
It’s time for our next 14-day moving average determinations and projections for infections and deaths from SARS-CoV-2 for the United States and my thoughts on vaccines and mutant viruses. We use the WORLDOMETERS aggregators data set to make our projections of future total infections and deaths since it includes data from the Department of Veterans Affairs, the U.S. Military, federal prisons and the Navajo Nation.
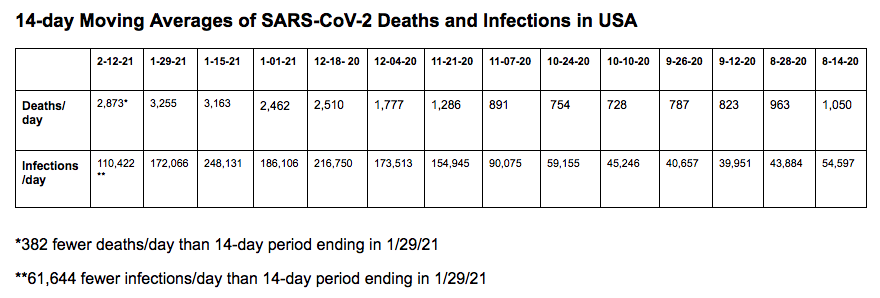
In the United States, SARS-CoV-2 deaths have decreased for the first time since the last 14-day period. There were 382 fewer deaths per day than in the last 14-day period. In the last 14 days, the number of infections has decreased by 61,644 infections per day. This decrease in infections over the last two 14-day periods may represent increased mask usage and social distancing, which are a part of the Biden 100-day SARS-CoV-2 plan. On 2/12/21, 100,288 new infections occurred in the United States. There were also 2,908 deaths. The number of hospitalized patients is decreasing, and only 19,927 patients are critically ill. The number of critically ill patients has decreased by 4,561 in the last 14 days, while 40,216 new deaths occurred. This suggests that the number of critically ill patients is decreasing because a large number of patients are dying.
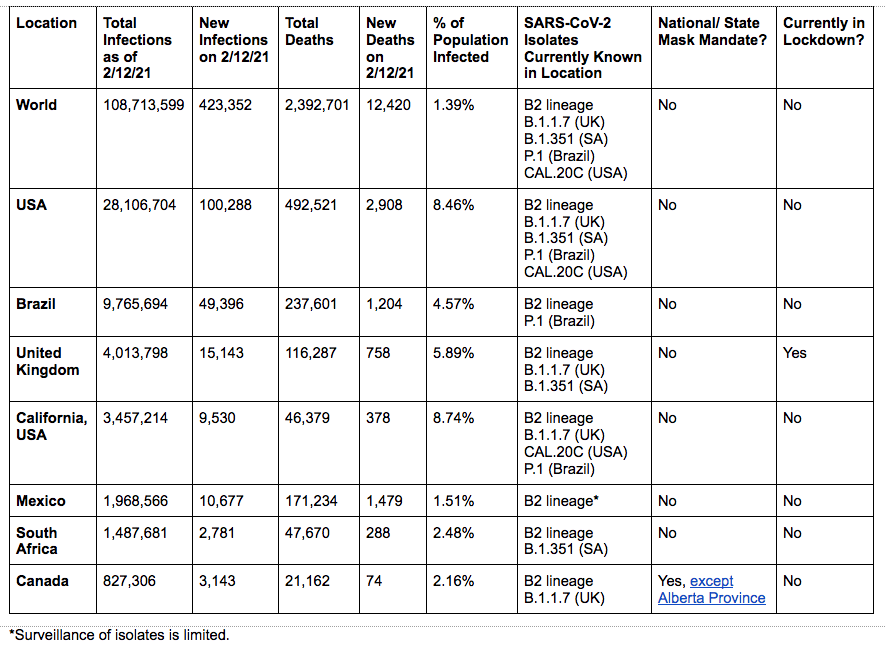
As of 2/12/21, we have had 492,521 deaths and 28,106,704 SARS-CoV-2 infections in the United States. We have had 1,545,917 new infections in the last 14 days. We are adding 772,958 infections every 7 days. Each million infections usually results in at least 20,000 deaths. On 2/12/21, eighteen states have had greater than 500,000 total infections, and 28 states had greater than 5,000 total deaths.
On 11/20/20 in the United States, 3.70% of the population had a documented SARS-CoV-2 infection. California was ranked 41st in infection percentage at 2.77%. In North Dakota 9.18% of the population was infected (ranked #1), and in South Dakota 8.03% of the population was infected (ranked #2).
As of 2/12/21, in the United States 8.46% of the population has had a documented SARS-CoV-2 infection. California was ranked 25th in infection percentage at 8.74%. In North Dakota 12.92% of the population was infected (ranked #1) and in South Dakota 12.44% of the population was infected (ranked #2). Ten states have greater than 10% of their population infected: North Dakota, South Dakota, Iowa, Nebraska, Arizona, Utah, Tennessee, Oklahoma, Arkansas, and Rhode Island. Only six states have less than 6% of their population infected: New Hampshire (5.51%), Washington (4.33%), Oregon (3.54%), Maine (3.14%), Vermont (2.15%), and Hawaii (1.88%).
New Mutants
A new mutant SARS-CoV-2 virus (lineage B.1.1.7), first seen in the UK in September, has now been found in multiple other countries. There are 981 reported cases in the US as of 2/11/21. This isolate has now been found in over 37 states. This isolate (let’s call it Lineage B.1.1.7 or SARS-CoV-2 UK) is more infectious than other previously circulating B2 lineage isolates (probably 30 to 40% increased infectivity). There are two deletions and six other mutations in its spike protein. One mutation involves a change of one amino acid, an asparagine at position 501 in the receptor binding motif with a tyrosine. This enhances binding (affinity) to the ACE-2 receptor and may alone be responsible for the increased infectivity of this isolate. Due to air and other travel, this isolate will become the dominant isolate worldwide.
B.1.351, also known as the South African isolate, has 13 reported cases and has occurred in 5 states: South Carolina, North Carolina, Virginia, Maryland, and California. The P.1 isolate (Brazil) has 3 reported cases and has been found in Minnesota and Oklahoma. (This data is available at https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant-cases.html.)
A new, disturbing report out of the UK has found a second mutation in B.1.1.7. This mutation, which occurs in the loop sequence has also been found in the South African (B.1.351) and Brazilian (P.1) variants. (The loop sequence is in the receptor binding motif in the receptor binding domain of the S1 sequence of the spike protein.) This mutation involves a change of one amino acid of the spike protein, number 484, from glutamic acid to lysine. This point mutation allows the virus to bind better to the ACE2 receptor, which increases infectivity. People who are exposed to one of these variants (verus the old B2 isolate) are more likely to be infected and are more likely to transmit the virus to others.
In our last update we summarized a research letter published in Clinical Infectious Diseases about a patient in the UK who was first infected in April with a B2 isolate and experienced only mild symptoms but was infected with the new B.1.1.7 variant in December and became critically ill. The patient described in this research letter was not protected by a natural infection with a B2 lineage SARS-CoV-2 isolate in April 2020 from having a potentially lethal second infection with a B.1.1.7 lineage variant in December 2020, suggesting that folks who have had a past SARS-CoV-2 infection should not expect to have any immunity to new variants such as B.1.1.7. All of the currently available vaccines were developed with spike protein from B2 lineages. Moderna, Pfizer, and AstraZeneca/Oxford are currently remaking their spike protein vaccines to address the mutations in the South African variant of SARS-CoV-2 because the AstraZeneca/Oxford vaccine did not work in a small trial in South Africa, where most of the patients had the South African mutant (B.1.351).
A California Mutant
A fourth mutant isolate (CAL.20C) of SARS-CoV-2 has been identified in California. This isolate does not have any of the mutations mentioned above, but contains five mutations, three of which are in the spike protein, but not in the receptor binding motif. This mutant appears to be responsible for the massive increase in infections in California, to include infections of people who had already recovered from a SARS-CoV-2 infection earlier. In California, we have had 3,457,214 infections, 46,379 total deaths, and 6,533 deaths in the last 14 days. California is averaging 466 deaths per day in the last 14 days. Currently, 8.3% of the population in California is infected. Nationally, we rank 25th in the percentage of people in the state infected. To my knowledge, no company is currently modifying their vaccines to cover the CAL.20C (California) mutant.
Watching the Data
Over the next few months, we’ll be paying close attention to correlations between the SARS-CoV-2 data, the number of isolates identified in various countries and states, and the non-pharmaceutical interventions (like mask mandates and lockdowns) put in place by state and national governments.
The Road Ahead
We have a new President and Vice President. The President has made the pandemic a first priority. Testing, wearing masks, social distancing and washing our hands frequently should no longer be political issues. These are non-pharmaceutical interventions used by most successful countries and some states to protect their citizens and their economies. New Zealand, Taiwan, and Australia are three countries that have done this successfully. In the United States, Vermont and Hawaii are doing a better job handling the pandemic than many of our states. The pandemic problem is overwhelming our health care delivery system in many states.
The Pfizer and Moderna RNA vaccines are both now approved in the USA. The Johnson & Johnson and Novavax vaccines are pending approval. To vaccinate 80% of our population with two doses of vaccine, we will need over 500 million doses of vaccine. The current goal of the Biden administration in the US is to vaccinate one million people each day for 100 days. At this rate, to vaccinate 280 million people it would take 280 days—more than 9 months. The good news is this week, on one day, 2 million vaccinations occurred. If this pace were to continue we could vaccinate everyone who wanted a vaccine in the USA in less than five months.
All current vaccines are based on the Chinese spike protein sequence from December 2019. Mutated isolates, as discussed above, may overtake our ability to produce vaccines and vaccinate the populace. Like Influenza vaccines, we may have to reformulate vaccines based on active, worldwide surveillance every 6 to 8 months. The FDA is currently putting together a guidance document for how to develop booster vaccines for SARS-CoV-2 mutations. We need to perform more virus isolations and perform more DNA sequencing of viruses in each country, state, populous city, and county if we are to rapidly identify new mutations. I’m more hopeful that we will have the facilities, the equipment, and the trained staff needed to perform this work. As a nation we are finally preparing to make more vaccine, new vaccines directed against mutants, and the necessary rapid tests and protective equipment needed by medical staff, first responders, and especially teachers and students. I’m hopeful we can work together on our and the world’s problems.

You must be logged in to post a comment.