle-cells
- Distinguishing features of Long COVID identified through immune profiling (Preprint) https://doi.org/10.1101/2022.08.09.22278592
- Virological characteristics of the SARS-CoV-2 Omicron BA.2.75 (Preprint) https://doi.org/10.1101/2022.08.07.503115
- Multiple pathways for SARS-CoV-2 resistance to nirmatrelvir (Preprint) https://doi.org/10.1101/2022.08.07.499047
- Transmissible SARS-CoV-2 variants with resistance to clinical protease inhibitors (Preprint) https://doi.org/10.1101/2022.08.07.503099
- Comparative pathogenicity of SARS-CoV-2 Omicron subvariants including BA.1, BA.2, and BA.5 (Preprint) https://doi.org/10.1101/2022.08.05.502758
- Neuropathology and virus in brain of SARS-CoV-2 infected non-human primates (Nature Communications) https://doi.org/10.1038/s41467-022-29440-z
- SARS-CoV-2 Brain Regional Detection, Histopathology, Gene Expression, and Immunomodulatory Changes in Decedents with COVID-19 (Journal of Neuropathology and Experimental Neurology) https://doi.org/10.1093/jnen/nlac056
- Examination of SARS-CoV-2 In-Class Transmission at a Large Urban University With Public Health Mandates Using Epidemiological and Genomic Methodology (JAMA) http://jamanetwork.com/article.aspx?doi=10.1001/jamanetworkopen.2022.25430
- Antiviral treatment is more effective than smallpox vaccination upon lethal monkeypox virus infection (Nature) https://doi.org/10.1038/nature04295
- Impact of Pre-Existing Chronic Viral Infection and Reactivation on the Development of Long COVID (Preprint) https://doi.org/10.1101/2022.06.21.22276660
- Notes from the Field: Increase in Pediatric Intracranial Infections During the COVID-19 Pandemic — Eight Pediatric Hospitals, United States, March 2020–March 2022 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7131a4
- Broadly neutralizing antibodies target the coronavirus fusion peptide (Science) https://doi.org/10.1126/science.abq3773
- Efficacy and Safety of a Recombinant Plant-Based Adjuvanted Covid-19 Vaccine (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMoa2201300
- Efficacy and Safety of the RBD-Dimer–Based Covid-19 Vaccine ZF2001 in Adults (NEJM) https://www.nejm.org/doi/full/10.1056/NEJMoa2202261
- Risk of Reinfection, Vaccine Protection, and Severity of Infection with the BA.5 Omicron Subvariant: A Danish Nation-Wide Population-Based Study (Preprint) https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4165630
- SARS-CoV-2 Omicron BA.5: Evolving tropism and evasion of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. (Preprint) https://doi.org/10.1101/2022.07.07.22277128
- Brain imaging and neuropsychological assessment of individuals recovered from mild to moderate SARS-CoV-2 infection (Preprint) https://doi.org/10.1101/2022.07.08.22277420
- Increased Risk of Herpes Zoster in Adults ≥50 Years Old Diagnosed With COVID-19 in the United States (Open Forum Infectious Diseases) https://doi.org/10.1093/ofid/ofac118
- Neutralization sensitivity of Omicron BA.2.75 to therapeutic monoclonal antibodies (Preprint) https://doi.org/10.1101/2022.07.14.500041
- Neutralizing antibody activity against 21 SARS-CoV-2 variants in older adults vaccinated with BNT162b2 (Nature Microbiology) https://doi.org/10.1038/s41564-022-01163-3
- How COVID-19 affects microvessels in the brain (Brain) https://doi.org/10.1093/brain/awac211
- Fine Analysis of Lymphocyte Subpopulations in SARS-CoV-2 Infected Patients: Differential Profiling of Patients With Severe Outcome (Frontiers in Immunology) https://doi.org/10.3389/fimmu.2022.889813
- SARS-CoV-2 accelerated clearance using a novel nitric oxide nasal spray (NONS) treatment: A randomized trial (The Lancet Regional Health – Southeast Asia) https://doi.org/10.1016/j.lansea.2022.100036
- Effectiveness of 2, 3, and 4 COVID-19 mRNA Vaccine Doses Among Immunocompetent Adults During Periods when SARS-CoV-2 Omicron BA.1 and BA.2/BA.2.12.1 Sublineages Predominated — VISION Network, 10 States, December 2021–June 2022 (MMWR) http://dx.doi.org/10.15585/mmwr.mm7129e1
- Characterization of virologic rebound following nirmatrelvir-ritonavir treatment for COVID-19 (Clinical Infectious Diseases) https://doi.org/10.1093/cid/ciac512
- Potential Autoimmunity Resulting from Molecular Mimicry between SARS-CoV-2 Spike and Human Proteins (Preprint) https://doi.org/10.1101/2021.08.10.455737
- COVID-19 positive patients at higher risk of developing neurodegenerative disorders, new study shows (Medical Express) https://medicalxpress.com/news/2022-06-covid-positive-patients-higher-neurodegenerative.html
- Evidence of previous SARS-CoV-2 infection in seronegative patients with long COVID (eBioMedicine) https://doi.org/10.1016/j.ebiom.2022.104129
- SARS-CoV-2 infection induces inflammatory bone loss in golden Syrian hamsters (Nature Communications) https://doi.org/10.1038/s41467-022-30195-w
- Persistent 129Xe MRI Pulmonary and CT Vascular Abnormalities in Symptomatic Individuals with Post-Acute COVID-19 Syndrome (Radiology) https://doi.org/10.1148/radiol.220492
- ACE2-independent infection of T lymphocytes by SARS-CoV-2 (Signal Transduction and Targeted Therapy) https://doi.org/10.1038/s41392-022-00919-x
- Persistent circulating SARS-CoV-2 spike is associated with post-acute COVID-19 sequelae (Preprint) https://doi.org/10.1101/2022.06.14.22276401
- SARS-CoV-2 is detected in the gastrointestinal tract of asymptomatic endoscopy patients but is unlikely to pose a significant risk to healthcare personnel (Gastro Hep Adv) https://doi.org/10.1016/j.gastha.2022.06.002
- Long COVID symptoms in SARS-CoV-2-positive children aged 0–14 years and matched controls in Denmark (LongCOVIDKidsDK): a national, cross-sectional study (Child & Adolescent Health) https://doi.org/10.1016/S2352-4642(22)00154-7
- Age and sex-specific risks of myocarditis and pericarditis following Covid-19 messenger RNA vaccines (Nature Communications) https://doi.org/10.1038/s41467-022-31401-5
- COVID-19 positive patients at higher risk of developing neurodegenerative disorders, new study shows https://medicalxpress.com/news/2022-06-covid-positive-patients-higher-neurodegenerative.html
- Posttranslational modifications optimize the ability of SARS-CoV-2 spike for effective interaction with host cell receptors (Biophysics and Computational Biology) https://doi.org/10.1073/pnas.2119761119
- Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2 (The Lancet) https://doi.org/10.1016/S0140-6736(22)00941-2
- Antibody escape of SARS-CoV-2 Omicron BA.4 and BA.5 from vaccine and BA.1 serum (Cell) https://doi.org/10.1016/j.cell.2022.06.005
- Immunomodulatory treatment in postural tachycardia syndrome: A case series (European Journal of Neurology) https://doi.org/10.1111/ene.14711
- Long COVID-19 Liver Manifestation in Children (JPGN) https://journals.lww.com/jpgn/abstract/9900/long_covid_19_liver_manifestation_in_children.84.aspx
- Cross-reactive immunity against the SARS-CoV-2 Omicron variant is low in pediatric patients with prior COVID-19 or MIS-C (Nature Communications) https://doi.org/10.1038/s41467-022-30649-1
- C.D.C. Dismisses Airborne Transmission of Monkeypox. Some Experts Disagree. (NY Times) https://www.nytimes.com/2022/06/10/health/monkeypox-airborne.html
- Omicron BA.1 breakthrough infection drives cross-variant neutralization and memory B cell formation against conserved epitopes (Science Immunology) https://doi.org/10.1126/sciimmunol.abq2427
- SARS-CoV-2 Infection and Persistence Throughout the Human Body and Brain (National Institutes of Health) https://videocast.nih.gov/watch=45296?jwsource=twi
- Long COVID is associated with extensive in-vivo neuroinflammation on [18F]DPA-714 PET (Preprint) https://doi.org/10.1101/2022.06.02.22275916
- Unexpected worsening of progressive multifocal leucoencephalopathy following COVID-19 pneumonia (Journal of Neurovirology) https://doi.org/10.1007%2Fs13365-021-00980-2
- Virological characteristics of the novel SARS-CoV-2 Omicron variants including BA.2.12.1, BA.4 and BA.5 (Preprint) https://doi.org/10.1101/2022.05.26.493539
- During the Omicron Wave, Death Rates Soared for Older People (NY Times with CDC data) https://www.nytimes.com/2022/05/31/health/omicron-deaths-age-65-elderly.html
- PD-1 blockade counteracts post–COVID-19 immune abnormalities and stimulates the anti–SARS-CoV-2 immune response (JCI Insight) https://insight.jci.org/articles/view/146701
- Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance (Nature Reviews Clinical Oncology) https://doi.org/10.1038/s41571-019-0218-0
- Herpesvirus infections and post-COVID-19 manifestations: a pilot observational study (Observational Research) https://doi.org/10.1007/s00296-022-05146-9

You must be logged in to post a comment.